
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Godavari Institute of Pharmacy, Kolpa, Latur
One of the Controlled released drug delivery through topical route is Transdermal delivery system which can enable to attend steady blood drug level profiles. Transdermal drug delivery system is defined as self-contained discrete dosage forms which are also known as patches. TDDS are dosage forms design to deliver a therapeutically effective amount of drug across a patient’s skin. Now days TDDS treatment is available for diseases like motion sickness, diabetes, arthritis, hormonal replacement, and anti-nausea & Alzheimer treatment. In present review we summarized recent advance, development & various modified techniques in transdermal drug delivery to achieve better therapeutic effect for treatments different diseases.
Transdermal Delivery represent a seductive to oral delivery of medicines and is poised to give a volition to hypodermic injection. TDDS are defined as self-contained separate lozenge forms which are also known as “Patches”.1 TDDS are lozenge form design to deliver a therapeutically effective quantum of medicine across a Cases Skin. For thousands of time people have placed substance on the skin for rectifier’s goods and in ultramodern period a verity of topical expression has been developed to treat original suggestion.2 The first Transdermal system for methodical delivery – a three day patch that delivers scopolamine to treat stir sickness was approved for use in United States in 1979.3 The main ideal of Transdermal medicine delivery system is to deliver medicine into methodical rotation through skin at pre determine rate with minimum inter and intra patient variation.4 A decade latterly nicotine patches come the first Transdermal blockbuster rising the profile of transdermal delivery in medical and for public in general. moment there are Nemours transdermal delivery system for similar medicine as estraclios, Fentanyl, lidocaine and testosterone.5 Combination Patches containing further than one medicine for contraception and hormone relief and ion theoretic and ultra-sonic delivery system for analgesia.6
For understanding the conception of TDDS it's important to know the structure and biochemical features of mortal skin and those characteristics which contributes to the hedge function and the rate of medicine access into the body via skin. The skin acts as a redoubtable hedge to the penetration of medicines and other chemicals; it does have certain advantages which make it an indispensable route for systemic delivery of medicine.7
SKIN ANATOMY:
The following categories apply to the four primary layers of human skin:
The stratum corneum, which is a non-viable epidermis, is the epidermis.
The dermis lying on top subcutaneous fat's deepest layer.
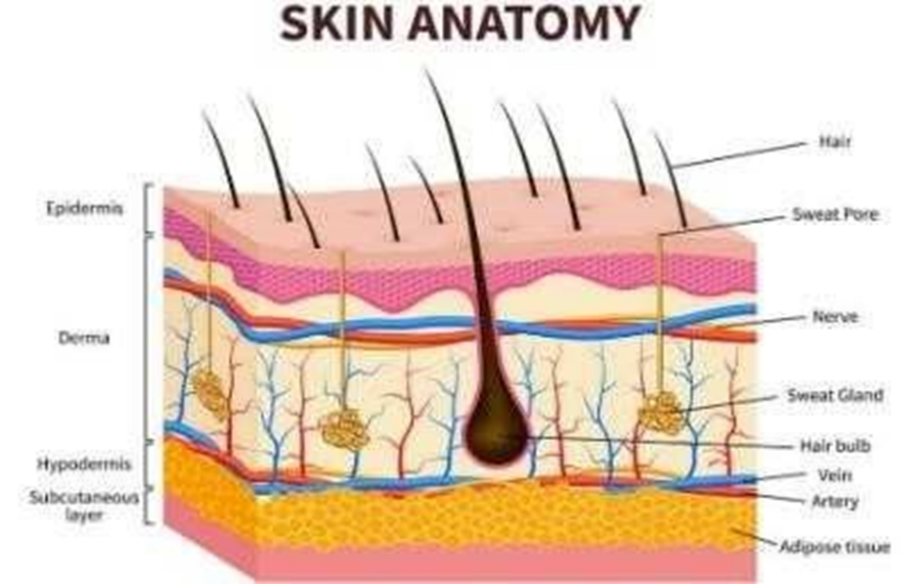
Fig. 1 Skin Anatomy
Number of drugs deliver through TDDS patches for various diseases.
|
BRAND NAME |
DRUG |
MANUFACTURER |
INDICATION |
|
Nicotine |
Nicotine |
Novartis |
Pharmacological Smoking cessation |
|
Marti fen |
Fentanyl |
Nicomed |
Pain relief patch |
|
Orth Euro |
Norelgostromine/ Ethinyl Oestradiol |
Ortho-McNeil |
Postmenstrual syndrome |
|
Nupatch 100 |
Diclofenac diethylamino |
Zydus cedilla |
Anti-inflammatory |
|
Nepro |
Rioting |
UCB and Schwarz Pharma |
Early-stages idiopathic Parkinson’s diseases |
|
Alora |
Oestradiol |
Thera/ Thec/ Proctor and Gamble |
Postmenstrual syndrome. |
|
Anoderm |
Testosterone |
Thera/ Tech Giaxosmith kine |
Hypogonadism Inj.(male) |
|
Nitro disc |
Nitro-glycerine |
Robert pharmaceuticals |
Angina pectoris |
|
Transdermal cop |
Scopolamine |
Alza/ Novartis |
Motion sickness |
|
Nclvellets |
Estragon/progesterone |
Ethical Holdings/ Schering’s |
Hormones replacement therapy |
Epidermis:
The whole exterior of the body is covered in a layered, continuously self-renewing squamous epithelium called the epidermis. It is primarily made up of two types of cells: living or viable cells in the malpighia layer (the viable epidermis), and dead cells in the stratum corneum, also known as the horny layer.1The four distinct layers of viable epidermis are further classified.8
Stratum corneum:
The horny layer, which is the skin's outermost layer, is present here. Chemical substances cannot move both inward and outward because of the rate limiting barrier. The horny layer's constituents—75–80% proteins, 5–15% lipids, and 5–10% ondansetron material on a dry weight basis—have a significant impact on the barrier properties of the layer. When fully hydrated, stratum corneum expands to a thickness of several times its normal 10 mm thickness. Despite being somewhat impermeable, it is flexible. The design of the horny layer can be replicated using lipid mortar and protein bricks (figure 3).It is made up of horny skin cells (corneocytes) that are joined together by desmosomes, which are protein-rich extensions of the cell membrane. The lipid matrix that surrounds the corneocytes significantly influences how permeable the skin is to substances.9
Viable epidermis
Under the stratum corneum, this layer ranges in thickness from 0.06 mm on the eyelids to 0.8 mm on the palms. Stratum lucidum, stratum granulosum, stratum spinosum, and stratum basale are some of the layers that make up the interior. The loss of dead horny cells from the skin's surface is compensated for by the basal layer's constant cell regeneration through mitosis. The top layer of the stratum corneum is formed by keratinization of the outwards migrating cells of the basale layer, which results in morphological and histochemical alterations.10-11
Dermis
Nerves, lymphatic veins, and blood vessels make up the dermis, a 3–5 mm thick layer of connective tissue that sits directly beneath the epidermis. It is essential for the cutaneous blood supply to regulate body temperature.12
In addition, it nourishes and oxygenates the skin while eliminating toxins and waste. In order for most molecules to pass through the skin barrier, capillaries must be within 0.2 mm of the skin's surface. As a result, the blood supply keeps the dermal concentration of permeate at an extremely low level. The resulting concentration difference across the epidermis then acts as the primary driving force for transdermal permeation. Although the dermal barrier may be significant when delivering highly lipophilic molecules, this layer is frequently thought of in terms of transdermal drug delivery as essentially gelled water and thus provides a minimal barrier to the delivery of most polar drugs.13
Hypodermis
The dermis and epidermis are supported by the subcutaneous fat tissue, or hypodermis.It serves as a location for fat storage. This layer offers nutritional support, mechanical protection, and assistance with temperature regulation. It may contain sensory pressure organs and major blood vessels and nerves that supply the skin .A medication must penetrate all three layers and reach the bloodstream in order to be administered transdermally.13
PATHWAYS OF DRUGS ABSORPTION THROUGH THE SKIN:
Trans follicular route is the shortest pathway that drugs has to follow to reach the systemic circulation that provide a large area for diffusion of drugs.14
Drugs delivering through this route passes from corneocytes which has highly hydrated keratin creating hydrophilic pathways. The drugs passes through the corneocytes of stratum corneum.15
In intercellular pathway the drug diffuses through the continuous lipid matrix present between cells.16
TRANSDERMAL PATCH

Fig. 2 Transdermal Patch
A transdermal patch, also known as a skin patch, is an adhesive patch that contains medication and is applied to the skin in order to deliver a specific dose of medication through the skin and into the bloodstream. In December 1979, the U.S. Food and Drug Administration approved the first prescription patch for motion sickness that contained scopolamine. The nicotine patch, which releases nicotine to aid in quitting tobacco use, was the transdermal patch with the highest sales in the United States. In 2007, Europe approved the first commercially available vapour patch to help people quit smoking.13
Various other patches, such as nitro-glycerine patches for angina and lidocaine patches marketed under the name Lidoderm, which reduce shingles-related peripheral pain, are also offered on the market. As an analgesic for moderate to severe chronic pain, buprenorphine is sold under the brand name Bu Trans. In addition, it is now frequently used off-label to treat chronic pain and the pain from recent injuries. A topical NSAID called Elector (Diclofenac Epolamine) patch is used to alleviate acute pain from mild sprains, strains, and contusions.17
Additionally, it is used to treat fibromyalgia, arthritis, and other chronic conditions that benefit from NSAIDs in terms of pain and inflammation. ADHD, or excessive activity. The FDA revealed in 2005 that they are looking into reports of fatalities and other grave adverse events connected to narcotic overdose. Fentanyl transdermal patch users who use Duragesic for pain relief.18
The transdermal patch's constituent parts:
A polymer matrix/drug reservoir, the active ingredient (drug), permeation enhancers, pressure-sensitive adhesive (PSA), backing laminates, release liner, and additional excipients such as plasticizers and solvents are the main components of transdermal patches.19
Transdermal drug delivery systems are built on polymers. Transdermal delivery systems consist of multilayered polymeric laminates, in which a drug reservoir or drug polymer matrix is positioned between two polymeric layers. The inner polymeric layer acts as an adhesive and/or rate-controlling membrane, while the outer impermeable backing layer stops drug loss via the backing surface.20
When attempting to meet the various requirements for the creation of reliable transdermal delivery systems, polymer selection and design must be taken into account. The biggest issue is designing a polymer matrix, which is followed by optimizing the drug-loaded matrix in terms of its adhesion cohesion balance, physical and stability with other system components as well as with skin.21
The polymers utilized for TDDS can be classified as
The drug must meet the necessary physicochemical and pharmacokinetic requirements, which are the main requirements for TDDS. Drugs that undergo extensive first-pass metabolism, have a limited therapeutic window, or have a short half-life that necessitates frequent dosing and results in noncompliance have a lot to gain from transdermal patches.25
Permeation enhancers interact with the proteins or lipids that make up the structural elements of the stratum corneum in order to increase its permeability and increase the therapeutic levels of the drug. It is believed that the chemical enhancers' partial leaching of the epidermal lipids, which improves the skin's conditions for wetting as well as for trans-epidermal and trans-follicular penetration, is the cause of the enhancement in the absorption of oil-soluble drugs. The miscibility and solution characteristics of the enhancers may be the reason for the increased transdermal penetration of watersoluble.25
4.Pressure-sensitive adhesive (PSA):
A PSA keeps the patch and the skin's surface in close proximity. It should be aggressively and permanently tacky, adhere with no more than finger pressure, and exert a strong holding force. Adhesives based on silicon, polyisobutylene, and polyacrylates are among them, according to World Journal of Pharmacy and Pharmaceutical Sciences. The choice of adhesive is influenced by a number of factors, including the drug composition and patch design. PSA shouldn't affect drug release and should be compatible with physicochemical and biological processes. The PSA may be placed on the device's face or inside the device's back and extending outward.26
5. Backing laminate:
Support is the backing laminate's main purpose in life. Excipients, medications, or permeation enhancers may diffuse through the backing layer or additives may leach out as a result of extended contact between the backing layer and the excipients. Layer should be chemically resistant and excipients compatible. They ought to have a slow rate of moisture vapour transmission. They must have optimal elasticity, flexibility, and tensile strength.27
6. Release liner:
The release liner stops contamination during storage as well as drug loss that has migrated into the adhesive layer. Therefore, rather than being a component of the dosage form for dispensing the medication, it is viewed as a part of the primary packaging material. The base layer of the release liner can be either non-occlusive or occlusive, and the release coating layer is made of silicon or Teflon. Polyester foil and metalized laminate are additional materials used to make the TDDS release liner.28
7. Other excipients:
Drug reservoirs are made using a variety of solvents, including dichloromethane, acetone, chloroform, methanol, and methanol. Additionally, plasticizers like dibutyl phthalate, triethyl citrate, polyethylene glycol, and propylene glycol are added to the transdermal patch to give it plasticity.29
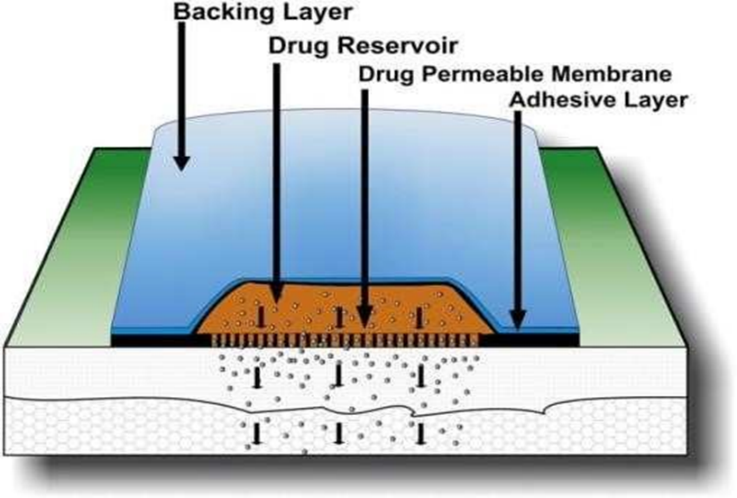
Fig. 3 Constituent Parts of Transdermal Patches
DESIGN OF TRANSDERMAL DELIVERY SYSTEM:
The drug is dissolved or dispersed in an inert polymer matrix, which serves as support and a platform for drug release, as the fundamental component of any transdermal delivery system. The patch system's two fundamental designs, which determine the drug release characteristics and patch behaviour, are as follows:
Matrix or Monolithic: The inert polymer matrix binds with the drug and controls its release from the device.
Reservoir or Membrane: The polymer matrix does not control the release of drugs. Instead, a rate- regulating membrane that is sandwiched between the drug matrix and the adhesive layer acts as the rate-limiting barrier for drug release from the device.30
PREPARATION OF TRANSDERMAL PATCHES
There are several ways to prepare transdermal medication delivery patches.
Mercury Substrate Method:
This method involves dissolving the required amount of drug in a solution of polymer and plasticizer. To achieve a uniform dispersion, the previously indicated combination needs to be agitated for some time. It should then be set aside until all air bubbles have been eliminated before being poured into a glass ring that will be placed over the mercury surface in a glass petri dish. By putting an inverted funnel over the petri dish, the rate at which the solvent evaporates can be managed. It is necessary to store the dried-out films in a desiccator.
Circular Teflon Mould Method:
In an organic solvent, solutions with different ratios of polymers are used. The drug is dissolved in half as much of the same organic solvent as was calculated. Drug polymer solution contains a plasticizer. After thoroughly stirring the mixture, it should be poured into a Teflon mould that is circular. Inverted glass funnels on Teflon moulds were used to control the rate of solvent vaporisation. The solvent is allowed to evaporate for 24 hours. The dehydrated films must be kept in a desiccator.
Glass Substrate Method:
The polymeric solutions are set aside to swell before the necessary amounts of plasticizer and drug solution are added, followed by a 10-minute stirring period. It is also allowed to stand for a while to release any trapped air before being poured into a dry, clean an umbra Petri plate. Inverting a glass funnel over the petri plate regulates the rate of solvent evaporation. The dried films are removed from the overnight drying process and placed in a desiccator.31
By Using IPM Membranes Method
This method involves dispersing the drug over a 12-hour stirring period in a solution of water and propylene glycol that contains carbomer 940 polymers. Triethanolamine will be added to the dispersion to neutralise it and make it viscous. If the drug is very poorly soluble in aqueous solution, a buffer pH 7.4 can be used to create solution gel. After formation, the gel will be incorporated into the IPM membrane.32-33
By Using EVAC Membranes Method:
Rate control membranes made of polyethylene (PE), ethylene vinyl acetate copolymer (EVAC), and 1% Carbopol reservoir gel can be used to prepare the target transdermal therapeutic system. When making a gel, propylene glycol is used if the drug is not soluble in water. The drug is dissolved in propylene glycol, and then Carbopol resin is added to the mixture before it is neutralised with 5% w/w sodium hydroxide solution. The medication is applied to a backing layer sheet that covers the designated area and is in the form of a gel. The gel will be covered with a rate-regulating membrane, and the edges will be heated to seal, resulting in a leak-proof device.34
Aluminium Backed Adhesive Film Method:
Transdermal drug delivery devices may produce unstable matrixes if the loading dose exceeds 10 mg. Using adhesive film with an aluminium backing is a good option. Due to the fact that most drugs and adhesives are soluble in chloroform, it is the preferred solvent for preparation of the same. Adhesive material will be added and dissolved in the drug solution after the drug has been dissolved in chloroform. Aluminium foil is used to line a specially made aluminium former, and snugly fitting cork blocks are used to blank off the ends.28
Asymmetric TPX Membrane Method:
A prototype patch can be created using a heat sealable polyester film (type 1009, 3m) with a 1 cm-diameter concave backing membrane. A TPX "poly (4-methyl-1pentene)" asymmetric membrane is used to cover the concave membrane, which is then filled with the drug sample and sealed with adhesive.
EVALUATION TEST OF TRANSDERMAL PATCH
Studies on Drug Excipient Interactions:
For the product to function properly, the medication and excipients must get along. Stable product, so it's critical to find any possible defects. Physical and chemical forces interacting One category of research that examines human interaction is the interaction studies study. In this technique, thermal analysis is frequently performed. Assay, melting, and other physiochemical wave numbers, maxima, etc. are compared with FT-IR. Wwith UV and chromatographic procedures.26-27
Drug Content:
A specific volume of an appropriate solvent needs to be used to dissolve a section of the patch. The solution will next be filtered via a filter media. Determine the drug's composition using the proper technology (UV or X-rays). The HPLC method). Every sample value represents the average of three values.
Patch Thickness:
By using a digital micrometre to measure the patch's thickness at multiple locations, the average thickness and width of the drug-loaded patch are found. To confirm the thickness of the constructed patch, find the standard deviation for the same.
Moisture loss:
each of the generated films, then store them in a calcium chloride filled desiccator at 40?C. The movies will be screened the next day. Utilizing the procedure below, reweigh and determine the percentage of moisture loss [13]. % Moisture Loss = [Start weight–End weight] × 100.31
Swell ability:
After being weighed, the 3.14 cm2 patches were placed in a petri plate with 10 ml of double-distilled water to drink. A rise in mass. Patches were chosen at prearranged intervals until a decision was made. It was found that the weight did not change. To calculate the swelling degree (S), use the formula S(%) = Wt.-Wo/Wo ×100. Wt. is the weight of the patch at time t, Wo is the weight of the patch at time zero, and S is the percentage swelling.
In- vivo Studies:
The most accurate depiction of a drug's effectiveness comes from in vivo studies. In-vitro research allows for the full consideration of variables that are not possible to consider. Studies on in vivo research have been conducted. To carry out TDDS, the following techniques can be tested in vivo: Animal-based models Human race volunteers.32
Models of Animals:
Mice, hairless rats, and other animals are the most often employed animal species for transdermal drug delivery system testing. Examples of hairless animals include guinea pigs, hairless dogs, hairless rhesus monkeys, and rabbits.
Human Models:
The last stage in developing a transdermal patch for pharmaceutical pharmacokinetics is gathering human models. Pharmacodynamic information is gathered from a group of human volunteers following the application of the patch. Among other things, clinical trials have been conducted to ascertain efficacy, risk, side effects, and patient compliance.
Stability Studies:
Stability studies must be conducted by storing the TDDS in compliance with ICH regulations. Samples were maintained at 40.5% RH and 40.5% C for six months. At 0, 30, 60, 90, and 180 days beforehand, samples were collected. Carefully review the contents of the drug.33
OVERALL CLINICAL ASPECTS IN THE APPLICATION OF TDDS:
The patient should be informed of the general rules listed below. To help the skin regain its normal permeability and to prevent skin irritation, the application site should be rotated. To clean, dry skin that is largely hair-free and not oily, inflamed, irritated, or broken skin, TDDS should be applied. Drug permeation time can be sped up on moist or wet skin. Skin that is too oily can make patches less adherent. If hair is present at the site, it should be carefully cut, rather than wet shaved or removed with a depilatory agent, as this may affect the rate and extent of drug permeation by removing stratum corneum. It is not advisable to apply skin lotion where it will be used. Mainly because lotions can change the drug's partition coefficient and have an impact on the skin's hydration. In order to preserve the integrity of the system, the patient shouldn't physically alter the TDDS. Take care not to touch your fingertips when removing the protective backing. For about 10 seconds, press the heel of your hand firmly against the TDDS skin site. An area where a TDDS won't be exposed to movement or clothing rubbing off should be chosen for placement. TDDS should be left on while swimming, taking a shower, or bathing. A TDDS should be used as directed by the product's instructions, which include wearing it for the recommended amount of time before removing it and changing to a new system. Following the application of a TDDS, the patient or carer should wash their hands. When handling the system, the patient shouldn't touch their mouth or rub their eyes.The patient should request revaluation if they show signs of sensitivity or intolerance to TDDSs or experience excessive skin rashes.After removing a used TDDS, the adhesive layer should be folded in half to prevent reuse. In a way that is safe for kids and pets, the used patch was disposed of. applying a transdermal patch Use a different application site each day to prevent skin sensitivity. The recommended rotation is Day 1: Upper right arm, Day 2: Upper right chest, Day 3: Upper left chest, and Day 4: Upper left arm, then repeat from Day 1.35
CONDITIONS IN WHICH TRANSDERMAL PATCHES ARE USED:
When a patient needs an alternative drug delivery method because they have intolerable side effects (like constipation) from oral medication and are unable to swallow it (due to dysphagia), they turn to transdermal patches. where reliable administration could enhance the control of the pain. Patients with cognitive impairment or those unable to use their analgesia to self-medicate for other reasons may find this helpful.36
REQUIREMENTS FOR NOT USING TRANSDERMAL PATCHES:
Transdermal patches should not be used in the following situations:
Where the dosage requirement is equal to or less than 30 mg/24 hours.37
REFERENCES



Wasim Bagwan, Kumbhar Shivam, Kotsulwar Sohan, Nilewad Mahesh, A Review on Transdermal Drug Delivery System, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 2576-2586. https://doi.org/10.5281/zenodo.16089445
 10.5281/zenodo.16089445
10.5281/zenodo.16089445