M.A.M College of Pharmacy, Kesanupalli, Narasaraopeta (522601), Palnadu District, Andhra Pradesh.
Sleep is a vital neurological function that plays a crucial role in rest and restoring energy. Its significance is evident in the fact that people spend nearly one-third of their lives asleep. Alterations in sleep patterns, duration, or consistency can result in sleep disturbances, which, when persistent, negatively impact overall health and well-being. Sleep is broadly divided into two physiological and behavioral states: Non-Rapid Eye Movement (NREM) sleep—which includes four distinct stages—and Rapid Eye Movement (REM) sleep, which features muscle paralysis and a desynchronized EEG pattern. The sleep-wake cycle is controlled by the circadian rhythm, regulated by the suprachiasmatic nuclei in the hypothalamus. Common sleep-related problems include excessive daytime sleepiness, insomnia, irregular sleep behaviors, and delayed sleep onset. Diagnostic tools such as overnight polysomnography and the multiple sleep latency test are essential for identifying sleep disorders. This article will explore the epidemiology, causes, clinical features, types, diagnostic approaches, and treatment options for various sleep disorders.
Definition Of the Sleep
Sleep is a functional state that involves a variety of physiological and behavioral processes [1]. It is distinguished by a relative unconsciousness of the outside environment, a decrease in voluntary body movement, and a general lack of memory of the state [2].
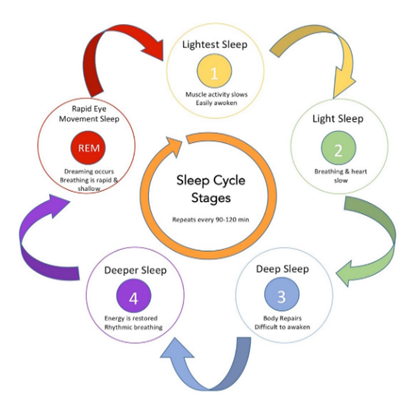
Sleep Cycle
Based on three physiological measurements electroencephalography (EEG), electrooculogram (EOG) and electromyography (EMG), sleep is categorized into two distinct states: rapid eye movement (REM) and non-rapid eye movement (NREM). The initial sleep cycle is often the shortest, lasting 70 to 100 minutes, while subsequent cycles last between 90 and 120 minutes [3].
NREM Sleep Patterns: NREM sleep is composed of three different stages.
REM Sleep Patterns: Dreaming occurs during the REM phase of sleep. It is distinguished by entire body voluntary muscular paralysis (with the exception of the extraocular muscles) This paralysis is hypothesized to be a mechanism that prevents neural stimuli from dreams from manifesting as actual muscle when asleep. The EEG in REM consists of ‘sawtooth waveforms,” theta waves, and slow, alpha waves in a desynchronized pattern [5].
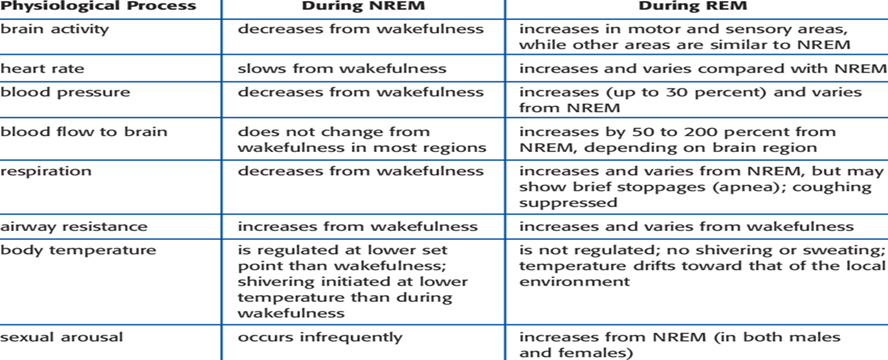
Physiological Chanes During Sleep
Various physiological and behavioral changes occur during normal waking, NREM sleep and REM sleep listed in (Table 1).
Table-1: Physiological Changes During Sleep
Many hormones have substantial connections with sleep-wake cycles. Growth hormone secretion increases in a pulsatile manner during NREM sleep in the initial third of the typical sleep period. Prolactin secretion rises 30 to 90 minutes after sleep onset, while sleep inhibits cortisol secretion. Thyroid-stimulating hormone secretion peaks in the evening and declines throughout the night. Testosterone levels in men increase during sleep, reaching peak levels at 0800 h, with no clear link found between gonadotropic hormones and the sleep-wake cycle in children or adults. Melatonin, released by the pineal gland, peals between 0300 h and 0500h, decreasing to low levels during the day. Body temperature to decline at sleep onset, reaching its lowest point during third sleep cycle. Penile erection and clitoral tumescence occur during REM sleep [6].
Circadian Rhythms, The 24-Hour Clock
Circadian rhythms are daily patterns in physiology and behaviour, governing sleep, activity, food intake, and regulating body functions like temperature and hormone release. These rhythms originate from neural structures in the hypothalamus, acting as a biological clock Sleep-wake regulation involves the balance between increasing sleep drive throughout the day and circadian rhythms promoting wakefulness. As the day progresses, sleep drive rises, leading to sleep onset, while in the morning, reduced sleep drive and circadian arousal contribute to awakening [7].
Sleep Disorders
A sleep disorder, or somnipathy, is a medical condition that disrupts an individual’s sleep patterns, impacting their physical, mental, social, and emotional functioning, often leading to serious consequences for health and overall quality of life [8].
Epidemiology
TYPES OF SLEEP DISORDERS
The American Academy of Sleep Medicine developed the ICSD-2 to standardize definitions and implement a systematic diagnostic approach in the realm of sleep disorders [14]. These conditions are primarily categorized in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV).
Also known as sleeplessness, is a sleep disorder causing difficulty in either falling asleep or staying asleep as desired [15].
Etiology:
Heart failure, Hyperthyroidism, Heartburn, Restless leg syndrome, Psychological stress.
Symptoms:
Trouble sleeping, Depressed mood, Low energy, Daytime sleepiness.
It is a neurological condition characterizes by either prolonged periods of sleep or excessive drowsiness [16].
Etiology:
Parkinson’s disease, Alzheimer’s disease, Upper airway resistance syndrome
Symptoms:
Excessive daytime sleepiness, Sleep drunkenness [17].
Narcolepsy is a long-term Neurological condition characterized but difficulty in controlling sleep and wakefulness patterns.
Etiology:
Orexin deficiency, genetic factors
Symptoms:
Excessive daytime sleepiness, Involuntary sleep episodes, hallucinations [18].
CRSD refer to a group of sleep disorders that impact the timing of sleep. Also known as Circadian Rhythm Sleep Wake Disorder
Etiology:
Jet lag syndrome, Night shift work.
Symptoms:
Excessive day time sleepiness, decreased alertness [19].
Sleep disturbances caused by breathing disorders like Obstructive or Central Sleep Apnoea or Central Alveolar Hyperventilation result in either excessive sleepiness or insomnia
Etiology:
Central Hypoventilation syndrome (When brain receptors fail to detect CO2 level changes during sleep, causing low breathing and O2 level.
Symptoms:
Snoring, Catathrenia [20].
RLS also called to as Willis-Ekbom Disease is typically a chronic condition characterized by an intense desire to move the legs. Furthermore, numerous individuals experience limb jerking while a sleep, a condition referred to as Periodic Limb Movement.
Etiology:
Due to Iron deficiency (Anaemia), End Stage Renal Disease (ESRD), Multiple sclerosis, Diabetes, Sleep apnoea
Symptoms:
Uncomfortable sensation in the legs (sitting or lying down) [21].
Parasomnias
Parasomnias are sleep disorders involving abnormal movements, behaviours or emotions during sleep [22].
Types Of Parasomnias:
They are two types of parasomnias (NREM and REM)
NREM Parasomnias
It is also referred to as somnambulism or noctambulism. It usually happens during the initial phase of the night when slow-wave sleep is most dominant [23].
Also known as Sleep terror, is a sleep disorder that causes panic or anxiety and usually occurs during the initial phases of sleep [24].
Rem Parasomnias
The main characteristic of RBD is the loss of muscle atonia or hypotonia and the occurrence of different unusual movements during sleep [25].
Nightmares are intense and frightening dreams that happen during REM sleep, followed by waking up with vivid memory recall [26].
Diagnosis
The top two vital laboratory tests comprise polysomnography (PSG) and multiple sleep latency test (MSLT).
Polysomnography
Polysomnography (PSG), a form of sleep study, is a comprehensive analysis of sleep and a diagnostic tool in sleep medicine. It monitors various bodily functions such as brain activity (EEG), eye movements (EOG0, muscle activity (EMG), and heart rhythm (ECG) [27].
Multiple sleep latency tests
The MSLT assess sleep disorder by measuring the time from nap start to sleep onset, useful for diagnosing hypersomnolence disorders like narcolepsy. It involves monitoring brain waves, muscle activity, and eye movements, typically spanning 7 hours in a day [28].
Treatment For Sleep Disorders
Treatment for sleep disorders are depend upon the particular type of sleep disorder.
Treatment for Insomnia can be divided into non-pharmacological and pharmacological treatments.
Non-pharmacological Treatment
Pharmacological Treatment
Treatment for obstructive sleep apnoea (OSA) primarily involves using positive airway therapy (PAP) devices, making lifestyle changes, and in some cases, utilizing oral appliances or surgical interventions [33]. For patients who continue to experience excessive daytime sleepiness despite proper PAP usage and resolution of breathing problems, drug treatments like solriamfetol, stimulants (such as amphetamines or modafinil), and norepinephrine reuptake inhibitors may be considered to improve wakefulness [34]. Modafinil, a non- amphetamine stimulant that enhances wakefulness, is the primary treatment choice for narcolepsy due to its ability to decrease daytime sleepiness, good tolerability, and lower potential for abuse compared to traditional stimulants like amphetamines and methylphenidate, which are used as secondary treatment. Patients experiencing significant cataplexy may find relief from medications that suppress REM, such as antidepressants and sodium oxybate. Light-phase shift therapy can help correct sleep disturbances related to circadian rhythm abnormalities by exposing patients to bright light. Gabapentin enacarbil, a prodrug of gabapentin, is effective in improving restless leg syndrome and can therefore help alleviate sleep disturbances [35].
CONCLUSION
It has a major impact on controlling both body and central nervous system processes. Daily lifestyle decisions have a big impact on how sleep is regulated. Since it promotes healing, growth, and restoration, getting enough sleep is crucial for maintaining general physical and mental health.
REFERENCES



Dr. Manchineni Prasada Rao*, Dr. V Rajini, Dr. Y Narasimha Rao, L. Komalatha, A Review Article on Sleep Disorders, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 448-456. https://doi.org/10.5281/zenodo.15795520
 10.5281/zenodo.15795520
10.5281/zenodo.15795520
