Department of Pharmaceutics, Konkan Gyanpeeth Rahul Dharkar College Of Pharmacy & Research Institute, Karjat
Gastroretentive floating drug delivery systems (FDDS) overcome rapid gastric emptying to enhance bioavailability of drugs with narrow absorption windows. This review comprehensively examines FDDS formulation strategies, evaluation parameters, therapeutic applications, recent advances, and influencing factors. Effervescent systems utilize gas-generating agents (sodium bicarbonate, citric acid) with swellable polymers (HPMC, sodium alginate), while non-effervescent approaches employ low-density hydrogels and hollow microspheres. Key evaluation includes pre/post-compression parameters, buoyancy lag time, dissolution kinetics (zero-order, Higuchi models), and ICH stability testing. FDDS enable sustained release, site-specific gastric delivery (H. pylori eradication), bioavailability enhancement (metformin, ciprofloxacin), and benefits for pediatric/geriatric populations. Recent innovations feature stimuli-responsive polymers, nanocomposite hydrogels, nanotechnology-based carriers, and Quality by Design (QbD) optimization using factorial/DoE approaches. Physiological factors (gastric pH, motility), formulation variables (polymer ratio, density), and patient characteristics modulate performance. Future directions emphasize AI-driven design, theranostics, and patient-centric formulations for superior gastroretention and therapeutic outcomes..
Overview of GRDDS-
Gastro-retentive Drug Delivery Systems (GRDDS) are designed to keep dosage forms in the stomach for a prolonged period, supporting controlled release and improved absorption in the upper GIT [6]. They are especially useful for drugs with a narrow absorption window or instability at intestinal pH [7]. Floating Drug Delivery Systems (FDDS) are the most common type; they have a lower density than gastric fluids, allowing them to remain buoyant and provide sustained drug release [1,2]. Although the oral route is convenient and widely accepted, it is limited by rapid gastric emptying, enzymatic degradation, and short residence time [3]. These factors, along with physiological and patient-specific variations, reduce the bioavailability of drugs absorbed in the upper GIT [4]. Floating systems help overcome these issues by extending gastric residence time, improving absorption, and enabling localized action in the stomach [5]. These review highlights recent developments in floating formulations, including polymers, buoyancy mechanisms, release characteristics, and emerging technologies such as nanotechnology and smart polymers, along with regulatory and practical considerations [8].
Importance and Challenges in Oral Drug Delivery-
The oral route is preferred for its simplicity, comfort, and cost-effectiveness; however, its performance is affected by variable gastric emptying, changing pH, enzymatic degradation, and first-pass metabolism [3]. These factors limit the absorption of drugs dependent on stomach or upper intestinal sites. Physiological variability, dosage form characteristics, and patient-related factors further contribute to inconsistent bioavailability [4]. Floating GRDDS improves drug absorption and therapeutic effects by prolonging gastric retention and maintaining controlled release. Modern development emphasizes selecting appropriate polymers and using Quality by Design (QbD) for consistent formulation performance [5].
Aim and Scope of the Review-
Objectives-To present a concise review of advancements in gastroretentive floating drug delivery systems (GRFDDS) [6][7][8].
Scope Includes-
MATERIALS & METHODS -
Floating formulations typically employ a combination of polymers, gas-generating agents, and excipients to achieve buoyancy and controlled release. Frequently used materials include:
Instruments-
Experimental studies commonly use standard pharmaceutical processing and testing tools. The key instruments included:
Polymer Categories-
Polymers used in floating drug delivery systems can be broadly classified into three categories based on their origin and functional properties. Their primary roles are summarized as follows [3,4,13]:
TABLE 1- POLYMER CATEGORIES
FUNDAMENTALS OF FLOATING DRUG DELIVERY SYSTEM (FDDS)-
|
Type |
Examples |
Role in Floating system |
|
Natural release |
Alginate, Chitosan |
Form hydrogels, enhance buoyancy, sustain release . |
|
Semi-synthetic release |
HPMC, CMC |
Produce swellable matrices, control drug release. |
|
Synthetic |
Eudragit RLPO, PMMA |
Provide structural stability, modulate permeability. |
Definition and Mechanism of Gastro-retention-
Floating Drug Delivery Systems (FDDS) are oral formulations engineered to possess a bulk density lower than gastric fluid, allowing them to remain buoyant in the stomach for extended periods [6]. By remaining in the upper gastrointestinal region, the system can slowly release the drug at the optimal absorption site [7]. Gastroretention is achieved by creating low-density structures. In effervescent designs, agents such as sodium bicarbonate react with gastric acid to liberate carbon dioxide, which is trapped inside a hydrated polymer matrix [8]. This trapped gas decreases the density of the dosage form and promotes flotation. Non-effervescent systems rely on swellable or low-density polymers that hydrate, expand, and entrap air, further supporting buoyancy and preventing early gastric emptying [9]. Maintaining the formulation in the stomach overcomes rapid gastric transit and reduces variability in absorption. FDDS improves bioavailability, provides steadier drug levels, and enhances patient adherence, especially for drugs with narrow absorption windows in the stomach or proximal intestine [6,7].
Classification of FDDS-
Floating systems are broadly divided into two groups—effervescent and non-effervescent—based on the mechanism by which buoyancy is generated and sustained within the stomach [12].
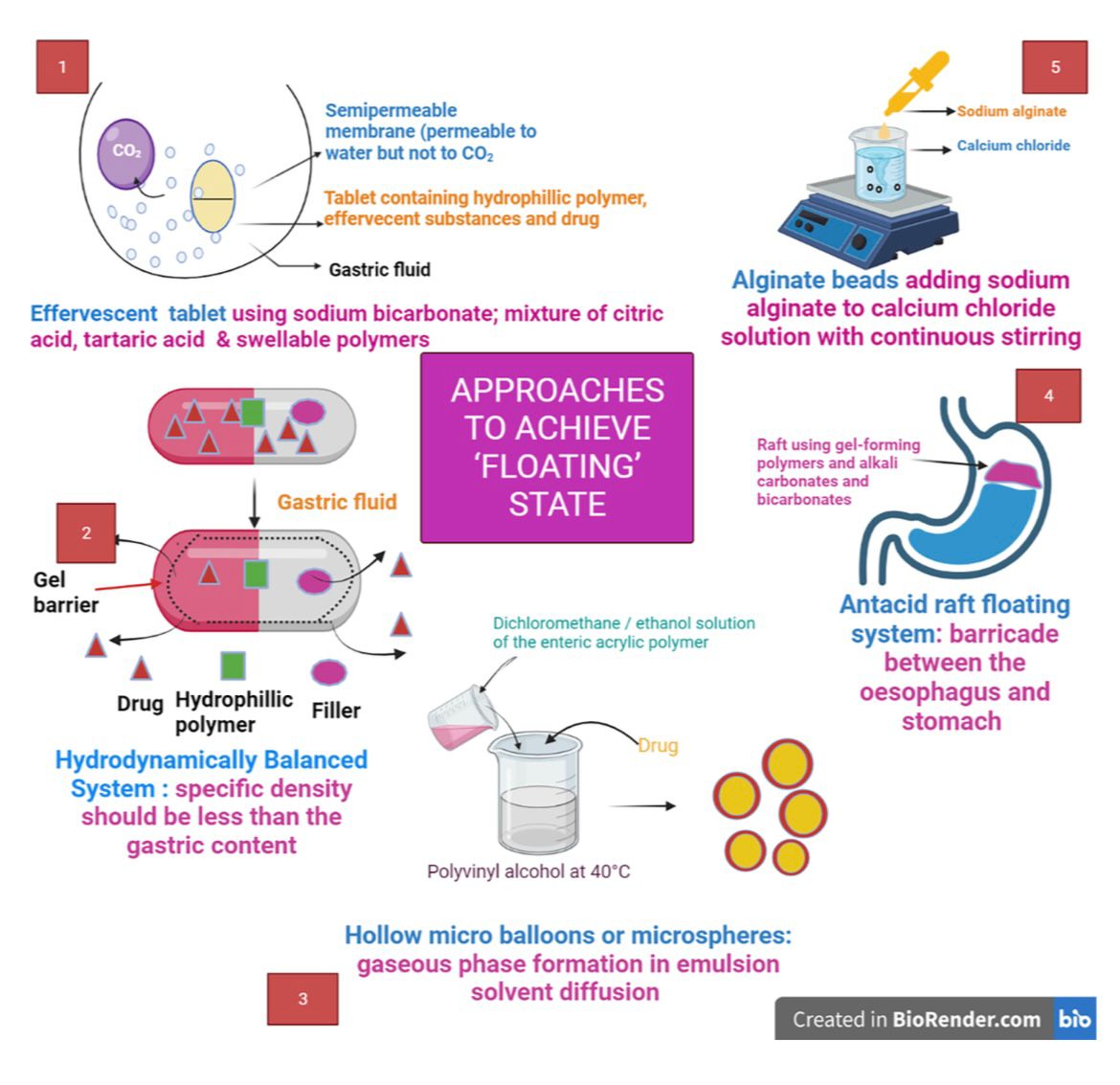
FIG 1- EFFERVESCENT AND NON-EFFERVESCENT FDDS APPROACHES
Effervescent Systems-
Effervescent floating systems incorporate gas-forming components such as sodium bicarbonate, citric acid and tartaric acid. These materials react with acidic gastric fluid to release carbon dioxide, which becomes embedded within the hydrated polymer network, lowering density and enabling floatation [10]. This category includes floating tablets, capsules, beads, and microsphere [11]. Effervescent systems remain the most widely investigated type of FDDS because of their simple formulation requirements and predictable buoyancy behavior [13].
Non-Effervescent Systems-
Non-effervescent floating systems do not rely on chemical reactions to generate gas. Instead, they employ polymers such as HPMC, polysaccharides, and hydrogel-forming materials that swell upon contact with gastric fluids. Swelling forms a porous gel layer that traps air and maintains buoyancy.These systems include hydrodynamically balanced systems, raft-forming systems, and certain types of floating microspheres. Their stability, minimal gas production, and sustained drug-releasing nature make them suitable for prolonged gastric retention [12].
Floating Microspheres & Hollow Microballoons -
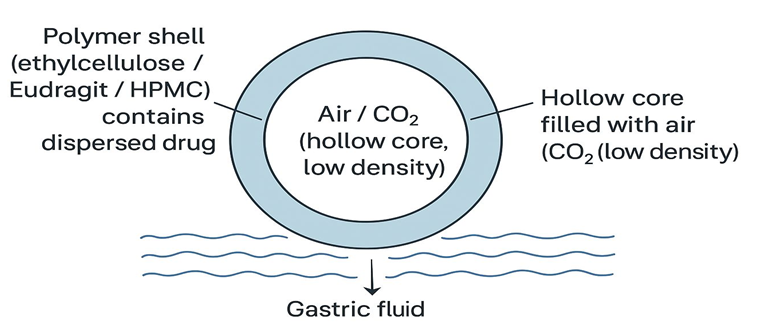
FIG 2- FLOATING MICROSPHERES (HOLLOW MICROBALLOON)
Low-density, hollow multiparticulates made of polymers such as ethylcellulose, eudragit, or HPMC are known as floating microspheres. Although the polymer shell allows for controlled release, its internal air/CO? chamber allows for buoyancy [22]. They are often produced by spray-drying, coacervation, or solvent evaporation [23]. Long-term stomach retention and enhanced absorption of medications restricted to the upper GI tract are guaranteed by their lightweight, porous nature [22].
Matrix Tablets and Gas?Generating Systems-
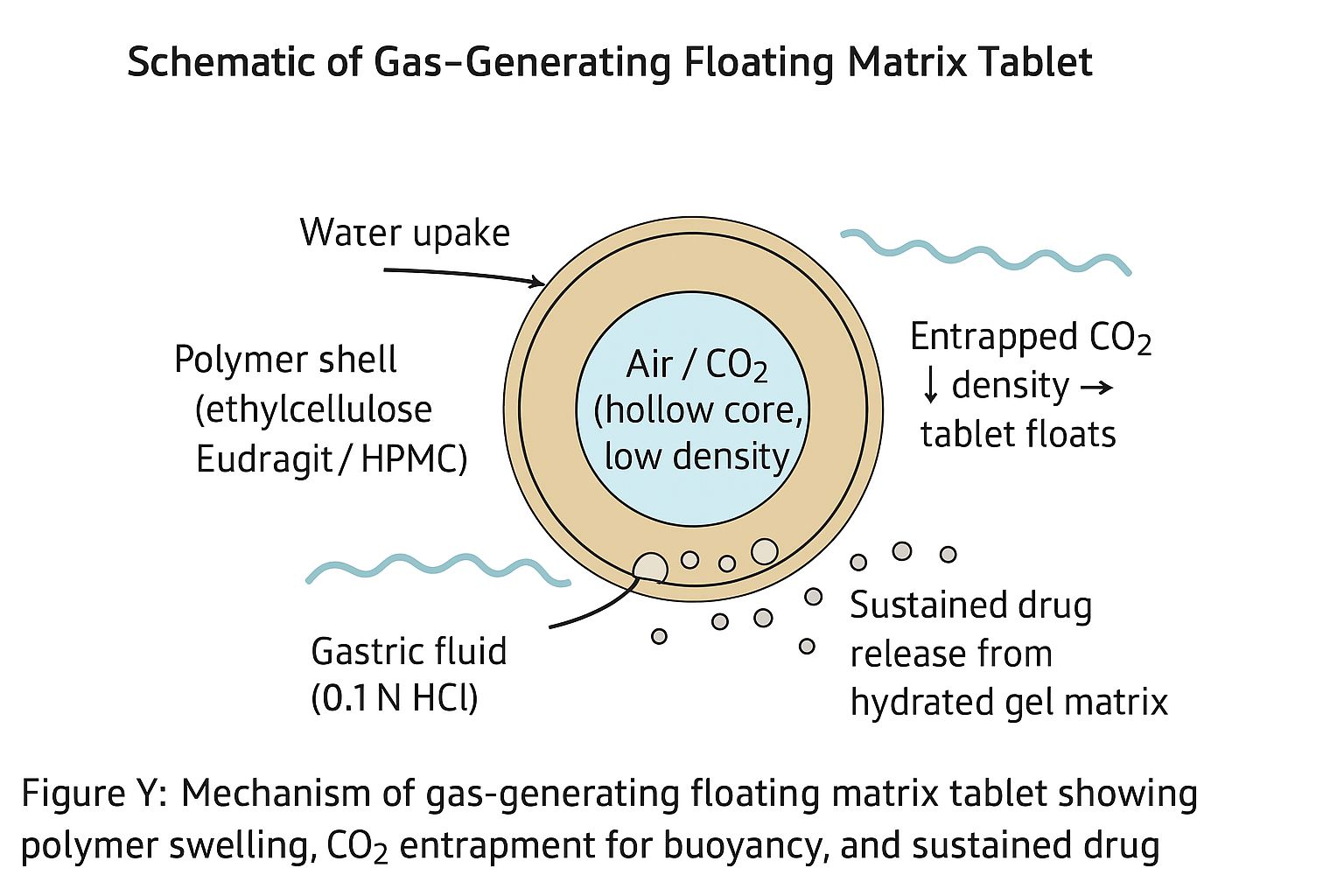
FIG 3- GAS-GENERATING FLOATING MATRIX TABLET
Gas?generating matrix tablets consist of drugs dispersed in swellable polymers (e.g., HPMC, Carbopol and sodium alginate) plus effervescent agents such as sodium bicarbonate and citric/tartaric acid [11]. On contact with gastric fluid, the matrix hydrates to a gel and generated CO? becomes entrapped, lowering tablet density so it floats while releasing drug in a sustained manner [12]. This approach is simple, cost?effective, and widely used for local or narrow?window drugs [14]. Proper optimization of polymer level and effervescent ratio is essential to balance buoyancy, mechanical strength, and release kinetics, avoiding premature disintegration or dose dumping [11].
Emulsion based techniques-
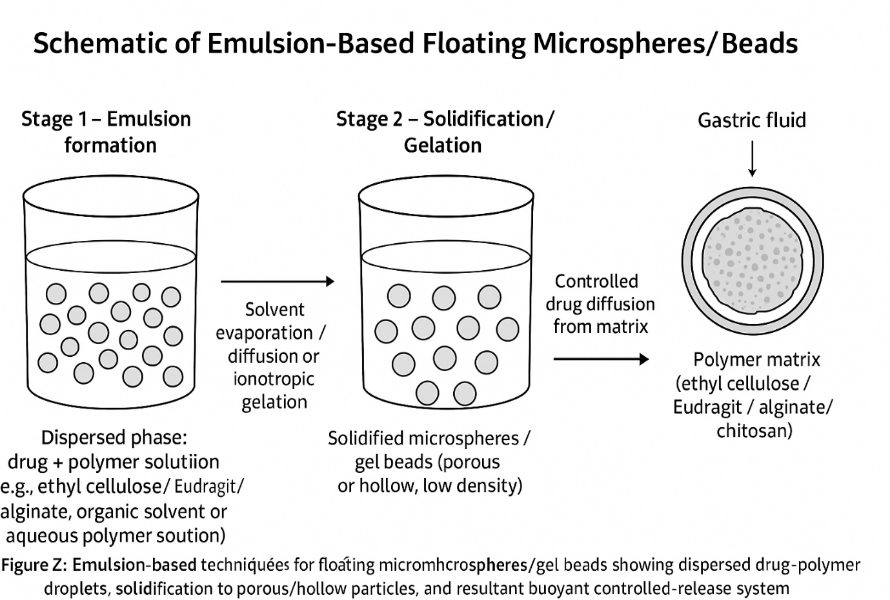
FIG 4-EMULSION-BASED FLOATING MICROSPHERES/BEADS
Emulsion methods (O/W or W/O) are used to prepare floating microspheres or gel beads with good buoyancy and controlled drug release [17]. Drugs and polymers (e.g., ethyl cellulose, Eudragit and carbomers) are dissolved or dispersed in an organic phase, emulsified into an aqueous phase and then solidified by solvent evaporation or ionotropic gelation to form porous or hollow low?density particles [21]. Alginate or chitosan emulsions can be cross?linked with calcium to form gel beads, and variables such as particle size, polymer concentration, and stirring speed govern floatation, loading, and release [23]. This technique is scalable and suitable for both hydrophilic and hydrophobic drugs, however organic solvents must be thoroughly removed to ensure safety [21].
Ionotropic gelation and solvent evaporation-
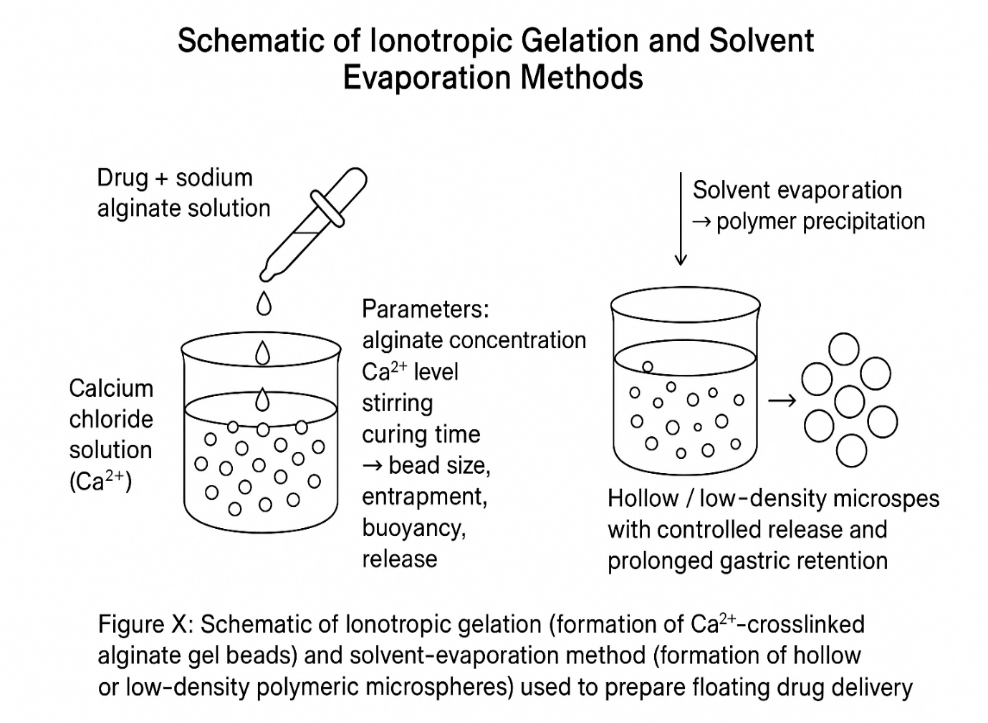
FIG 5- IONOTROPIC GELATION AND SOLVENT EVAPORATION
Ionotropic gelation uses polymers such as sodium alginate that cross?link with multivalent cations (e.g., Ca²?) to form drug?loaded, low?density gel beads under mild aqueous conditions. Process variables such as polymer and cross?linker concentration, stirring, and curing time control bead size, entrapment, buoyancy, and release [15]. Solvent evaporation dissolves or disperses drugs and polymers (ethyl cellulose, PMMA, Eudragit) in a volatile organic solvent, forms an emulsion, and removes the solvent to obtain hollow or low?density microspheres with prolonged gastric retention and controlled release [16]; Both methods are scalable, but require careful control of gelation conditions and complete solvent removal, respectively [18].
Quality by Design (QbD) and Experimental Optimization Tools-
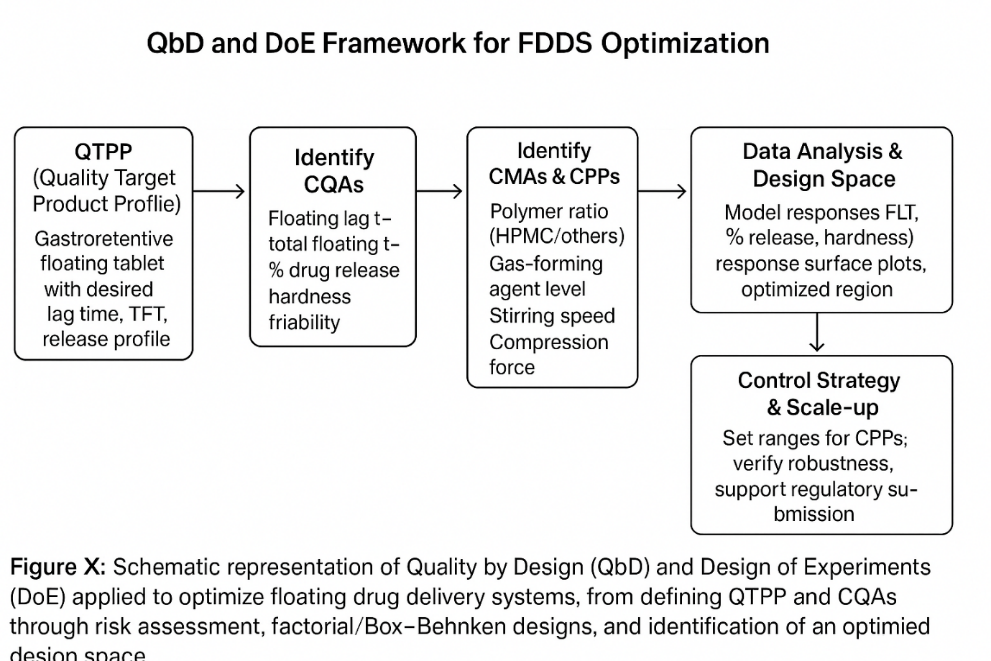
FIG 6- QBD AND DOE FRAMEWORK FOR FDDS OPTIMIZATION
Quality by Design (QbD) builds quality into FDDS by first defining critical quality attributes (CQAs) and critical process parameters (CPPs), then using risk assessment and design of experiments (DoE) to establish a design space that ensures consistent performance [1]. Experimental designs such as factorial, Box–Behnken, and central composite models evaluate how variables such as polymer ratio, gas?forming agent level, and stirring speed influence floating lag time, drug release, and tablet strength. In Mahale et al.’s 3² design for dapsone floating tablets, polymer and gas?forming concentrations emerged as key determinants of buoyancy and release, allowing an optimized formulation with improved efficacy [22]. Overall, QbD and DoE minimize trial?and?error, support robust scale?up, and strengthen regulatory submissions by demonstrating thorough process understanding.
EVALUATION PARAMETERS-
Pre-Compression Parameters (Flowability, Density, etc)-
Pre?compression studies ensure that powder blends have adequate flow and packing for uniform tablet production and consistent drug content. Key tests include angle of repose, Carr’s index, and Hausner ratio to assess flowability; an angle of repose <30°, Carr’s index <15%, and Hausner ratio <1.25 generally indicate good flow [25]. Bulk and tapped densities describe packing behavior and are used to calculate compressibility, whereas moisture content (by LOD or Karl Fischer) is controlled to prevent clumping, poor flow, and drug degradation [26]. Optimizing these parameters yields blends suitable for compression or encapsulation, supporting uniform buoyancy and release in FDDS.
Post?Compression Parameters (Hardness, Friability, Weight Variation)-
Post?compression tests confirmed the mechanical strength and dose uniformity of the floating tablets. The hardness (typically 3–6 kg/cm²) must be sufficiently high to withstand handling without impairing drug release [26]. Friability (<1% weight loss) indicates resistance to abrasion, and weight variation testing verifies that individual tablet weights and therefore doses-remain within pharmacopoeial limits [27]. Together, these parameters ensured robust tablets with reliable floating behavior and dosing.
Buoyancy and Floating Lag Time Studies-
Buoyancy and floating lag time directly reflect the gastroretentive performance of FDDS. Buoyancy is assessed as total floating time of the dosage form in 0.1 N HCl at 37±0.5°C, while floating lag time (FLT) is the time taken to rise to the surface after immersion [28]. These metrics depend on the polymer type and level, gas?generating agents, density, and porosity, and are optimized to achieve rapid onset of floatation and prolonged gastric residence with controlled drug release.
In Vitro Drug Release and Release Kinetics-
In vitro dissolution (often USP Type II in 0.1 N HCl at 37±0.5°C) provides the drug release profile and allows comparison between formulations [29]. Cumulative release data are fitted to models such as zero?order, first?order, Higuchi, Korsmeyer–Peppas, and Hixson–Crowell to elucidate mechanisms such as diffusion, erosion, or anomalous transport [30]. Understanding the kinetics guides selection of polymer type, concentration, and matrix design to meet desired sustained?release and therapeutic targets.
Micromeritic and Morphological Evaluations-
Micromeritic and morphological properties influence the manufacturability and in vivo behavior of FDDS. Particle size and distribution affect flow, compressibility, release rate, and buoyancy, and are measured by sieving, laser diffraction, or microscopy [26]. SEM provides insight into shape, surface texture, and porosity; smooth, spherical, and porous particles generally show better flotation and controlled release [27]. Bulk/tapped density and flow indices (angle of repose, Carr’s index, Hausner ratio) further characterize powder behavior, while porosity, void volume, and swelling index (weight gain in simulated gastric fluid) are critical for lowering density, enhancing buoyancy, and modulating diffusion [28].
Stability Studies-
Stability testing confirmed that the FDDS maintained their physical integrity, drug content, buoyancy, and release characteristics over their shelf life. According to ICH guidelines, products are stored under accelerated (e.g., 40±2°C/75% RH±5%) and long term (25±2°C/60% RH±5%) conditions and monitored for changes in key attributes such as hardness, friability, floating behavior, and dissolution [31]. Studies like Mahale et al. showed that optimized dapsone floating tablets retained drug content and floating performance after accelerated and ambient storage, highlighting the importance of polymer choice, protective packaging, and antioxidants to prevent degradation and density changes under humidity and heat [32]. Comprehensive stability evaluation using validated methods is essential to assure quality, safety, and efficacy throughout storage and use.
APPLICATIONS-
Sustained and Controlled Drug Release-
FDDS prolongs gastric residence time, enabling sustained and controlled drug release, improving efficacy, reducing dosing frequency, and enhancing compliance. Hydrophilic gel?forming polymers (HPMC, sodium alginate) regulate diffusion, while gas?generating agents maintain buoyancy for prolonged delivery in the upper GIT, which is ideal for drugs with narrow absorption windows or local gastric action [19]. Examples include famotidine and quetiapine fumarate floating tablets, which maintain steadier plasma levels and better control of acid?related or psychiatric disorders [14,20]. Multiparticulate systems such as floating microspheres/hollow microballoons further reduce the dose?dumping risk and allow fine control of release via matrix composition [33]. FDDS are used for antibiotics, antidiabetics, cardiovascular and GI drugs, often designed using kinetic models to approximate zero?order or near zero?order release [19]
Site?Specific Drug Delivery in the Stomach-
By floating on gastric contents, FDDS retains the dosage form in the stomach and provides localized drug release at the gastric mucosa, maximizing local concentration while limiting systemic exposure [19]. This is particularly useful for antibiotics against *H. pylori*, antacids, and gastroprotective or anticancer agents used for ulcers, gastritis, and gastric tumors [29]. Optimized formulation variables (polymer type, gas?forming level, floating lag time) keep the system in the stomach for the required duration, and imaging techniques such as gamma scintigraphy and MRI have confirmed in vivo gastroretention [36]. Site?specific release can lower required dose, decrease dosing frequency, and protect drugs unstable at intestinal pH, giving more predictable pharmacokinetics [14].
Enhanced Bioavailability of Poorly Absorbed Drugs-
FDDS improves the bioavailability of drugs limited by short residence in the upper GIT by retaining them at their main absorption sites [31]. Drugs such as metformin, riboflavin, and ciprofloxacin, which have narrow absorption windows, benefit from sustained gastric release, leading to higher and more consistent absorption [35]. Floating microspheres and matrix tablets also enhance dissolution of poorly soluble drugs through prolonged gastric contact and swelling matrices [24]. By smoothing plasma profiles and reducing first?pass effects, FDDS can reduce dose fluctuations, dose dumping, and related side effects [20].
Therapeutic Benefits in Special Populations-
In pediatrics, FDDS provides sustained release with fewer doses and can be formulated as small multiparticulate systems that are easier to swallow and allow dose flexibility [36]. In geriatric patients, where gastric motility and pH are altered, FDDS helps maintain steady plasma levels and reduce dose?related adverse effects and pill burden. For chronic diseases such as diabetes, hypertension, and *H. pylori* infection, FDDS enable long?term site?specific therapy with improved efficacy and lower systemic toxicity [20]. Patients with GI disorders or post?surgical changes can also benefit when formulations are tuned to overcome rapid emptying or variable transit, ultimately improving clinical outcomes and quality of life [36].
RECENT ADVANCES & FUTURE PERSPECTIVE -
Novel Polymers and Composite Materials-
Recent FDDS research has emphasized the use of new polymers and composites that improve buoyancy, release control, stability, and biocompatibility [19,20]. Stimuli?responsive (pH/temperature/enzyme?sensitive) polymers enable site?specific, on?demand drug release [29]. Chemically modified chitosan and alginate enhance mucoadhesion, swelling, and encapsulation, thereby strengthening gastroretention and sustaining drug [31]. Composite matrices combining natural and synthetic polymers (e.g., HPMC–Eudragit and HPMC–ethyl cellulose) balance biodegradability with mechanical strength and optimize lag time and kinetics [19,20]. Nanocomposite hydrogels with silica, clays, or nanotubes show superior swelling, strength, and tunable release, whereas biodegradable polyesters such as PLA, PGA, and PLGA provide degradable floating microparticles with controlled release and better compliance [31,36].
Nanotechnology and Smart Floating Systems-
Nanotechnology?based FDDS uses nanosized floating particles to increase the surface area, dissolution, and absorption while maintaining prolonged gastric residence, often with PLGA, chitosan, or other biodegradable carriers [31]. Stimuli?responsive polymers integrated into nano?FDDS create “smart” systems that adjust release according to gastric pH, temperature, or enzymes, improving precision and safety [37]. Ligand?conjugated nanocarriers target gastric receptors for localized therapy in infections and cancers, and multifunctional nanocomposites incorporating magnetic or imaging agents support theranostic use and mucus penetration for better local retention [33,38]
Regulatory Aspects and Commercial Products-
Regulatory approval of FDDS requires compliance with pharmacopeial tests, robust data on bioavailability enhancement, gastric retention (often via imaging), and validated analytical methods [22,25]. Demonstrating predictable in vivo performance is challenging, therefore, advanced imaging and characterization tools are encouraged [16]. Several marketed products, such as Madopar HBS, Valrelease, and Cifran OD, illustrate the successful clinical application of gastroretentive concepts and support further development [14]. Future frameworks are expected to emphasize QbD, strong IVIVC, and clear guidance for nano?FDDS [39].
Challenges and Research Opportunities-
Key challenges include inter?patient variability in gastric retention, difficulties in scaling up multiparticulate and nano?FDDS, and the need to fully assess safety and biocompatibility of novel polymers [36,40]. Establishing reliable IVIVC remains difficult due to complex gastric physiology, while opportunities exist for targeted, multifunctional and theranostic systems, and for patient?centric designs tailored to pediatrics, geriatrics, and GI?disorder populations [33,36]. Emerging directions such as AI?assisted formulation optimization and organ?on?chip models are being explored to accelerate development and de?risk commercialization [20,39]
FACTORS AFFECTING FLOATING DRUG DELIVERY SYSTEMS -
Physiological Factors (Gastric Emptying, pH, Motility)-
The physiological conditions of the GIT strongly influence the performance and gastric retention of FDDS. The gastric emptying rate varies with the fed/fasted state, meal composition, and MMCs; rapid motility can expel floating systems and shorten the residence time [29]. The acidic gastric pH (1–3) affects drug stability and polymer swelling, whereas diseases or pH?modifying drugs may alter buoyancy and release [24]. Motility patterns and gastric volume, influenced by age, disease, and diet, as well as anatomical variations such as pyloric size or gastric morphology, further modify residence time and must be considered in formulation design [40].
Formulation Factors (Polymer Type, Density, Drug Properties) -
Formulation variables determine floatation and release behavior of FDDS. Hydrophilic and hydrophobic polymers, such as HPMC, sodium alginate, carbopol, and Eudragit, control swelling, gel strength, and matrix integrity, thereby modulating floating lag time, duration, and kinetics [19]. The dosage form density must remain below that of gastric fluid (~1.004 g/cm³), which is achieved using low?density polymers, gas?generating agents, or porous structures; excess density causes sinking [24]. Drug solubility, stability in gastric pH, dose, and absorption window guide candidate selection and may require strategies to enhance dissolution without losing buoyancy [29]. The levels and types of effervescent agents (e.g., sodium bicarbonate and citric acid) are adjusted to generate adequate CO? while preserving tablet integrity [40].
Patient?Related Factors-
Patient characteristics also affect FDDS efficacy by altering gastric residence and absorption. Age?related changes, such as slower emptying and reduced acid secretion in the elderly, can extend retention and modify dissolution [36]. The feeding state is critical: fed conditions increase volume, pH, and residence time, whereas fasting MMCs may rapidly clear floating systems[40].Gastrointestinal diseases (e.g., gastroparesis, ulcers), concomitant medications affecting pH or motility, surgical alterations, and individual variability in motility all contribute to variable in vivo performance, highlighting the need for robust and, where possible, patient?tailored formulations [36,40].
CONCLUSION
Gastroretentive floating drug delivery systems (FDDS) successfully address rapid gastric emptying limitations, significantly enhancing bioavailability for drugs with narrow absorption windows. This review confirms the efficacy of both effervescent systems—employing gas-generating agents (sodium bicarbonate, citric acid) alongside swellable polymers (HPMC, sodium alginate)—and non-effervescent approaches utilizing low-density hydrogels and hollow microspheres.Comprehensive evaluation through pre/post-compression parameters, buoyancy lag time measurements, dissolution kinetics analysis (zero-order, Higuchi models), and ICH stability testing validates robust FDDS performance. Therapeutic applications demonstrate sustained release capabilities, site-specific gastric delivery for H. pylori eradication, bioavailability enhancement for metformin and ciprofloxacin, and specialized benefits for pediatric/geriatric populations.Recent innovations in stimuli-responsive polymers, nanocomposite hydrogels, nanotechnology-based carriers, and Quality by Design (QbD) optimization via factorial/DoE methodologies represent transformative advancements. Performance modulation by physiological factors (gastric pH, motility), formulation variables (polymer ratio, density), and patient characteristics underscores the need for tailored approaches.Future research must prioritize AI-driven formulation design, theranostic systems, and patient-centric strategies to achieve superior gastroretention and optimized therapeutic outcomes. FDDS evolution from laboratory innovation to clinical reality exemplifies pharmaceutical science's capacity to overcome physiological barriers through systematic engineering and technological integration.
REFERENCES


Tanmayi Patil, Rajani Shettigar, Swapnil Phalak, Advanced Formulation Paradigms in Gastroretentive Floating Drug Delivery Systems, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 1130-1142. https://doi.org/10.5281/zenodo.18955282
 10.5281/zenodo.18955282
10.5281/zenodo.18955282
