Smt. Kishoritai Bhoyar College of Pharmacy, Kamptee (Nagpur
Polycystic ovary syndrome (PCOS) is a prevalent hormonal disorder affecting women during their reproductive years. It is characterized by hormonal imbalances, insulin resistance, and the presence of multiple cysts on the ovaries. PCOS is associated with various symptoms and complications, such as irregular menstrual cycles, infertility, obesity, and metabolic disorders. Oxytocin, a hormone primarily known for its involvement in childbirth and lactation, has emerged as a potential treatment for PCOS due to its diverse physiological effects. Recent studies have highlighted the significant role of oxytocin in regulating reproductive and metabolic processes, which are disrupted in PCOS. Oxytocin acts on the hypothalamus-pituitary-gonadal axis, influencing the release of gonadotropin-releasing hormone (GnRH), luteinizing hormone (LH), and follicle-stimulating hormone (FSH). By modulating these hormonal pathways, oxytocin may help restore a normal menstrual cycle and promote ovulation in women with PCOS. Moreover, oxytocin exhibits insulin-sensitizing properties, enhancing glucose uptake in adipose tissue and skeletal muscles. This effect has the potential to improve insulin resistance, a key characteristic of PCOS, and reduce the risk of developing type 2 diabetes and metabolic syndrome. Oxytocin may also aid in weight management by reducing food intake and increasing feelings of satiety, thereby addressing the obesity commonly associated with PCOS. Beyond its endocrine and metabolic effects, oxytocin has been shown to have positive psychological and social impacts. It promotes social bonding, reduces anxiety, and improves mood, which could be particularly beneficial for PCOS patients experiencing emotional distress or social challenges related to the syndrome. While initial studies have demonstrated promising results, further research is necessary to determine the optimal dosage, duration, and safety profile of oxytocin treatment for PCOS. Additionally, long-term effects and impacts on fertility outcomes need careful evaluation. Nevertheless, oxytocin represents an intriguing and innovative therapeutic approach for managing PCOS, as it has the potential to address multiple aspects of the syndrome, including its reproductive, metabolic, and psychological components
PCOS is a complex condition in which we will see the features like hyperandrogenism, persistent anovulation and it is accompanied by a number of hormonal abnormalities, including an elevated LH-to-FSH ratio. (Conway et.al.,2014) PCOS affects women who are on fertile stage is becoming an epidemic. Ovarian antral follicle cysts are a symptom of this condition, which is brought on by an imbalance in female sex hormones. A cyst is an egg-containing water-filled sac that should have been expelled regularly for potential fertilisation. (Ndefo et.al.,2013) Functional cysts, which are created when an egg is transformed into a cyst, which will stop ovulation. The disruption of menstrual cycle known as a “amenorrhea”, occurs as a result of obstructed ovulation. The size of the ovary rises, reaching a maximum width of 10 cm, due to the water-retained cysts, some of which can be as large as 10 mm broad. (Jiang et.al.,2021) Pregnancy becomes challenging since ovulation and the menstrual cycle impede fertilisation and conception. If implantation takes place there will be higher risk of birth and termination. (Witchel et.al.,2019) Newborns are very young for their gestational age and eclampsia arise PCOS can lead to a number of pregnancy-related issues, including gestational diabetes and pregnancy-induced hypertension. Ovarian theca cells support the developing follicle, aiding in the production of mature oocytes. (McDonnell et.al.,2017) However, these cells are hypersensitive to insulin's stimulatory effects in PCOS patients, which causes them to multiply and lead to ovarian hyperthecosis. Insulin resistance increases the theca cells' androgenic potential, exacerbating PCOS. (Rosenfield et.al.,2016) Additionally, androgenism in PCOS is aided by theca cells' increased sensitivity to gonadal steroid gonadotropin activation. (Patel et.al.,2018) PCOS has also been related to endometrial and breast cancers, as well as neurological and psychological adverse effects (such as anxiety and despair). (Diamanti-Kandarakis et.al.,1998). The three main phenotypic features of this illness are ovulatory failure, polycystic ovaries, and hyperandrogenism. This syndrome is associated with obesity, hyperinsulinemia, (T2DM), and insulin resistance (present in 60–80% of PCOS-affected women). (Barthelmess et.al, 2014). Numerous studies have found that women with PCOS had a considerably greater IGF-1/IGFBP-1 ratio. IGF-1 availability in thecal cells may rise, leading to an increase in androgen production. (Leo et.al, 2016)
Prevalence Study of PCOS Across Globe
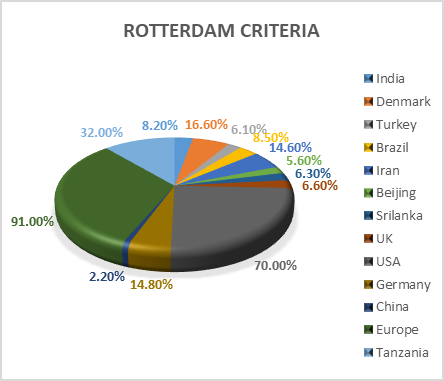
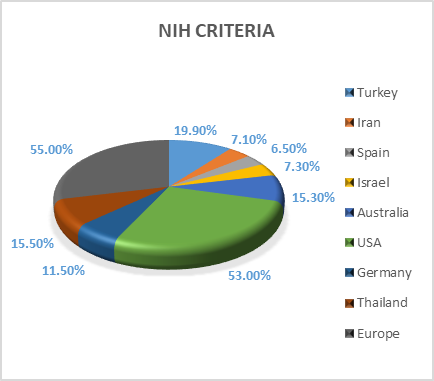
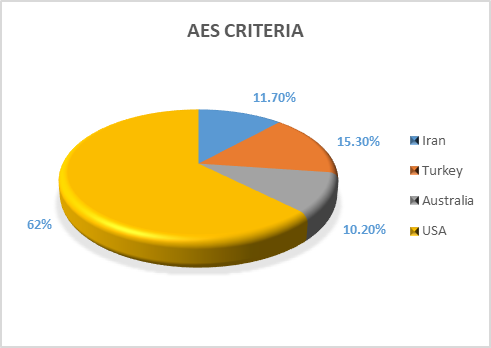
Fig 1: Prevalence of PCOS according to AES-Androgen Excess Society, NIH-National Institutes of Health, RC-Rotterdam Criteria
Causes of PCOS
The exact cause of PCOS is still unknown but parameters like insulin resistance, Low – grade Inflammation, Heredity and Excess secretion of Androgen lead to develop PCOS in women. The excessive amount of insulin produced by body leads to more production of androgen into the body. You may experience difficulty with ovulation, the process by which eggs are released from the ovary. Dark, velvety patches of skin in the armpits, groyne, or under the breasts are one indication of insulin resistance. Other symptoms could include a greater appetite and weight gain. In reaction to an infection or damage, white blood cells produce different chemicals. Low-grade inflammation is the term for this reaction. According to research, polycystic ovaries in persons with PCOS create androgens as a result of a sort of chronic, low-grade inflammation. This may result in issues with the heart and blood vessels. Heredity may be connected to PCOS. A family history of PCOS may increase your risk of having the disease. In PCOS condition ovaries may create lot of androgens. Ovulation is hampered by an excess of androgen. This indicates that the follicles in which the eggs develop are not regularly used to release the eggs. Acne and hirsutism are further side effects of too much androgen (Divyashree et.al.,2019).
SIGNS AND SYMPTOMS OF PCOS
Basically, pcos is characterised by three main features.
Oligomenorrhea: - A high frequency of miscarriages and infertility are linked to oligomenorrhea/amenorrhea. Around 12 menstrual cycles per year are typical for reproductively healthy women. However, PCOS women exhibit irregularities in their menstrual periods with a very low number of cycles (less than 10) per year, which is referred to as oligomenorrhea. Amenorrhea is the absence of cyclicity in the absence of pregnancy or lactation.
Hyperandrogenism: - In comparison to the male system, the female system secretes androgen in relatively smaller amounts—60% from ovarian theca cells and 40% from the adrenal zona reticularis. Compared to healthy women, PCOS women have higher levels of androgen. There could be a number of causes for this. Acne, hirsutism, and other signs of clinical hyperandrogenism are visible.
Presence of cystic follicles: - Ultrasonography allowed for the visualisation of cystic follicles. Moreover, the cysts' number, diameter, and size were determined.
Insulin resistance and compensatory hyperinsulinemia and Glucose intolerance are the other minor features found in pcos women. (Divyashree et.al.,2019)
Current Therapy on PCOS
For Obesity
There is some indication that hyperandrogenism associated with PCOS results in central adiposity. Obesity is known to increase the risk of anovulation, miscarriage, and problems in late pregnancy (such as pre-eclampsia and gestational diabetes). Obesity is seen in 35%–60% of women with PCOS and is associated with a lack of response or a delay in response to several treatments, including CC, gonadotropins, and surgical treatment of diathermy via laparoscopy. Weight loss increases the possibility of ovulation and pregnancy and enhances the endocrine profile. (Atawia et.al.,2019)
Diet & Exercise
5%–10% weight loss required to restore ovarian function in obese PCOS patients can be achieved with any variation of the low-calorie, low-carbohydrate diets that are advised. Patients with PCOS are also advised to increase their physical activity, albeit this frequently has drawbacks. A longer weight loss maintenance time did seem to be associated in these patients, but no significant differences were discovered when various diets, whether or not connected with activity, were examined. (Gill et.al.,2019)
Bariatric Surgery
The use of bariatric surgery as a weight loss method for severely obese people has been recommended. bariatric surgery improves ovulation, insulin resistance, hyperandrogenism, and hirsutism. (Escobar-Morreale et.al.,2005)
Ovulation induction
Low FSH levels and the cessation of antral follicle growth during the maturational stage are related to anovulation in PCOS. Anovulatory infertility is the primary concern for many women. The next sections go over several medications and other ovulation induction options. (Messinis et.al.,2005)
Clomiphene Citrate
The estrogen-signalling pathway's negative feedback is blocked by the oestrogen receptor antagonist CC, which raises the amount of FSH available. A surge in LH and ovulation follow an increase in FSH, which causes follicular expansion. Patients with PCOS and anovulation who have normal FSH levels should consider CC, but there are some restrictions. (Homburg et.al., 2005)
Metformin
Metformin use is linked to better ovulation, lower levels of circulating testosterone, and greater menstrual cyclicity. Metabolic advantages are increased when weight loss occurs, and metformin use alone may increase weight loss. (Kim et.al.,2020)Although it also reduces intestinal glucose absorption and boosts insulin sensitivity in peripheral tissues, its main therapeutic effect is to block hepatic glucose synthesis. Metformin probably affects ovarian androgen production, theca cell proliferation, and endometrial growth through a number of mechanisms, including lowering insulin levels and changing how insulin affects these processes. It also inhibits ovarian gluconeogenesis, possibly through a direct impact, which lowers the generation of ovarian androgen. (Sharpe et.al.,2019)But regardless of whether metformin is used alone, in conjunction with clomiphene, or in comparison to clomiphene, there is no proof that it increases live birth rates. But metformin seems to have a limited role in helping PCOS-affected women have better reproductive results. (Legro et.al.,2007)
Insilico Evaluation
According to a study done on silica, anethole, which is present in essential oils, may also be a possible PCOS therapy drug because it was predicted that it would bind androgen receptors more strongly than FSH receptors and IRS 1 receptors. (Chandran et.al.,2019)
Gonadotropin
Exogenous gonadotropins are the second potential treatment option when CC resistance in women with PCOS has been established. The purpose of gonadotropins is to promote ovulation, maintain and stimulate optimal follicle growth by the carefully regulated dose of FSH, and produce a follicle that can be fertilised.The primary problem with gonadotropins is that they increase the growth of numerous follicles, which raises the possibility of (OHSS) and multiple pregnancies.
Laparoscopic ovarian diathermy
Bilateral laparoscopic ovarian surgery with monopolar electrocautery (multiple controlled perforation of the ovary) or laser is a suitable alternative for clomiphene-resistant PCOS patients who are unable to adhere to the close monitoring required for gonadotropin administration. Both techniques produce comparable outcomes. Compared to gonadotropins, LOD is associated with a decreased multiple gestation rate. (Palomba et.al.,2007)LOD helps 63%–85% of women resume regular menstruation, and the positive effects on reproductive results appear to endure for few years in a lot of females. Using metformin as medicine is equally effective in reversing clinical, endocrine, along with PCOS-related metabolic problems. The clinical, endocrine, and metabolic problems linked to PCOS can all be resolved with metformin therapy. (Palomba et.al.,2005)
In vitro fertilization techniques
When there are co-occurring illnesses, such as severe endometriosis, tubal blockage in women, and male factors such azoospermia that make other methods less viable, IVF is the primary option. The risk of multiple gestations was dramatically decreased by IVF with a single embryo transfer. Only one embryo may be implanted with IVF, or all embryos may be cryopreserved using IVF and only one embryo transferred at a subsequent cycle with endometrial stimulation rather than ovarian stimulation. IVF techniques have a success rate comparable to that of people without PCOS, indicating that PCOS does not affect embryo implantation. (Xiong et.al.,2019)
Treatment of menstrual dysfunction
Endometrial hyperplasia and cancer risk are both elevated by chronic anovulation. Therefore, it is advisable to take endometrial biopsy into account in PCOS patients who haven't seen menstrual blood in a year or more. In order to assess whether or not to do an endometrial biopsy, several researchers have suggested using ultrasonography to measure endometrial thickness. By giving cyclic progestin or oral contraceptives that contain both estrogen and progestin, endometrial growth can be prevented. The latter strategy, which also lessens ovarian androgen production, would be very helpful in this situation. (Balen et.al.,2001 and Nader et.al.,2008)
Hirsutism
Generally speaking, hirsutism is seen in 70%–80% of women with high androgen. Androgens speed up hair development and change vellus hair into terminal hair. Reducing androgens decreases the growth of existing terminal hair and inhibits the growth of newly formed hair. Cycles of hair growth are irregular. For facial hair, the anagen phase, which varies according on the location of the body, lasts about four months. The benefits of hormone therapy take longer than six months to reach their peak because of the lengthy hair growth cycle. (Korytkowski et.al.,1995)
Those females who don't want to conceive OCPs are used as a treatment. Here by encouraging direct negative feedback on LH secretion, it leads in less androgen production in the ovaries, OCPs lessen hyperandrogenism and additionally it raises SHBG produced by the liver, which reduces the amount of free androgen that is circulated. One of the newest OCPs is a combination of drospirenone, ethinyl estradiol, and nonandrogenic progestin that may be more effective at reducing the formation of new terminal hair and acne. It makes potentially the greatest option for treating PCOS in women. (Badawy et.al.,2011)
Antiandrogens
Spironolactone, CPA, and flutamide are examples of antiandrogens that work by inhibiting androgen-binding receptors competitively or by reducing androgen synthesis.
Glucocorticoids
Patients with adrenal hyperandrogenism have utilised glucocorticoids to reduce adrenal androgen production. It helps in avoiding and treating hirsutism as well as allowing ovulatory cycles in people with congenital adrenal hyperplasia. (Azziz et.al.,1998 and Spritzer et.al.,1990)
Gonadotropin-releasing hormone agonist
GnRHa responds in women with severe insulin resistance. Pituitary hormones are suppressed by GnRHa, and androgen and estradiol release are reduced, which helps with severe hirsutism. (Novaira et.al.,2014)
Insulin-lowering agents
Both metformin and thiazolidinediones have the potential to reduce ovarian androgen production, mostly due to their effects on insulin. (Yilmaz et.al.,2005)
Topical treatment also beneficial like eflornithine hydrochloride has been authorized for topical use in treating facial hirsutism because it inhibits the human skin enzyme ornithine decarboxylase. It also combines with laser treatment. Direct hair removal Electrolysis has been also used for many years to remove unwanted hair. (Malhotra et.al.,2001)
Genetic basis of PCOS
The syndromic disorder PCOS is polygenic and multifactorial. A multitude of anomalies contribute to PCOS, a complex condition. PCOS is linked to all genes and mutations that directly or indirectly impact the ovaries. Elevated androgen levels are most frequently linked to PCOS as an endocrine condition. CYP11a gene an enzyme that is necessary for a transitional stage in the conversion of cholesterol to progesterone is encoded by the CYP11a gene. This phase of the conversion of cholesterol is rate-limiting. (Diamanti-Kandarakis et.al.,2000) CYP21 gene an enzyme that is encoded by CYP21 catalyses the conversion of 17-hydroxyprogesterone to 11-deoxycortisol during the manufacture of steroid hormones. Due to variance, a less-active enzyme results in inefficient anabolism of steroidogenesis, which further contributes to PCOS. (Witchel et.al., 2005) CYP17 gene a P450c17 enzyme (encoded by CYP17) is responsible for converting pregnenolone and progesterone into 17-hydroxypregnenolone and 17-hydroxyprogesterone, respectively. In PCOS patient level of androgen was high observed by Rosenfield et.al. In theca cell CYP17 expression was up it was observed by Wickenheisser et.al and in the promoter area polymorph that is connected to PCOS observed by Carey et al. (Chua et.al.,2012) CYP19 gene The CYP19 gene, which produces the aromatase p450 enzyme required for the synthesis of oestrogen, is located on chromosome 15q21, aromatase activity has been observed in both obese and lean women with PCOS.
Genes Involved in Steroid Hormone Effects
Androgen Receptor Gene
The AR gene, which has 11 exons and codes for a tridomain protein with a length of 90 kb, is located on chromosome X's "q" arm. (Gottlieb et.al.,2012) According to reports, PCOS is caused by gene mutations and structural disturbance. When the "X" chromosome is inactivated, the biological mechanism is disrupted, which results in an increase in androgen hormone and PCOS. (Urbanek 2007).
Sex Hormone-Binding Globulin Gene
On chromosome 17p13–p12, the SHBG gene is located. A protein with 373 amino acids is created by SHBG. By binding to androgens, primarily with oestrogen and testosterone, the protein product of SHBG regulates the amount of sex hormones in the body. Hepatocytes in the liver produce a large portion of SHBG. Multiple metabolic variables, including androgens and insulin, regulate the synthesis of SHBG by hepatocytes. Females with PCOS have reduced SHBG concentrations, which has primarily been linked to a negative impact of hyperinsulinemia on SHBG production. Numerous studies have shown that the SHBG gene's single nucleotide polymorphism is strongly related to PCOS. (Deswal et.al.,2018)
Genes Involved in Gonadotropin Action and Regulation
Lutein Hormone (LH) and Its Receptor Gene
PCOS is commonly attributed to both elevated LH levels and altered LH function. PCOS is brought on by these anomalies, which lead to annulations. A high LH level subsequently increases androgen production. Reduced follicle-stimulating hormone (FSH) is the adverse feedback in response to increased LH, which may indirectly contribute to the exacerbation of excess androgen in the ovaries by impairing androgen's ability to convert to oestrogen. Initially, PCOS patients were found to have a point mutation (Trp8Arg and Ilg15Thr) in a gene encoding the B subunit. According to reports PCOS has also been linked to polymorphism in the LH subunit gene. (Khan et.al.,2019)
AMH gene is 13.3 on the long arm of chromosome 19. The gene's five exons89 code for a protein that plays a role in infertility. PCOS is linked to variations in the AMH gene. GWAS and whole exome sequencing revealed several variations in the AMH gene as reliable indicators of PCOS. (Gorsic et.al.,2017 and Cimino et.al.,2016)
Follicular Stimulating Hormone Receptor (FSHR)
The 14 exon FSHR gene is found on the "p" arm of chromosome 2 and is situated there. The G-coupled protein receptor that the gene encodes is necessary for gonad development. The structural protein is disrupted by gene mutation, which leading to the hormone being out of balance that is why the unbalanced hormones causes PCOS. (Baban ASS et.al.,2018 and Laven et.al.,2019)
Genes Involved in Insulin Action and Secretion
The Insulin Gene
Theca cell receptors on insulin play a vital role in the synthesis of androgen. Phosphoinositide 3-kinase/protein kinase B is a pathway that is activated in PCOS theca cells and is responsible for inducing this insulin action. Similar to LH, high insulin levels promote androgen production even more.Tyrosine hydroxylase and IGF-II are linked together at 11p15.5 by the INS gene. A tandem repeat of VNTR takes up the entire 5′ untranslated region. VNTR polymorphism controls the rate of transcription of INS and IGF-II. This VNTR polymorphism is linked to PCOS. (Cabrera-Cruz et.al.,2020)
INSR gene
This gene produces a protein called turmeric that has two alpha and two chains. The strongest link with PCOS was found to be D19S884 when a greater portion of chromosome 19p13.2 was investigated the INSR gene is also located in this area of the chromosome.
Insulin Receptor Substrate Proteins
Insulin and its receptor form a bond. The binding of insulin causes the receptor to become auto phosphorylated, which activates it. The INS receptor's tyrosine kinase activity then phosphorylates IRS-1 and IRS- 2. The subsequent downstream phase makes further use of these activated substrates. To determine whether the genes IRS-1 and IRS-2 are associated with PCOS, several researches have been conducted. (Genazzani et.al.,2014)
CAPN10 gene
CAPN10 is present on the long arm of “q” of chromosome 2 and consists of 12 exons. This gene makes heterodimeric protein calcium dependent cysteine protease heterodimeric protein. The gene is linked to type 1.108 diabetes mellitus. Calpain 10 is a protein that obstructs the metabolism and release of insulin. PCOS is brought on by a low level of insulin; as a result, PCOS can also result from a calpain 10 mutation. Thus, CAPN10 is a potential gene responsible for PCOS. (Ajmal et.al.,2019)
Drawback of current therapy
The value of exercise in the management of obese PCOS patients has been investigated in a number of researches. When different diets, whether or not they included exercise, were compared, no one observed any substantial differences, albeit these patients' prolonged weight loss maintenance times did seem to be related.Medications and other options available for the induction of ovulation. Few side effects and minimal monitoring are associated with clomiphene citrate. Insulin resistance, glucose tolerance, vascular reactivity, and coagulability may all be negatively impacted by oral contraceptives. When used in significant quantities, spirolactone exhibits mild antiandrogenic properties (100–200 mg daily). In addition to those caused by OCPs, it has visible effects on hirsutism and obesity. Despite being typically well accepted, it can occasionally produce lethargy, postural hypotension, and dizziness. When used alone and in large doses, it can also result in menstrual irregularities.For anovulatory women with PCOS, gonadotropin should be viewed as a secondary reproductive treatment. Ultrasound and lab monitoring are required during the treatment. The disadvantages of the therapy include high costs, the possibility of multiple pregnancies, and the risk of ovarian hyperstimulation syndrome. (Vause et.al., 2010)
INTRODUCTION OF OXYTOCIN: -
In 1909, Sir Henry H. Dale observed that an extract from the human posterior pituitary gland convulsed a pregnant cat's uterus (Louisa Dalton) OXY (Syntocinon® - Orphan Biovitrum) was first synthesised in 1954 (Boie, Sidsel (1996). The peptide hormone and neuropeptide OXY is typically made in the hypothalamus and released by the posterior pituitary (Gray's Anatomy:) A neurohypophysial hormone recognised to play crucial roles in labour, nursing, and sexual behaviour is OXY. As a neurohormone, neurotransmitter, or neuromodulator, the neuropeptide OXY has a wide range of effects on the brain's central and periphery. The hypothalamic PVN and SON nuclei of the CNS include magnocellular neurons that primarily express the OXY gene. (Kiss and Mikkelsen 2005)Important neuropsychiatric activities of OXY include modulation of neuroendocrine reflexes and socially complicated behaviours. Other cell lines like the corpus luteum, placenta, and leydig cells of the testis contain OXY, supporting its reproductive function. (Fischer-Shofty et.al.,2010)Recently, OXY has been considered as a viable treatment for psychiatric diseases like autism and borderline personality disorders since it suppresses hunger and lessens fear, anxiety, and despair (Ho and Blevins 2013). By feeding mice an HFD, Zhang and colleagues demonstrated that the mice's hypothalamic OXY receptors were upregulated, and that OXY treatment prevented the mice's HFD induced obesity (Zhang et.al., 2011). Furthermore, the OXY nasal spray not only reduced body weight but also enhanced lipid profiles, glucose metabolism, and insulin levels. (Zhang et.al.,2013) According to research findings released in 2002, functional OXY receptors are expressed by human granulosa-cell lines, and OXY stimulates the synthesis of progesterone (Copland et.al.,2002) OXY beneficial effects on rat folliculogenesis and ovulation have been studied. (Roushangar et.al.,2009) Another investigation revealed that adding OXY to the drugs used to induce ovulation in anovulatory women enhanced the clinical pregnancy rates. (Sayyah-Melli et.al 2012)
Role of Oxytocin in PCOS
OXY plays a diagnostic role in PCOS and also serves as a predictive indicator of ovarian response and therapy success rates. Further research on the impact of various OXY doses on PCOS women's ability to expedite ovulation induction, lose weight, and balance their hormonal profile is advised in order to better PCOS management. (Jahromi et.al.,2018) Also in a DHT-induced rat model of PCOS, peripheral injection of OXY led to decreases in body weight and food consumption. Moreover, OXY treatment led to decreases in adipocyte size and visceral fat weight. According to this study we found that the OXY can use for the management of pcos. (Iwasa et.al.,2020)
Impact of PCOS on Oxytocin level
As per Shota Yamamoto 2022, they investigate that the rats with PCOS had considerably lower serum OXY levels than the rats in the Control group, suggesting that human PCOS patients may also have lower endogenous OXY levels. (Yamamoto et.al.,2022) The endogenous OXY level was found to be lower in fatty rats in earlier research, and it is believed that the same pathogenic mechanisms are play in obese PCOS patients. (Zhang et.al.,2011, Gajdosechova et.al.,2014 and Yuan et.al.2016)
Preclinical studies of Oxytocin in PCOS
A 9-amino acid neuropeptide called OXY has recently come to light as a factor in the regulation of metabolism, appetite, and body weight in both humans and animals. OXY can be administered intraperitoneally (i.p.), subcutaneously, intracerebroventricularly, or intravenously. In some species, including mice, rats, and people, these injections reduce food intake and body weight. Additionally, OXY injections in these species both directly and indirectly encourage the lipolysis of adipose tissue by beta oxidation and decrease fat mass. It's interesting to note that diet-induced and genetically obese animals show more pronounced OXY effects on food intake and fat mass. (Iwasa et.al.,2020) By changing the levels of other appetite-regulating hormones (for example, by raising the anorexigenic hormones CCK and GLP1, OXY may indirectly affect appetite GLP1. (Lawson et.al.,2017)
Clinical study of Oxytocin
In some research paper we studied that OXY peripheral delivery resulted in weight loss. OXY administration also resulted in decreases in adipocyte size and visceral fat weight. (Takeshi Iwasa et.al.,2019) In adipocytes, OXY boosted lipolysis and the expression of genes involved in lipid metabolism. As a result, OXY anorectic and lipolytic effects may have contributed to the decreases in body fat seen in the current study.Longer-term dosing may lead to ovarian morphological changes and ovulation restoration. Therefore, more research is required to determine how OXY affects reproductive processes in obese people. It has been noted that prolonged OXY nasal administration in obese and overweight people lowers blood levels of low-density lipoprotein and has little to no effect on hepatic enzyme levels. These findings suggest that OXY therapy does not result in hepatic issues in obese people, but rather enhances hepatic functions. Because of this, OXY may be safe to use in a clinical context since it does not appear to have any clear side effects.
Future Prospective
The pathophysiology of PCOS as a complex disease and the difficulties experienced in treating the disease. It is currently recommended that a team consisting of an endocrinologist, a doctor, a gynecologist, and a reproductive medicine specialist would aid these patients in light of the pathophysiology of PCOS. Depending on the appearance, comorbidities, age and stage of life, family history, patient preferences, and medical objectives, suppressive or maintenance treatment for PCOS typically entails lifelong follow-up and polytherapy involving a number of therapeutic modalities.
REFERENCES:



Khushi M. Kongre*, Saloni H. Nagpure, Milind J. Umekar, A Review of the Role of Oxytocin in Polycystic Ovary Syndrome, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 3342-3358. https://doi.org/10.5281/zenodo.18409262
 Khushi M. Kongre*, Saloni H. Nagpure, Milind J. Umekar, A Review of the Role of Oxytocin in Polycystic Ovary Syndrome, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 3342-3358. https://doi.org/10.5281/zenodo.18409262
Khushi M. Kongre*, Saloni H. Nagpure, Milind J. Umekar, A Review of the Role of Oxytocin in Polycystic Ovary Syndrome, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 3342-3358. https://doi.org/10.5281/zenodo.18409262
