Department of Pharmaceutics, K.K. Wagh College of Pharmacy, Nashik, Maharashtra, India.
The appearance of intragastric pH less than 4 for a minimum of 60 consecutive minutes Throughout the night in patients receiving proton-pump inhibitors (PPIs) is known as nocturnal acid breakthrough. More than 70% of Helicobacter pylori-negative patients on PPI therapy experience nocturnal acid breakthrough, which can have clinical implications, particularly in those with Barrett's esophagus, complex GERD, and abnormalities in esophageal motility.An important development in the treatment of nocturnal acid secretion is the availability of sustained-release cimetidine tablets. Cimetidine's pharmacokinetic profile is improved by this formulation, enabling longer-lasting therapeutic benefits and better symptom management at night. Sustained-release cimetidine efficiently lowers nocturnal acid production by sustaining steady medication levels over time, reducing sleep-disturbing symptoms including heartburn and acid reflux. Because there are fewer dosage requirements, this improvement not only encourages improved patient compliance but also lowers the risk of chronic acid exposure-related problems such as Barrett's esophagus and esophagitis. To improve patients' quality of life and overall health outcomes, sustained-release cimetidine could be marketed as a first-line treatment for nocturnal acid-related disorders.
"Peghini and colleagues coined the term 'nocturnal acid breakthrough' (NAB), which refers to the occurrence of stomach acid reaching a pH level below 4 for at least 60 consecutive minutes during the overnight period (from 10:00 PM to 6:00 AM)." More than 70% of Helicobacter pylori-negative patients receiving proton pump inhibitors (PPIs) experience nocturnal acid breakthrough (NAB), which can have clinical repercussions, especially for those with Barrett's esophagus, complex gastro-oesophageal reflux disease (GERD), and anomalies in oesophageal motility. 70% of GERD patients on PPI twice a day had NAB, which is linked to in 30 ± 50% of patients, gastro-oesophageal reflux is present. One of the primary causes of GERD treatment failure that jeopardizes patient therapeutic objectives is NAB. Heartburn, coughing, and choking due to fluid in the throat are the most common symptoms of nocturnal acid breakthrough (NAB); morning phlegm, wheezing, and dyspnoea are all commonly described at this period.Cimetidine is an antagonist of the histamine H? receptor. It is a competitive antagonist of the parietal cell's histamine H? receptor. It is commonly used in conditions including acid reflux-related heartburn, duodenal and gastric ulcers, gastro-oesophageal reflux illnesses, and hypersecretory syndromes like Zollinger-Elosions, where it may be helpful to reduce gastric acid secretion. According to published research, cimetidine has a short elimination half-life and is poorly absorbed in the lower gastrointestinal tract.
|
Extended acid contact period during sleep. |
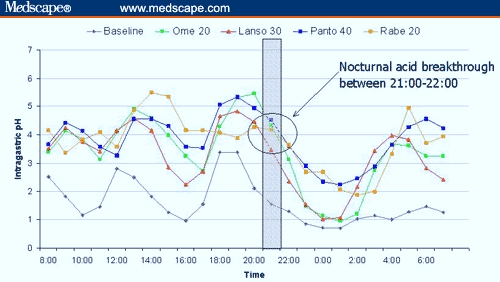
Figure 2. Twenty-four-hour intragastric pH profiles of daily-dosed PPIs show the onset of nocturnal acid breakthrough between 9:00 and 10:00 PM for all PPIs. [7]
Cimetidine, a gastric acid reducer, can temporarily treat duodenal and stomach ulcers [8]. It is also prescribed to treat reflux esophagitis, prevent stress-induced stomach ulcers, and control gastric hypersecretion. Along with other H2-receptor antagonists, cimetidine is now available over-the-counter to avoid heartburn and acid indigestion in response to the widespread use of proton pump inhibitors (PPIs) like omeprazole, which are also approved for the same purposes.Before the approval of proton pump inhibitors, intravenous cimetidine, an H2-receptor antagonist, was used as a therapeutic option for critically ill patients in the intensive care unit requiring prophylaxis against stress-induced ulcers.
NOCTURNAL ACID SECRETION:
In 1987, Kruse-Anderson et al. [10] assessed acidic gastroesophageal reflux in asymptomatic volunteers and patients with duodenal ulcers, both with and without GERD, using pH monitoring. The study found that GERD patients experienced significant acid reflux during the 6-hour evening, even though it was most noticeable during the three postprandial hours. Compared to 37.9% of GERD patients, 5.5% of reflux in healthy people happened throughout the night. The motility of the esophagus was reduced. A few years later, Sozzi et al. [11] investigated nocturnal reflux patterns in healthy volunteers as well as in patients with and without erosive esophagitis. The nighttime stomach pH of esophagitis patients was considerably lower (1.6 vs. 2.2 and 2.6, respectively), and they were exposed to more esophageal acid between 11:00 PM and 3:00 AM during the nocturnal period, at pH < 2. These findings unequivocally showed that the pathophysiology of gastroesophageal reflux is mostly influenced by gastric acidity.In recent years, it has become evident that the spectrum of GERD has broadened. The majority of individuals with GERD symptoms do not have erosive reflux disease (ERD); these individuals are classified as having non-erosive reflux disease (NERD), or negative-endoscopy reflux disease. NERD and ERD may differ significantly in terms of pathogenesis and treatment. As a result, patients with NERD may not be suitable candidates for surgery, as they appear to be somewhat resistant to proton pump inhibitors (PPIs). Future research on the role of genetics in the various symptoms of GERD will build upon the findings of recent twin studies, which have shown that genetic factors contribute to the disease. [12]
Control of Nocturnal Acid Breakthrough (NAB) with Bedtime H2-Receptor Antagonist Therapy:
When proton pump inhibitors (PPIs) are administered 15–30 minutes before meals, the drug's blood concentrations peak during meal-induced proton pump activity, effectively blocking numerous pumps and maximizing therapeutic efficacy. [13] Since there is typically no food consumption at night, administering an additional drug, such as H2-receptor antagonists (H2RAs), at bedtime may be a viable strategy for further suppressing nocturnal acid output.Peghini and colleagues first studied the addition of H2-receptor antagonists (H2RAs) to PPI therapy to prevent nocturnal acid breakthroughs. [14] This double-blind study randomly assigned 12 healthy volunteers, who were taking omeprazole 20 mg before breakfast and supper, to receive either a placebo, ranitidine 150 mg, ranitidine 300 mg, or an additional dose of omeprazole 20 mg at bedtime. The third bedtime dose of omeprazole was statistically less effective at controlling nocturnal acid breakthrough than both doses of ranitidine. However, the addition of omeprazole at bedtime was still significantly superior to the placebo in reducing nocturnal acid breakthrough. Only one-third of participants experienced nocturnal acid breakthroughs on the first day after adding ranitidine to the regimen.A second dose of PPI before dinner is still required, even with the addition of a nighttime H2RA. Khoury and colleagues conducted a randomized, crossover study comparing nocturnal acid control in 20 healthy subjects who received a 7-day course of either omeprazole 20 mg twice daily (before meals) or omeprazole 20 mg before breakfast and ranitidine 150 mg before bedtime [15]. The study supports the idea that H2-receptor antagonists (H2RAs) should be used in addition to, rather than as a replacement for, twice-daily PPI therapy. This is evidenced by the finding that overnight intragastric pH control was better when subjects received omeprazole 20 mg twice daily compared to omeprazole 20 mg before breakfast and ranitidine 150 mg before bedtime.
CLINICAL IMPORTANCE OF NOCTURNAL ACID BREAKTHROUGH
At night, most people lie down and swallow less frequently than during the day. Esophageal acid clearance primarily relies on peristalsis in the absence of gravity and reduced salivary buffering. Thus, the nighttime acid breakthrough is especially crucial for individuals with Barrett's esophagus, complex GERD, and abnormalities of esophageal motility. Clinical research supports the significance of the aforementioned pathways. At least 50% of individuals with GERD who also had Barrett's esophagus and scleroderma experienced higher nocturnal esophageal acid exposure during acid breakthrough, according to research by Fouad and colleagues [16]. Katz and associates conducted a related study [17] and found that patients with nocturnal acid breakthrough had an 8-fold increased risk of reflux during gastric acid breakthrough compared to those without nocturnal acid breakthrough. This group also exhibited a high frequency of distal esophageal body ontractions (<30 mmHg) and decreased lower esophageal sphincter pressure.In healthy volunteers and patients with mild GERD, the clinical significance of nocturnal acid breakthrough remains more debatable.Concerns about the clinical significance of nocturnal acid breakthrough are raised by these seemingly contentious studies. For patients with uncomplicated GERD and normal esophageal clearance mechanisms, the phenomenon is likely to be of minimal significance. However, a nocturnal acid breakthrough may be more clinically relevant in patients with complex GERD and/or impaired esophageal clearance. Future research is needed to elucidate the clinical significance of nocturnal acid breakthrough.
CIMETIDINE:
Cimetidine is a histamine H?-receptor antagonist that reduces the volume, acidity, and quantity of stomach acid secreted in response to stimuli such as food, caffeine, and insulin. It also decreases both basal and nocturnal gastric acid production. Cimetidine is used to treat a variety of gastrointestinal conditions, including pathological hypersecretory syndromes, gastroesophageal reflux disease (GERD), and gastric or duodenal ulcers. Many of the hepatic CYP450 enzyme system's isoenzymes are inhibited by cimetidine. Cimetidine also increases the number of nitrate-reducing organisms and other gastrointestinal bacterial flora.
DRUG PROFILE: [18]
Cimetidine
Molecular Formula: C??H??N?S
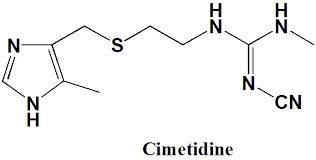
Molecular Weight: 252.34 g/mol
Description: Cimetidine appears as a white crystalline solid.
Category: Antiulcer, Histamine H2-Receptor Antagonist, Gastric Acid Secretion Inhibitor.
Physical Properties:
Appearance: A white to pale yellow crystalline powder.
Solubility: Soluble in both water and ethanol.
pKa: 6.8 (weak base)
Melting point: Around 141-143°C
Storage Conditions: Store at 25°C (77°F), with permissible excursions between 15 and 30°C (59 and 86°F). Protect from light and moisture.
Shelf life: typically, 2-3 years
Dose: 400 mg OD
Mechanism of Action: Cimetidine blocks H2 receptors on gastric parietal cells, thereby reducing both basal and stimulated acid secretion.
Pharmacokinetics:
Absorption: Rapid but limited (~60-70% bioavailability due to first-pass metabolism).
Distribution: Widely distributed, including into gastric tissues.
Metabolism: Primarily in the liver
Excretion: mainly via urine
Half-life: 2 hours
Pharmacodynamics:
The onset of action is within 1 hour, with peak effects around 1-2 hours post-dose
Duration of action: 4-8 hr. Depending on the dose and patient's condition.
Adverse Effects: Headache, dizziness, fatigue, diarrhea.
USES:
Cimetidine is prescribed to treat pathological hypersecretory disorders, duodenal ulcers, stomach ulcers, and gastro-oesophageal reflux syndrome. [19] Another purpose for cimetidine is to prevent or treat heartburn. [20]
MECHANISM OF ACTION:
Cimetidine's mechanism of action is based on the physiology of gastric acid secretion. Gastrin, released from antral G cells; histamine, released from oxyntic enterochromaffin-like cells; and acetylcholine, released from antral and oxyntic neurons due to parasympathetic (vagal) stimulation, are the primary stimuli for gastric acid production [21]. Ghrelin and motilin are additional triggers of gastric secretion. Activation of adenylate cyclase and the subsequent production of cyclic AMP (cAMP) amplify the stimulatory effect of histamine on parietal cells, leading to acid release [22]. This cAMP activates a specific protein kinase, which phosphorylates an unidentified substrate to propagate the stimulatory signal [23]Cholecystokinin, atrial natriuretic peptide, nitric oxide, glucagon-like peptide-1, and somatostatin (secreted by oxyntic and antral D-cells) are the primary inhibitors of acid secretion. [24]Cimetidine, an H2-receptor antagonist, competitively inhibits histamine from activating H2 receptors on gastric parietal cells, which are responsible for secreting intrinsic factors and hydrochloric acid. This effect reduces the amount of stomach acid secreted in response to stimuli such as insulin, food, coffee, and histamine.
EXCIPIENTS:
e.g., microcrystalline cellulose or starch:
Use-Acts as a binder to hold the tablet together during compression.
e.g., Sodium starch glycolate:
Use: Ensures the tablet breaks down properly in the gastrointestinal tract.
e.g., magnesium stearate:
Use—Reduces friction during tablet production and aids in the smooth ejection of tablets from molds.
e.g., lactose or calcium carbonate:
Use to bulk up the tablet to the desired size when the active ingredient alone is not sufficient.
e.g., hydroxypropyl methylcellulose: Sometimes used as a coating agent to improve tablet stability and ease of swallowing
e.g., sodium benzoate
Use Sometimes added to enhance shelf life and prevent microbial growth.
e.g., titanium dioxide or other approved colorants.
Used for aesthetic purposes and to differentiate dosages.
EXPERIMENTAL WORK:
Study of Pre-formulation [25, 26]
Pre-formulation studies focus on the physicochemical characteristics of a drug sample that may influence its performance and the development of its dosage form. This stage represents the initial phase in the drug development process. The primary goal of pre-formulation studies is to create a stable, safe, and effective dosage form by evaluating the drug's kinetic rate profile and its compatibility with other excipients.
Physicochemical characteristics and drug identification—
Drug identification using infrared spectroscopy
The IR spectra of the cimetidine drug samples were compared to the standard IR spectra of pure cimetidine to identify the specific drug.
The drug's physicochemical characteristics and overall appearance
The drug's color, taste, and odor were evaluated.
Drug solubility:
A solubility test was performed to determine the drug's solubility in the dissolution medium and an additional solvent.
Compatibility of drugs and excipients
IR spectroscopy was employed to conduct a study on drug-excipient compatibility.
Precompression Parameters of Powder Blend [27, 28]
1. Bulk and Tapped Density
Ten grams of powder were weighed and added to a 100 mL measuring cylinder. The initial volume was recorded to determine the bulk density. The cylinder was then tapped continuously until no further volume change occurred.
Note the tapped density's final volume. Then, using the provided formula, bulk and tapped density were determined.
Bulk Density = Weight of Powder / Initial Volume
Tapped Density = Weight of Powder / Tapped Volume
2. Carr's Index
Carr's Index, also known as the Compressibility Index, is an important parameter derived from both the tapped and bulk densities. It was used to assess the compressibility of the raw material and blend using the following formula.
Carr's Index (%) = Tapped Density − Bulk Density/Tapped Density × 100
3. The Hausner's Ratio
Hausner's ratio is a measure of a powder's flowability. It is calculated using the following equation.
Hausner’s Ratio = Tapped Density / Bulk Density
4. Angle of Repose
The term 'angle of repose' refers to the maximum angle between the surface of a powder pile and the horizontal plane. Inappropriate flow results from using the angle of repose to measure frictional force. The angle of repose was obtained using the funnel stand method. Using the provided equation, the angle of repose was computed, and the average value was obtained.
tan θ = h/r
θ = tan?¹ (h/r)
where,
θ = Angle of repose h = height of the heap r = radius of the heap
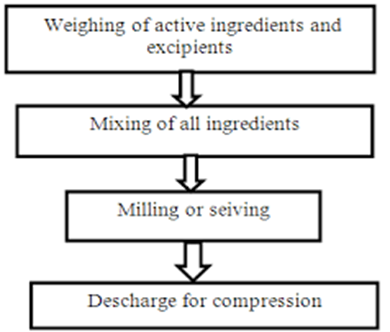
METHOD: [29, 30]
Pre-Blend: To guarantee homogeneity, combine cimetidine with excipients (fillers, binders, and disintegrants) in an appropriate blender.
Lubrication: To prevent excessive shear, add the lubricant (such as magnesium stearate) to the mixture and stir gently.
Compression: The mixture is compressed into tablets using a tablet press. To regulate the release profile and attain the required hardness, modify the compression force.
Coating (optional): To further alter the release profile, apply a coating if necessary.
Post Compression Parameter (Evaluation): [31-34]
General appearance, thickness, hardness, friability, weight fluctuation, and short-term stability studies were all assessed for the manufactured sustained-release tablets.
Appearance-
The primary factor influencing a tablet's acceptability is its organoleptic properties, or overall appearance. It has a significant impact on consumer acceptance. The prepared tablets' organoleptic qualities (taste, color, odor, and shape) were assessed.
The Thickness—
Vernier calipers were used to measure the thickness of six randomly selected tablets from each formulation, and the average value was then calculated.
Hardness—
The term 'hardness' refers to a tablet's resistance to mechanical stress. The tablet’s breaking point is tested through hardness testing. Six tablets from each formulation were tested. A Pfizer hardness tester was used to measure the tablet hardness, expressed in kg/cm².
Friability-
Friability, expressed as a percentage, was determined using the Roche friabilator. Twenty tablets were weighed initially (W-initial). The friabilator, which operates at 25 rpm (100 revolutions per minute), was loaded with the pre-weighed tablets and rotated for four minutes. Afterward, the tablets were removed from the chamber, cleaned, and weighed again (W-final). The percentage of friability was then calculated using the following formula:
Friability (F) = (W initial) - (W final) / (W initial) × 100
Variation in Weight-
Twenty tablets from each formulation were randomly selected and weighed individually. Using the provided formula, the average weight was calculated, and the percentage deviation from the average weight was determined.
Deviation % = (Average Weight – Initial Weight) / Average Weight X 100
APPLICATION OF SUSTAINED-RELEASE CIMETIDINE TABLET:
Cimetidine is effective in the treatment and prevention of gastric and duodenal ulcers because it reduces acid secretion. It also helps control the symptoms of gastroesophageal reflux disease (GERD) by decreasing stomach acidity, which alleviates esophageal irritation.
Sustained-release formulations can offer more reliable acid secretion control in patients with Zollinger-Ellison Syndrome, a rare disorder that results in excessive production of gastric acid. Sustained-release cimetidine is a preventative treatment for stress ulcers in hospitalized patients who are susceptible to stress-related mucosal illness. Acid Indigestion and Heartburn Symptomatic Relief: Compared to immediate-release formulations, it offers longer-lasting relief from acid reflux and heartburn symptoms.Cimetidine can be used in conjunction with other drugs (such as proton pump inhibitors or antacids) for improved therapeutic results.Postoperative Care: To avoid issues from stomach acid, patients may get it after surgery.
CONCLUSION:
The development of sustained-release cimetidine tablets marks a significant advancement in the management of nocturnal acid secretion, offering patients improved symptom control and enhanced quality of life. By effectively prolonging the release of cimetidine, these formulations provide continuous therapeutic levels throughout the night, reducing the frequency of nighttime awakenings and associated discomfort. This innovation not only addresses the limitations of traditional immediate-release formulations but also highlights the potential for tailored treatments that align with patients' needs. As research and clinical evaluations continue to evolve, sustained-release cimetidine tablets may play a pivotal role in the comprehensive management of nocturnal acid-related disorders, potentially leading to improved therapeutic strategies in gastroenterology.
FUTURE SCOPE:
Future investigations may include in?vitro dissolution studies followed by mathematical modeling using Higuchi, Korsmeyer?Peppas, and zero?order kinetics. In vivo bioavailability and pharmacodynamic studies can further validate the clinical significance of sustained?release cimetidine tablets in managing nocturnal acid breakthrough.
REFERENCES:





Sonam B. Chauhan, Nikita R. Sandhan, Akanksha R. Wagh, Akshada U. Pawar, Sakshi B. Bhangre, A Review on Sustained Release Cimetidine Tablets for the Management of Nocturnal Acid Secretion, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 537-546. https://doi.org/10.5281/zenodo.18484557
 10.5281/zenodo.18484557
10.5281/zenodo.18484557
