Kamalakshi Pandurangan College of Pharmacy, Ayyampalyam, Tiruvannamalai
Thyroid disorders are a worldwide, most prevalent endocrine diseases. It is a group of conditions affecting the thyroid gland's function, are widespread globally, with over 42 million people affected in India alone. These disorders can manifest as either underactive (hypothyroidism) or overactive (hyperthyroidism) thyroid. It significantly impacts the metabolism, growth, and overall health of the human body. This review article’s main goal is to provide a comprehensive overview of anatomy and physiology of the thyroid gland, the various types of thyroid disorders including hypothyroidism, hyperthyroidism, thyroid cancer, goiter, thyroiditis, thyroid disorders in pregnancy as well as their etiology, risk factors, clinical manifestations, diagnostic approaches, and management strategies. Understanding the pathophysiology of these disorders is crucial for early detection and effective treatment. The article further explores the role of genetic and environmental factors in the development of thyroid conditions, the advancements in diagnostic techniques, and the latest therapeutic interventions. Additionally, it highlights the importance of early intervention and the impact of thyroid dysfunction on quality of life, particularly in vulnerable populations such as pregnant women and the elderly. By consolidating current research and clinical practices, this review aims to contribute to a more thorough understanding and better management of thyroid disorders.
The thyroid gland, a small butterfly-shaped organ located in the neck, plays a crucial role in regulating various metabolic processes in the body. It mainly produces two thyroid hormones- thyroxine (T?) and triiodothyronine (T?),which control the body's metabolism, growth, and energy expenditure [1]. Dysregulation of thyroid function can lead to a wide range of disorders, including hypothyroidism, hyperthyroidism, goiter, thyroid cancer, and autoimmune conditions like Hashimoto’s thyroiditis [2]. These disorders can significantly affect an individual’s health, quality of life, and productivity [3]. The growing prevalence of thyroid disorders, coupled with their multifactorial etiology, makes early detection and timely intervention vital [4]. Thyroid disorders are not only common in the general population but are also prevalent in specific vulnerable groups, including pregnant women and the elderly. The pharmacist plays a key role in managing these disorders, as they are often involved in the dispensing of medication, patient counseling, and ensuring compliance with therapeutic regimens[5]. This article aims to provide a comprehensive overview of thyroid disorders, focusing on their etiology, clinical manifestations, diagnostic approaches, and management strategies, while emphasizing the role of the pharmacist in effective disease management.
ANATOMY OF THE THYROID GLAND
The thyroid is a small butterfly-shaped gland located at the front, base of the neck[6]. It consists of two lobes that are connected by a thin tissue, known as the isthmus, and are comprised of cells called ‘thyroid follicles’[6]. The primary function of the thyroid is the synthesis and release of two main thyroid hormones--tri-iodothyronine (T3) and the relatively inactive prohormone tetra-iodothyronine (T4), which is more commonly known as thyroxine[7].T3 and T4 secretion is regulated by thyroid-stimulating hormone (TSH), which, in turn, is regulated by thyrotrophin-releasing hormone (TRH), produced by the anterior pituitary gland and the hypothalamus, respectively[8]. The thyroid is one of the largest endocrine glands which is located in the neck, just below the larynx. It is made of two lateral lobes, right and left, connected by a central isthmus, with occasionally an accessory pyramidal lobe discernible as a finger-like projection directed upward from the isthmus.The parathyroid glands are located behind the thyroid gland which involved in calcium metabolism[9].
PHYSIOLOGY OF THYROID GLAND
The thyroid gland’s main function is to produce thyroid hormones thyroxine (T4) and triiodothyronine (T3), homodimer peptides derived from the iodination and coupling of the amino acid L-tyrosine. Thyroxine is a multifunctional hormone, which helps in the metabolism of carbohydrate, proteins and lipids. It maintains the Body Mass Ratio (BMR) and also the heat regulation of the body [10]. It plays a vital role in the growth and development of various organs. The hypothalamo, hypophyseal-thyroid axis mainly regulates the thyroxin secretion. The major diseases associated with thyroid gland, hyper and hypo thyroidism is due to increased or decreased secretion of the hormones respectively.
Synthesis of triiodothyronine and tetraiodothyronine is shown below:
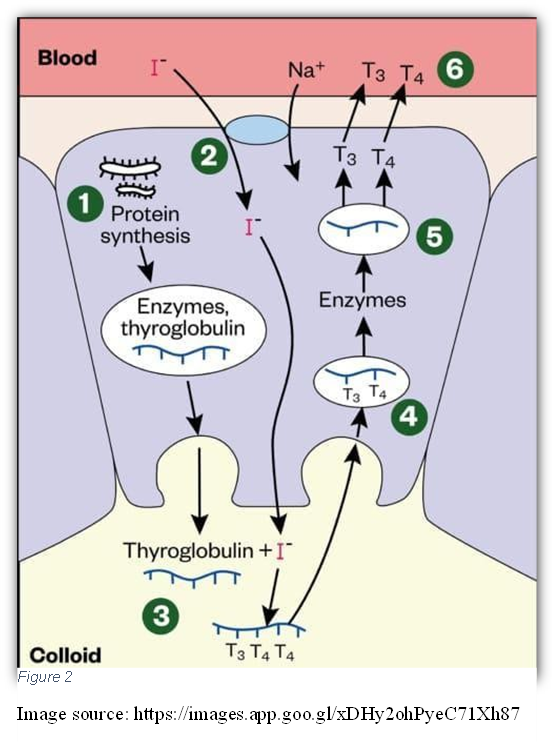
Role of Thyroid Hormones:
In times of increased metabolic rate or when circulating levels of T3 and T4 are low, TRH and TSH stimulate the release of T3 and T4 into the bloodstream [6]. Around 80% of this will be T4 and only 10% will be the active T3, as T3 has a short half-life of 24–36 hours, in comparison to that of T4, which has a half-life of 6–7 days [7].
Regulation by the Hypothalamic-Pituitary-Thyroid Axis:
The synthesis and release of thyroid hormones are controlled by the hypothalamic-pituitary- thyroid axis. The hypothalamus releases thyrotropin-releasing hormone (TRH), which stimulates the pituitary to secrete thyroid-stimulating hormone (TSH). TSH then activates the thyroid gland to produce T? and T?. This process is regulated through negative feedback, where high levels of thyroid hormones inhibit the release of TRH and TSH, thus maintaining homeostasis [13]. TSH production is regulated by two interacting systems. They are,
THYROID HORMONE REGULATIONS[14]
Thyroid Hormone activity is regulated at multiple steps; however, the primary point of regulation is synthesis of thyroid hormones by the thyroid gland. Here we study the basic circuitry which governs the release of thyroid hormone by the thyroid gland.
Overview: Thyroid Hormone release is regulated by an extended version of the circuit that governs Basic Hypothalamic-Pituitary Coordination.
Hypothalamic Step: The hypothalamus releases Thyrotropin-releasing Hormone (TRH) which acts on the anterior pituitary. It should be pointed out that TRH is also involved in the regulated release of prolactin.
Pituitary Step: Being stimulated by TRH, the anterior pituitary synthesizes and secretes Thyroid Stimulating Hormone (TSH) which acts directly on the thyroid gland.
Thyroid Step: The thyroid gland releases thyroid hormones by the stimulation of TSH.
Tissue Step: The thyroid gland mostly releases T4 which does not possess much endocrine activity. Target tissues possess the enzyme Iodinase that converts T4 to either T3 or rT3. T3 possesses tremendously more endocrine activity than T4 whereas, rT3 does not possess any endocrine activity. Therefore, in reality, the final step of the thyroid hormone regulatory axis can be occured in the actual peripheral target tissues as shown in the Figure.3
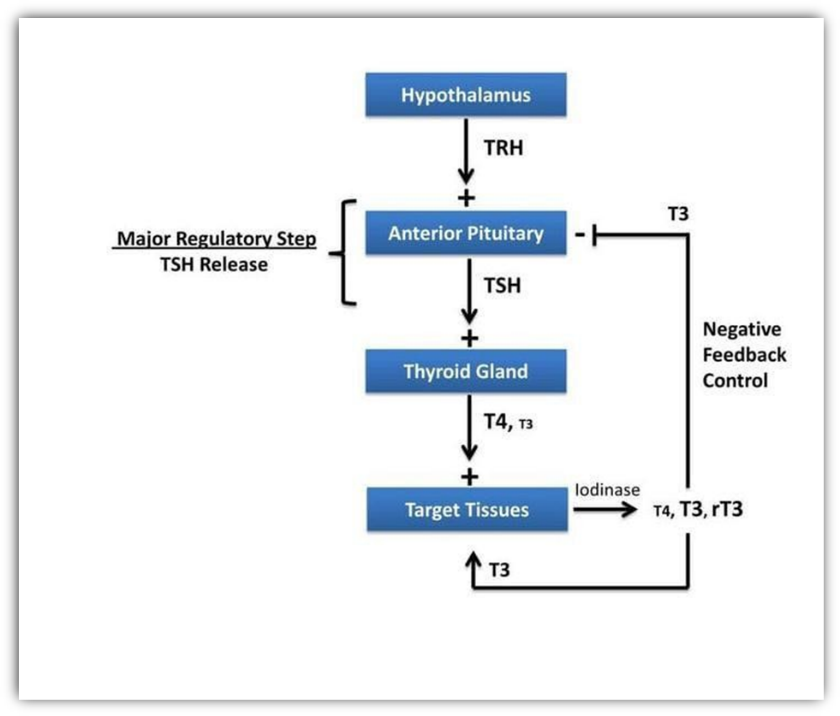
Figure 3
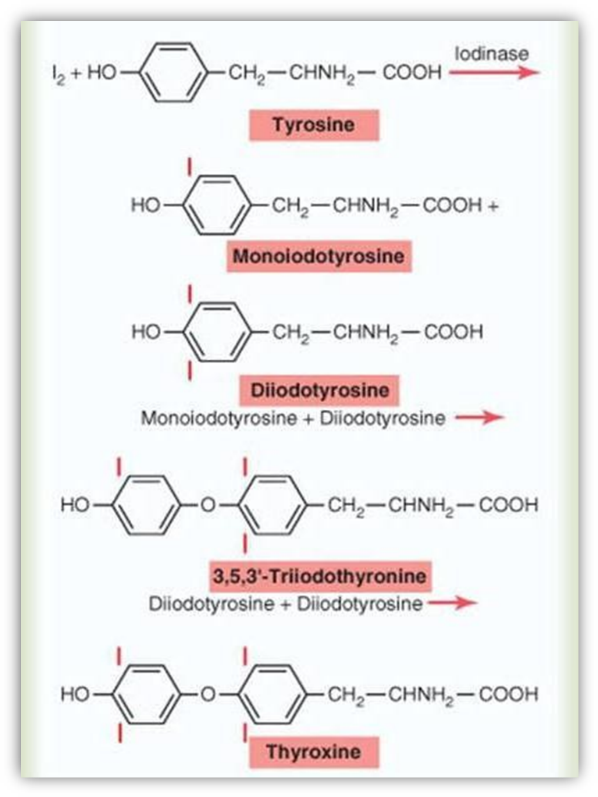
CHEMICAL STRUCTURE OF THYROID HORMONES
Thyroid hormones play a major role in the development and functional maintenance of many organs [15]. They are a group of hormones synthesized and secreted from the thyroid gland, which is located in front of the trachea, below the thyroid cartilage. In general, two compounds, thyroxine (3, 5, 3', 5' -tetra-iodo-L-thyronine, T4) and triiodothyronine (3, 5, 3' -tri-iodo-L- thyronine, T3), are considered thyroid hormones. In addition, another compound called reverse T3 (3, 3', 5' -tri-iodo-L-thyronine, rT3) is secreted from the thyroid gland. Their chemical structures are shown in Figure 4 .The essential molecular structure comprises two iodinated benzene rings connected by ether linkage. T4 is the major hormone secreted from the thyroid gland, whereas the other hormones are mainly generated by the deiodination of T4 in extrathyroidal tissues. The ratio of the secretion of T4:T3:rT3 from the thyroid gland is approximately 100:5:2.5. T3, a bioactive thyroid hormone, is mainly produced by the deiodination of T4 in thyroid hormone target tissues [14].
VARIOUS DISORDERS OF THYROID GLAND
HYPOTHYROIDISM[16,17]
Description: A condition where the thyroid gland doesn't produce enough thyroid hormones.
Causes: Autoimmune diseases (e.g., Hashimoto’s thyroiditis), iodine deficiency, thyroid surgery, radiation therapy.
Symptoms: Fatigue, weight gain, cold intolerance, constipation, depression, dry skin.
Types:
HYPERTHYROIDISM[18,19]
Description: Excessive secretion of thyroid hormones.
Causes: Graves’ disease, toxic multinodular goiter, thyroiditis.
Symptoms: Weight loss, heat intolerance, palpitations, tremors, anxiety, goiter.
GOITER[20]
Description: Enlargement of the thyroid gland.
Symptoms: Neck swelling, compressive symptoms (if large), sometimes euthyroid.
Types:
THYROID NODULES[21]
Description: Solid or fluid-filled lumps within the thyroid.
Evaluation: Ultrasound, fine-needle aspiration (FNA).
Types:
THYROID CANCER[22]
Description: Thyroid cancer is the abnormal growth of cells in the thyroid gland, often presenting as a painless thyroid nodule.
Symptoms: Hard nodule, rapid growth, hoarseness, lymphadenopathy.
Types:
THYROIDITIS[23]
Description: Thyroiditis is inflammation of the thyroid gland that can cause temporary hyperthyroidism followed by hypothyroidism.
Symptoms: Thyroid pain (in subacute), phases of hyper- then hypothyroidism.
Types:
THYROID DISORDERS IN PREGNANCY[24]
Description: Thyroid disorders during pregnancy can affect both maternal and fetal health. Proper management is essential to prevent complications like miscarriage, preterm birth, and impaired neurodevelopment in the fetus.
Types:
Hypothyroidism
Description: Inadequate thyroid hormone production, often due to Hashimoto’s thyroiditis.
Symptoms: Fatigue, constipation, weight gain, cold intolerance.
Types:
Risks: Miscarriage, preterm birth, impaired fetal development.
Hyperthyroidism
Description: Excess thyroid hormones, usually from Graves’ disease.
Symptoms: Palpitations, weight loss, tremors, anxiety.
Types:
Risks: Preterm labor, fetal growth restriction, maternal complications.
Postpartum Thyroiditis
Description: Autoimmune thyroid inflammation occurring within one year postpartum.
Symptoms:
Types: Biphasic or monophasic.
Outcome: Often self-limiting, may cause long-term hypothyroidism.
HYPOTHYROIDISM
Definition:
Hypothyroidism is a disorder that occurs when the thyroid gland does not make enough thyroid hormone to meet the body’s requirements. Thyroid hormone regulates metabolism (the way the body uses energy) and affects nearly every organ in the body. Without enough thyroid hormone, many of the body’s functions slow down. [25]
Hypothyroidism is a condition in which the thyroid gland does not produce enough Thyroid hormone, often requiring pharmacological management. Pharmacists should be able to recognise and treat the condition as they may provide direct patient care in both primary and secondary settings.
Classification of Hypothyroidism [26]
Hypothyroidism can be classified based on the site of dysfunction and onset:
Based on Site of Dysfunction:
Common causes: Hashimoto’s thyroiditis, iodine deficiency, post-thyroidectomy.
Often due to pituitary tumors, surgery, or radiation.
Based on Onset:
ETIOLOGY OF HYPOTHYROIDISM [27]
Hypothyroidism has several causes, including
Less commonly, hypothyroidism is caused by too much or too little iodine in the diet or by abnormalities of the pituitary gland.
This is the most common cause of hypothyroidism in many countries. It’s an autoimmune disease—the immune system attacks the thyroid gland. This causes inflammation and reduces hormone production. It is also called chronic lymphocytic thyroiditis.
Thyroiditis causes stored thyroid hormones to leak, first leading to hyperthyroidism, then hypothyroidism.
Types:
Some babies are born with an underdeveloped or non-functioning thyroid. If not treated early, it can lead to mental and growth problems. That’s why newborn screening is done in many countries.
If part of the thyroid is removed, hormone levels may stay normal. But if the entire thyroid is removed (due to goiter, cancer, or nodules), it causes permanent hypothyroidism.
Used to treat hyperthyroidism or cancers of the head and neck. Destroys thyroid cells, leading to reduced hormone production.
Some medicines can reduce thyroid hormone levels:
SYMPTOMS OF HYPOTHYROIDISM [27,28]
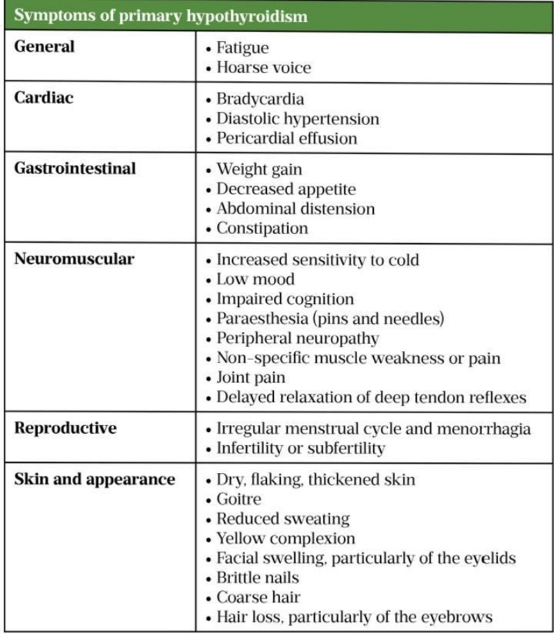
Hypothyroidism has many symptoms that can vary from person to person. Some common symptoms of hypothyroidism are
However, hypothyroidism develops slowly, so many people don’t notice symptoms of the disease. Symptoms more specific to Hashimoto’s disease are a goiter and a feeling of fullness in the throat. Hypothyroidism can contribute to high cholesterol, so people with high cholesterol should be tested for hypothyroidism. Rarely, severe, untreated hypothyroidism may lead to myxedema coma, an extreme form of hypothyroidism in which the body’s functions low to the point that it becomes life threatening. Myxedema requires immediate medical treatment.
DIAGNOSIS OF HYPOTHYROIDISM [27]
Doctor asks about your health history and symptoms.Then, they do a physical exam.
To confirm if you really have hypothyroidism and to find out the cause, doctors do the following tests:
b. T4 Test (Thyroxine):
This checks the level of actual thyroid hormone in your blood. In hypothyroidism, T4 levels are lower than normal.
This test checks if your immune system is attacking your thyroid (as in Hashimoto’s disease). People with Hashimoto’s usually have these antibodies. If no antibodies are found, the cause may be something else.
TREATMENT OF HYPOTHYROIDISM
Usually hypothyroidism is treated using a medicine called synthetic thyroxine (T4). This medicine works just like the natural thyroid hormone that human body makes.
The dose of thyroxine depends on:
After starting the medicine, doctors check your TSH levels in the blood after 6 to 8 weeks. Based on the results, they may adjust the dose. Each time the dose is changed, your blood will be tested again.
Once the right dose is found, blood tests are done:
Hypothyroidism can be completely controlled with this medicine—as long as you take it daily as prescribed.
SIDE EFFECTS OF LEVOTHYROXINE [29]
These symptoms may mean:
Rare but Serious Side Effects:
What to do:
DIET AND NUTRITION IN HYPOTHYROIDISM[30]
Balanced Diet:
People with hypothyroidism should eat a well-balanced diet to get all the essential nutrients.
Iodine and Supplements:
Iodine is important for making thyroid hormones.But people with autoimmune thyroid diseases (like Hashimoto’s) should be careful. Too much iodine (from seaweed, kelp, or iodine drops) can worsen thyroid problems.
Pregnancy and Iodine:
Pregnant women need about 250 micrograms of iodine daily. The baby depends on the mother’s iodine intake for thyroid hormone development. Around 7% of pregnant women in the U.S. don’t get enough iodine.
Tips for Adequate Iodine Intake:
Using of iodized salt instead of plain salt. Taking prenatal vitamins that contain iodine (during pregnancy).
REFERENCES





Abinesh, Deepika, Dheena, V. Senthilkumar, Dr. D. Rajalingam, Dr. N. Gnanasekar, A Review Article on Hypothyroidism, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 5407-5418. https://doi.org/10.5281/zenodo.15758000
 10.5281/zenodo.15758000
10.5281/zenodo.15758000
