
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Swami Vivekanand College of Pharmacy, Udgir
Adverse drug reactions (ADRs) are an often overlooked but critical aspect of patient care in hospitals. In India, they pose a significant challenge, affecting patient safety, treatment outcomes, and overall healthcare resources. Hospital pharmacists are uniquely positioned to detect, monitor, and prevent ADRs, playing a crucial role in improving medication safety. This review explores how Indian hospitals are implementing ADR monitoring systems, particularly under the framework of the Pharmacovigilance Programme of India (PvPI). Studies from different parts of India highlight common trends: antimicrobials are frequently involved in ADRs, with dermatological and gastrointestinal reactions being most common. Yet, under-reporting remains a major hurdle due to lack of awareness, limited resources, and time constraints among healthcare staff. Hospital pharmacists can make a difference by leading ADR monitoring initiatives, collaborating closely with doctors and nurses, and utilizing tools such as the Naranjo algorithm and WHO-UMC causality assessment. Introducing structured protocols, regular staff training, and digital surveillance systems can further enhance detection and reporting. By combining vigilance with proactive engagement, Indian hospital pharmacies can not only reduce preventable ADRs but also contribute to safer and more effective patient care across the country.
An Adverse Drug Reaction (ADR) is basically any unwanted or harmful reaction that happens when someone takes a medicine at the usual dose. According to the World Health Organization (WHO):
“An ADR is a response to a drug which is noxious and unintended, and which occurs at doses normally used in humans for prevention, diagnosis, treatment, or for modifying a physiological function.” In India, the Central Drugs Standard Control Organization (CDSCO) uses the same definition. Both highlight the importance of recognizing harmful drug effects, even when medicines are used correctly.[3,4]
Monitoring ADRs in hospitals is essential for multiple reasons. First and foremost, it ensures patient safety by detecting harmful reactions early and preventing serious complications or fatalities. It also ensures regulatory compliance, as hospitals are required to report ADRs to authorities like CDSCO, contributing to national pharmacovigilance efforts. Furthermore, ADR monitoring supports quality improvement in healthcare by helping professionals recognize patterns, enhance prescribing practices, and improve overall patient care. Additionally, it serves an educational purpose, training healthcare staff to understand potential drug-related risks. In India, the Pharmacovigilance Programme of India (PVPI) plays a key role in supporting hospitals to monitor ADRs and make medicines safer for the public.[5,6]
Adverse drug reactions (ADRs) are a significant cause of hospital admissions and fatalities worldwide. Globally, studies estimate that around 5% of urgent hospital admissions are caused by ADRs, and in certain countries, up to 12% of these cases can result in in-hospital deaths.[7] In India, the problem is also substantial. Research from a tertiary care hospital in Gujarat reported that 5.42% of hospital admissions in an internal medicine ward were due to ADRs, while another study noted a 1.8% mortality rate among patients experiencing ADRs.[8]
Historical Background of ADR Monitoring in India:
Adverse Drug Reactions (ADRs) have long been a concern in healthcare, and over the years, India has gradually recognized the importance of monitoring drug safety. The first structured attempt in India came in 1986 when the Drug Controller General of India set up 12 regional centres to collect ADR data from hospitals. However, the initiative faced many challenges, including limited trained personnel, lack of proper infrastructure, and low awareness among healthcare professionals. Despite these hurdles, this early effort highlighted the urgent need for a well-organized, national system for monitoring ADRs.
India took a significant step forward in 1997 by joining the World Health Organization’s Programme for International Drug Monitoring. This collaboration helped India connect with global pharmacovigilance efforts and emphasized the value of sharing ADR data internationally. Still, in the early stages, the program struggled due to insufficient infrastructure and coordination issues, showing that India needed a robust and systematic approach to effectively collect, analyse, and act on ADR reports.
To address these gaps, the National Pharmacovigilance Program (NPVP) was launched in 2005 under the Central Drugs Standard Control Organization (CDSCO). The aim was to create a network of ADR monitoring centres across hospitals and medical institutions, standardize reporting practices, and improve drug safety monitoring across the country.
In 2010, the NPVP was reorganized and renamed the Pharmacovigilance Programme of India (PVPI), with the Indian Pharmacopoeia Commission (IPC) serving as the National Coordination Centre. This change allowed for an expanded network of monitoring centres, more streamlined reporting systems, and increased awareness among healthcare professionals. Over time, PVPI has contributed significantly to ADR reporting in India. Yet, underreporting remains an issue. Today, efforts continue to train healthcare workers, raise public awareness, and integrate pharmacovigilance into daily clinical practice, ensuring that medicines remain safe and effective for all. [9,10]
Classification of Adverse Drug Reactions (ADRs) in Hospital Pharmacy:
An Indian Perspective Adverse Drug Reactions (ADRs) are an important concern in hospital settings because they can affect patient safety, treatment outcomes, and healthcare costs. Understanding and properly classifying ADRs is essential for effective pharmacovigilance and improving patient care. In India, hospital pharmacies play a crucial role in identifying, reporting, and managing ADRs to ensure safe medication.
1] Causality Classification: -
Causality assessment helps determine whether a drug is likely responsible for an observed adverse event. In India, two main methods are commonly used: WHO-UMC Causality Scale: This simple and widely used scale classifies ADRs as certain, probable/likely, possible, unlikely, conditional/unclassified, or assessable /unclassifiable. Naranjo Algorithm: A more detailed scoring system that considers factors like timing of drug administration, response to withdrawal, and rechallenge results. Studies in Indian hospitals report that most ADRs are categorized as “probable,” showing a strong link between the drug and the reaction. This classification helps healthcare professionals make informed decisions about drug safety.
2] Severity Classification: -
Severity classification measures how intense an ADR is and the impact it has on the patient’s health. Commonly used scales include Modified Hartwig and Siegel Scale: Grades ADRs from mild to fatal. Modified Schumock and Thornton Scale: Focuses on whether the ADR could have been prevented. In Indian hospital studies, most ADRs are of moderate severity. They often require intervention but rarely cause permanent harm. This type of classification helps prioritize which reactions need urgent attention and which can be monitored over time.
3] Predictability Classification: Types A to F
A widely used method to classify ADRs is based on predictability, known as Type A to F classification:
Type A (Augmented): Predictable and dose-dependent. Usually related to the drug’s known action Example: Hypoglycaemia from insulin, bleeding from warfarin.
Type B (Bizarre): Unpredictable and dose independent. Often immune-mediated or due to genetics. Example: Anaphylaxis from penicillin, Stevens-Johnson syndrome from sulphonamides.
Type C (Chronic): Reactions caused by long-term therapy. Example: Osteoporosis from prolonged corticosteroid use.
Type D (Delayed): Appear after long-term exposure or even after stopping the drug. Example: Thalidomide-induced birth defects, cancer from alkylating agents.
Type E (End-of-use/Withdrawal): Occur when a drug is stopped. Example: Rebound hypertension after stopping clonidine.
Type F (Failure of therapy): Unexpected failure of the drug to produce the desired effect. Example: Antibiotic treatment failure due to resistance.
Indian hospital data show that Type A reactions are most common, while Type B reactions, although rare, tend to be more serious and may require hospitalization.
4] Preventability Classification: -
Preventability helps determine whether an ADR could have been avoided:
Preventable ADRs: Often caused by medication errors, drug interactions, incorrect dosing, or lack of monitoring. Example: Digoxin toxicity due to dosing errors.
Non-preventable ADRs: Cannot be avoided even with proper prescribing and monitoring. Example: Stevens-Johnson syndrome caused by sulphonamides.[11,12]
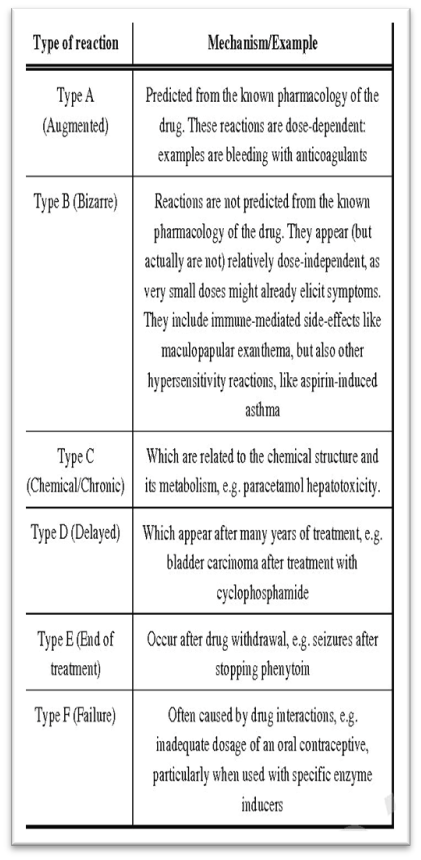
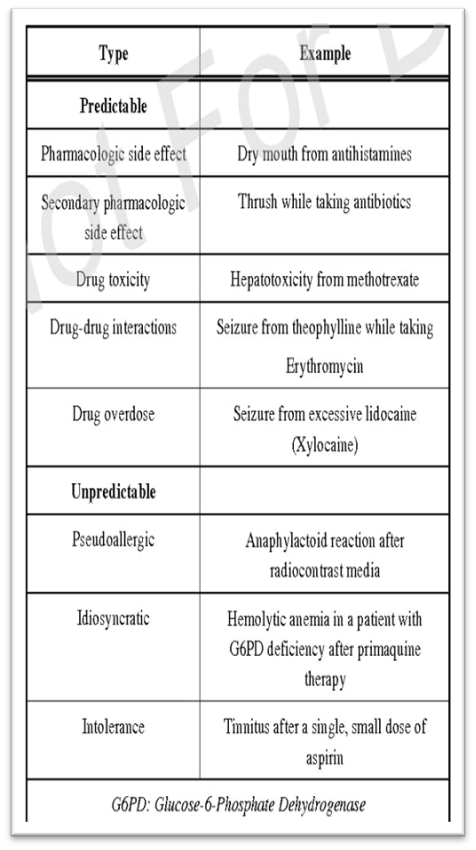
Fig.1, Predictability Classification of ADR Fig.2, Predictable & Unpredictable
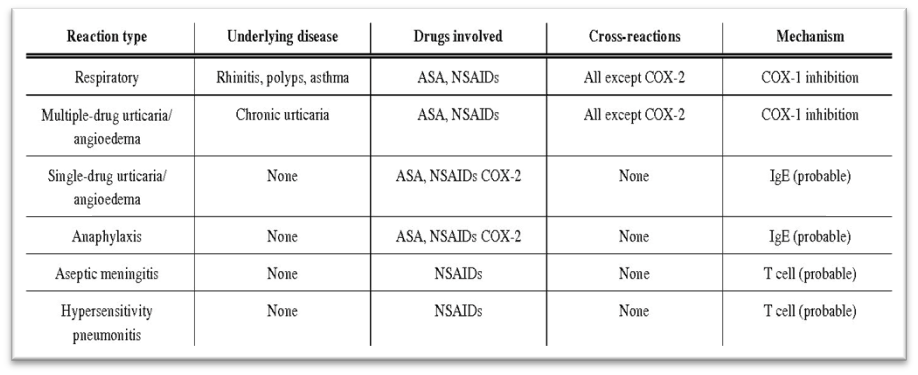
Fig.3 Severity classification of ADR
Importance of ADR Monitoring in Hospitals
1] Protecting Patient Safety:
The main goal of ADR monitoring is to detect harmful drug reactions early and prevent further complications. When healthcare professionals recognize and report ADRs promptly, they can stop or change the drug before it causes serious harm. Hospital-based surveillance in India has shown a reduction in avoidable injuries through active monitoring. [13]
2] Identifying High-Risk Drugs and Patterns:
ADR monitoring helps hospitals recognize which medicines most often cause problems. In India, antibiotics, NSAIDs, and anticancer agents are among the top drugs linked to ADRs. By knowing these trends, hospitals can promote safer prescribing and update treatment guidelines. [14]
3] Supporting National Pharmacovigilance and Policy Decisions:
Hospital data contribute directly to the Pharmacovigilance Programme of India (PVPI), helping authorities identify new safety signals, change drug labels, and issue alerts. This strengthens national drug safety and benefits patients across the country. [15]
4] Reducing Healthcare Costs and Hospital Stay:
ADR monitoring has a strong economic impact. When ADRs are detected early, patients recover faster and require fewer medical interventions. Studies from Indian tertiary hospitals have shown that active ADR reporting reduces unnecessary hospital expenses and bed occupancy rates. [14]
5] Enhancing Rational Use of Medicines:
Monitoring ADRs promotes responsible prescribing. When clinicians understand which medicines cause frequent reactions, they become more cautious with drug choices and dosages. This results in improved therapeutic outcomes and safer use of medicines for all patients. [13]
6] Improving Awareness and Reporting:
Many healthcare professionals do not report ADRs due to lack of awareness or time. Continuous hospital monitoring programs, led by pharmacists and clinicians, encourage better understanding and reporting habits. Such initiatives help feed essential safety data into the national PvPI system. [15]
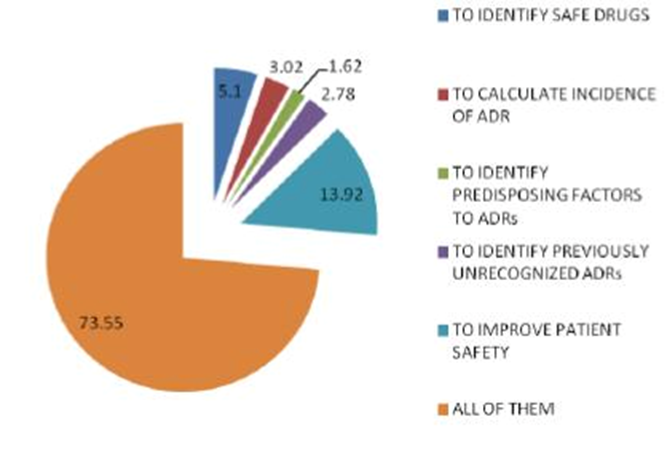
Fig.4 Importance of ADR monitoring
Role of hospital pharmacy in ADR monitoring:
Improving Awareness and Reporting in many healthcare professionals do not report ADRs due to lack of awareness or time. Continuous hospital monitoring programs, led by pharmacists and clinicians, encourage better understanding and reporting habits. Such initiatives help feed essential safety data into the national PvPI system. As seen through various studies and the basic concept of pharmaceutical care, a pharmacist plays a vital role in the identification, detection, Prevention, and management of drug-drug

Fig.5 Role of hospital pharmacist in ADR monitoring
Interactions, drug-food interactions and ADRs. Pharmacist can carry out such activities in inpatient Setting, while taking part in viewing charts during Ward rounds, and during medication management while dealing with prescriptions.
1. Detection and Identification of ADRs:
Pharmacists are often the first to notice unusual drug effects because of their constant interaction with both patients and prescriptions. Their knowledge allows them to identify whether a symptom is due to a disease condition or a side effect of a drug. For example, a pharmacist might identify that a patient’s skin rash is caused by a reaction to an antibiotic rather than an infection. Early detection of ADRs prevents further harm, reduces hospitalization time, and improves treatment outcomes. [18]
2. Reporting and Documentation of ADRs:
Pharmacists play a central role in documenting and reporting ADRs within the hospital and to the Pharmacovigilance Programme of India (PvPI). They ensure that data such as the drug involved, dosage, reaction type, and clinical outcomes are accurately recorded. This data helps identify national trends in drug safety and supports decisions on labelling, withdrawal, or warnings. [16]
3. Education, Training, and Awareness:
One of the most important contributions of hospital pharmacists is in educating healthcare staff about ADRs. Many healthcare professionals underreport ADRs because of limited awareness or uncertainty about what qualifies as a reportable reaction. Pharmacists help overcome this barrier by conducting regular training sessions, workshops, and awareness programs. These sessions guide doctors, nurses, and students on how to identify and report ADRs properly. In India, hospitals that include pharmacists in training activities have shown a notable rise in ADR reporting and overall pharmacovigilance participation. Pharmacists thus serve as effective communicators between departments, ensuring that safety information is shared promptly and efficiently. [16]
4. Promoting Rational Use of Medicines:
Pharmacists play a crucial role in promoting the rational and evidence. Based use of medicines. By reviewing ADR data, they help identify high-risk drugs and unnecessary drug combinations, advising physicians on safer alternatives or dosage adjustments. This process prevents repetitive ADRs and supports more effective therapy. Through hospital drug and therapeutics committees, pharmacists use ADR reports to improve local formulary decisions and treatment guidelines. Their recommendations reduce medication errors and improve patient outcomes. [18]
Methods of ADR detection:
1. Spontaneous Reporting:
Spontaneous reporting is the most widely used method for ADR detection in hospitals and national pharmacovigilance programs. In this approach, healthcare professionals voluntarily report suspected ADRs using standard forms, such as those provided under PvPI. Advantages of this system include its simplicity, low cost, and ability to detect rare and unexpected reactions that may not appear during clinical trials. However, disadvantages include underreporting, incomplete data, and reporting bias, as many cases depend on the motivation and awareness of healthcare workers. Hospital pharmacists help overcome these barriers by conducting regular training sessions and maintaining accessible reporting systems within the pharmacy department. [17]
2. Prescription Event Monitoring (PEM):
Prescription Event Monitoring is a post-marketing surveillance method in which pharmacists and clinicians follow up on patients who have received specific new drugs. They record any medical events occurring during the treatment period, whether or not they are suspected to be drug related. This prospective method helps identify ADR patterns in real world clinical settings and supports regulatory decisions about drug safety. Although PEM is more common in developed countries, it is gaining attention in India as part of hospital pharmacovigilance efforts. It enables long-term observation of a large number of patients, improving the understanding of a drug’s safety profile. [21]
3. Intensive Monitoring of High-Risk Drugs:
This method involves close surveillance of specific high-risk medicines known to cause frequent or severe ADRs. such as anticancer drugs, antibiotics, or antiepileptic. Hospital pharmacists play a key role by reviewing patient medication charts, monitoring vital signs, and assessing clinical laboratory values for early warning indicators. Intensive monitoring is especially useful in tertiary care hospitals where complex therapies are administered. Studies from Indian hospitals have shown that pharmacist led monitoring programs significantly increase the detection rate of ADRs and help initiate preventive measures early.[19]
4. Electronic Health Records (EHRs) and Data Mining:
With the increasing digitization of healthcare systems, electronic health records (EHRs) and data mining have emerged as powerful tools for ADR detection. Pharmacists can use hospital databases to track laboratory abnormalities, medication changes, or clinical keywords linked to ADRs. Automated algorithms can scan vast patient records to identify suspicious patterns. Data mining helps detect trends that might otherwise be missed by manual reporting. According to recent research, integrating based ADR detection with manual pharmacist review greatly enhances accuracy and efficiency. [20]
5. Prospective & Retrospective Approaches:
ADR detection can follow either a prospective or retrospective approach. In prospective monitoring, hospital pharmacists observe patients in real time, identifying ADRs as they occur during hospitalization. This method is resource-intensive but provides timely information that helps prevent escalation of drug reactions. Retrospective monitoring, on the other hand, involves reviewing past medical records or discharge summaries to identify unreported ADRs. While it is less laborious, it may miss early symptoms or incomplete cases. A combination of both methods is often recommended in hospital pharmacovigilance systems to ensure comprehensive ADR detection and analysis. [19]
Strategies to Improve ADR Monitoring in Hospital Pharmacy:
Adverse Drug Reactions (ADRs) are a significant concern in hospital settings, and effective monitoring is essential for patient safety. Hospital pharmacies play a central role in detecting, reporting, and preventing ADRs. Improving ADR monitoring requires systematic strategies that involve healthcare professionals, patients, and technological tools.
1] Develop a strong and reliable system for ADR reporting:
A standardized ADR reporting system within the hospital is crucial. Pharmacists, nurses, and doctors should have clear guidelines on how to report suspected ADRs. Hospitals can implement structured forms and digital reporting tools to make reporting quick and consistent. Encouraging non-punitive reporting increases reporting rates, as healthcare professionals are more likely to report ADRs if they are assured it won’t lead to blame. Example: The Pharmacovigilance Programme of India (PvPI) encourages hospitals to report ADRs to regional centre’s, helping create a national ADR database. [24]
2] Use of Clinical Decision Support Systems (CDSS):
CDSS integrated into hospital pharmacy systems can automatically flag potential ADRs, drug interactions, or high-risk prescriptions. Alerts generated by CDSS help pharmacists intervene before the patient experiences harm. Regularly updating CDSS with Indian specific drug guidelines and interaction data ensures relevance to local practice. [22]
3] Regular Medication Review and Reconciliation:
Pharmacists should perform medication reconciliation at admission, transfer, and discharge. Reviewing all prescribed drugs helps identify duplicate therapies, potentially harmful combinations, or inappropriate doses, which reduces ADR risk. Special focus should be on elderly patients, patients with renal/hepatic impairment, and polypharmacy cases, as they are more prone to ADRs. [21]
4] Training and Awareness for Healthcare Professionals:
Conducting regular training sessions for doctors, nurses, and pharmacists on ADR identification, reporting, and prevention improves vigilance. Workshops can cover topics like recognizing unusual symptoms, understanding high-risk drugs, and using reporting tools effectively. Promoting a culture of safety encourages proactive ADR monitoring. [22]
5] Patient Education and Engagement:
Educating patients about their medications, potential side effects, and the importance of reporting symptoms is critical. Patient counselling by pharmacists at discharge or during hospital stay can improve ADR detection. Providing educational leaflets or using digital apps for monitoring symptoms helps patients participate actively in their own care. [24]
6] Auditing and Feedback:
Regular audits of ADR reports and hospital prescribing patterns help identify trends and high-risk areas. Feedback to healthcare professionals about ADR incidents encourages safer prescribing habits and continuous improvement in monitoring. [21]
7] Implement Pharmacovigilance Programs:
Hospitals should actively participate in national pharmacovigilance programs like PvPI. Centralizing data collection allows hospitals to identify drug safety signals and contribute to national ADR databases. Such programs can also provide training, alerts, and resources for hospital pharmacists to enhance monitoring. [23]
Risk factors for Adverse drug reactions in hospital pharmacy
A] Patient-Related Risk Factors:
1) Age: Age is one of the most recognized determinants of ADRs. Elderly patients often have decreased kidney and liver function, slower metabolism, and altered body composition. These changes lead to drug accumulation and toxicity even at standard doses. Many elderly patients also use multiple medications, which increases the chance of drug–drug interactions. On the other hand, children are vulnerable because their organs and metabolic systems are still developing. Therefore, both age extremes require dose adjustment and closer observation.
2) Gender and Genetics: Women are more likely to develop ADRs due to hormonal fluctuations and differences in fat distribution, which affect how drugs are metabolized. Additionally, genetic variations in liver enzymes such as CYP2D6 or CYP3A4 can cause individuals to metabolize drugs too slowly or too rapidly, altering their therapeutic effects.
3) Lifestyle and Nutrition: Smoking, alcohol intake, and malnutrition also modify drug action. For instance, chronic alcohol use induces liver enzymes, changing how certain drugs like warfarin or phenytoin work. Malnourished patients may have low protein levels, which increases free (active) drug concentration in the blood. [29]
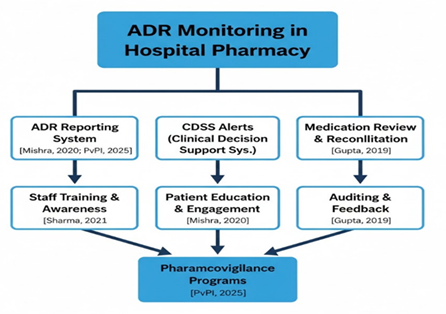
Fig.6 Risk factors for adverse drug reaction
B] Drug-Related Risk Factors:
1) Polypharmacy: Polypharmacy defined as the concurrent use of five or more medications is a leading cause of ADRs in Indian hospitals. It is common in elderly patients or those with chronic diseases such as diabetes, hypertension, and heart failure.
2) Narrow Therapeutic Index (NTI) Drugs: Some drugs, like digoxin, lithium, warfarin, and theophylline, have a narrow therapeutic index, meaning a small increase in dose can shift the drug from effective to toxic. These medications require careful therapeutic drug monitoring (TDM) by pharmacists and physicians.
3) Drug Formulation and Route: The route and formulation can also affect ADR frequency. For instance, intravenous drugs act faster but carry a higher risk of severe hypersensitivity reactions. Poor-quality or counterfeit formulations, occasionally reported in India, can further complicate safety. 4)Duration and Dose: Excessive dose or long-term therapy increases the risk of cumulative toxicity such as aminoglycoside induced nephrotoxicity or NSAID induced gastric ulcers. Hence, dose optimization and regular lab monitoring are crucial. [27]
C] Disease-Related Risk Factors:
The patient’s medical condition can also influence how the body handles drugs. Renal Impairment: Many drugs are excreted through the kidneys. In patients with reduced renal function, drug accumulation can lead to toxicity. For example, aminoglycosides or vancomycin can cause kidney damage if doses are not adjusted. Liver Disease: Impaired metabolism results in longer drug half-lives. Drugs like paracetamol, isoniazid, and valproic acid may cause hepatotoxicity in such cases. Cardiac and Respiratory Diseases: Reduced oxygen flow and altered circulation affect how drugs are distributed, especially sedatives and beta-blockers. Chronic Conditions: Patients with diabetes, cancer, or autoimmune disorders often require multiple long-term therapies, increasing ADR risk. [26]
D] Hospital and System-Related Risk Factors:
Even the hospital environment contributes to ADR risk. In India, pharmacovigilance systems are still developing, and many ADRs go unnoticed due to under-reporting. Overburdened healthcare workers and lack of digital prescription systems. To improve this, hospitals need to strengthen their ADR monitoring cells, encourage a non-punitive reporting culture, and involve pharmacists directly in ward-based care. [25]
Illustrative Case Studies on Adverse Drug Reaction (ADR) Monitoring in Indian Hospital Pharmacy Practice:
Case 1: Antibiotic Induced Hypersensitivity Reaction: A case of antibiotic-induced hypersensitivity was reported in a secondary care hospital in Tamil Nadu, where a 32-year-old female patient developed a severe allergic reaction following the administration of amoxicillin clavulanic acid for lower respiratory tract infection. The reaction was characterized by urticaria, pruritus, and dyspnoea occurring within 15 minutes of intravenous infusion. Immediate discontinuation of the antibiotic and administration of intravenous antihistamines and corticosteroids resulted in full recovery. The causality assessment using the WHO-UMC scale categorized the reaction as “probable.” Upon review, it was found that the patient’s allergy history had not been documented in her medical record. The incident prompted implementation of a pre-administration allergy check protocol by the hospital pharmacist. This observation correlates with findings reported by Arulmani et al. (2007), who conducted a prospective study at a secondary care hospital in South India involving 1,000 inpatients. The study identified antibiotics as the leading cause of ADRs, accounting for 38.8% of the total cases reported, with β-lactam antibiotics being the most common offenders. The authors emphasized the importance of establishing ADR monitoring centres and pharmacist-led pharmacovigilance committees for early identification and management of such reactions. [28]
Case 2: Cisplatin Induced Nephrotoxicity during Chemotherapy: A prospective ADR monitoring study conducted at a tertiary cancer institute in North-East India reported a case of cisplatin-induced nephrotoxicity in a 55-year-old male undergoing chemotherapy for non-small cell lung carcinoma. After administration of cisplatin (75 mg/m²), the patient developed vomiting, fatigue, and elevated serum creatinine levels (1.9 mg/dL) within 48 hours. The ADR was classified as “probable” according to the Naranjo scale. Dose adjustment and enhanced pre and post-hydration therapy were implemented under the supervision of a clinical pharmacist. Subsequent treatment cycles were completed without recurrence of nephrotoxicity. Wahlang et al. (2016) conducted a large prospective study on 256 oncology patients receiving various cytotoxic agents in a tertiary care hospital. Their study reported that 42.2% of patients experienced gastrointestinal ADRs, 18.0% experienced renal toxicity, and 12.5% had haematological toxicity. The study further demonstrated that early detection and pharmacist intervention significantly reduced the severity of ADRs. The authors highlighted the need for inclusion of pharmacists in chemotherapy monitoring protocols to ensure dose optimization and patient safety. [30]
Case 3: Polypharmacy Induced Adverse Reaction in Elderly Patients: A 72-year-old male patient with a history of hypertension, diabetes, and osteoarthritis presented with symptoms of dizziness and confusion after taking multiple concurrent medications. The regimen included amlodipine (5 mg), atenolol (50 mg), metformin (500 mg), glimepiride (1 mg), diclofenac (50 mg), and alprazolam (0.25 mg). Clinical evaluation indicated excessive hypotension and sedation due to the additive effects of calcium channel blockers, β-blockers, and benzodiazepines. The clinical pharmacist identified the drug interaction and coordinated with the medical team to discontinue alprazolam and reduce the amlodipine dosage.
The patient’s symptoms resolved within 48 hours. A similar pattern was reported by Sriram et al. (2011), who conducted a prospective study on 400 hospitalized patients at a tertiary care center in South India. The study found an overall ADR incidence rate of 16.1%, with polypharmacy being the primary risk factor. The majority of ADRs occurred in patients aged 60 years and above. The study recommended routine medication reviews by pharmacists to minimize ADRs arising from multiple drug use and drug–drug interactions. [31]
Case 4: NSAID-Induced Gastrointestinal Bleeding: An illustrative case of NSAID induced gastrointestinal bleeding was recorded in a tertiary care hospital in Delhi. A 60-year-old woman presented with melena and epigastric pain after self-medicating with diclofenac 50 mg twice daily for chronic joint pain over a three-week period. Endoscopic evaluation revealed gastric mucosal erosions and an active bleeding ulcer. The ADR was classified as “probable” on the Naranjo scale. The patient was treated with intravenous proton pump inhibitors and sucralfate suspension, followed by discontinuation of the NSAID. The hospital pharmacist reviewed the medication history and identified the lack of a gastroprotective agent as the primary contributing factor. D’Cruz et al. (2012) conducted a detailed analysis of ADRs among Indian inpatients and reported that non-steroidal anti-inflammatory drugs (NSAIDs) and antibiotics accounted for nearly 54% of ADR-related hospital admissions. Gastrointestinal bleeding was among the most frequent adverse events linked to NSAIDs. The study emphasized that a large proportion of these ADRs were preventable through appropriate patient counselling, rational prescribing, and routine pharmacist supervision. [32]
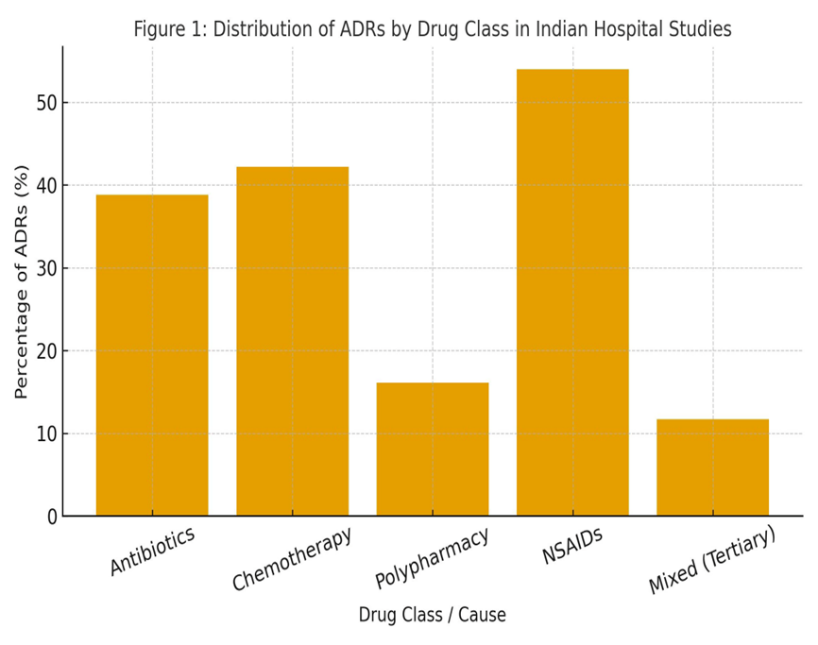
Fig. 7 Distribution of ADRs by drug class in hospital studies
Recent advances in adverse drug reactions monitoring in hospital pharmacy:
1) AI / ML MODELS TO PREDICT ADRs:
Artificial Intelligence (AI) and Machine Learning (ML) technologies are increasingly used to improve ADR prediction and management. These models can analyse large volumes of healthcare data such as electronic health records (EHRs), lab reports, and prescription data to identify high-risk patients. Algorithms such as neural networks, decision trees, and logistic regression can help predict ADRs associated with specific drugs by identifying complex patterns and risk factors. In Indian hospitals, AI and ML applications are still emerging but are expected to significantly transform pharmacovigilance by automating the detection of drug-safety signals. The introduction of AI-based tools into the Pharmacovigilance Programme of India (PvPI) has made digital reporting systems more efficient and accurate.
Hospitals are gradually integrating AI into pharmacy services to reduce human error, enhance drug surveillance, and ensure timely intervention in suspected ADR cases. This technological shift marks a significant step toward predictive pharmacovigilance in Indian healthcare systems. [33]
2) PHARMACOGENOMICS IN ADR MONITORING:
Pharmacogenomics (PGx) focuses on understanding how an individual’s genetic variations influence drug response and toxicity. The use of pharmacogenomic testing in ADR monitoring helps to identify genetic risk factors that may predispose patients to adverse reactions. India’s diverse genetic population offers a unique opportunity to explore gene–drug interactions specific to the Indian context. A study by Sahana et al. (2022) analysed whole-genome sequences of Indian individuals and revealed that most people carry several clinically relevant pharmacogenomic variants. These genetic variations are found in key drug-metabolising enzymes such as CYP2C9, CYP2C19, and immune-related genes such as HLA-B, which are linked with serious ADRs like Stevens Johnson syndrome due to carbamazepine use. The inclusion of pharmacogenomic testing in clinical practice allows healthcare professionals to tailor therapy and reduce preventable ADRs. Although its implementation in India faces challenges such as high testing costs, limited awareness, and infrastructure constraints, pharmacogenomics has the potential to greatly reduce ADR related hospitalisations and improve patient safety in the coming years. [34]
3) ELECTRONIC ADR DASHBOARDS AND REPORTING SYSTEMS:
The integration of electronic ADR reporting dashboards in hospitals has modernised the way ADRs are captured, reviewed, and reported. These digital dashboards consolidate ADR data from multiple departments and present them in an organised and easily accessible format. They allow pharmacists and clinicians to track ADR patterns, identify high-risk medications, and analyse trends across hospital units. The Pharmacovigilance Programme of India (PvPI) has developed several tools, including mobile applications, online portals, and reporting forms, to simplify ADR reporting. such initiatives have improved reporting rates and reduced underreporting by providing simple and accessible reporting platforms. Electronic dashboards not only help in data storage and analysis but also enable early detection of signals that could indicate emerging drug-safety concerns.
The use of these tools makes ADR management more data-driven and efficient, promoting real-time collaboration between pharmacists and physicians for safer prescribing practices.[35] Integration of technology in Indian hospital pharmacy practice Combining AI/ML models, pharmacogenomics, and electronic dashboards represents the next phase of hospital pharmacy advancement in India. AI can predict which patients are at risk of ADRs, pharmacogenomics can explain why these reactions occur, and electronic dashboards can track and manage them efficiently. The coordinated use of these technologies ensures early identification and prevention of ADRs. In Indian hospitals, implementation can begin with pilot programmes focusing on high-risk drugs and genetic testing for select patient groups. The collected data can be used to develop institution specific AI models and contribute to national pharmacovigilance databases. Although challenges such as funding, infrastructure, and workforce training persist, the gradual digital transformation of Indian healthcare makes the integration of these tools both feasible and essential.
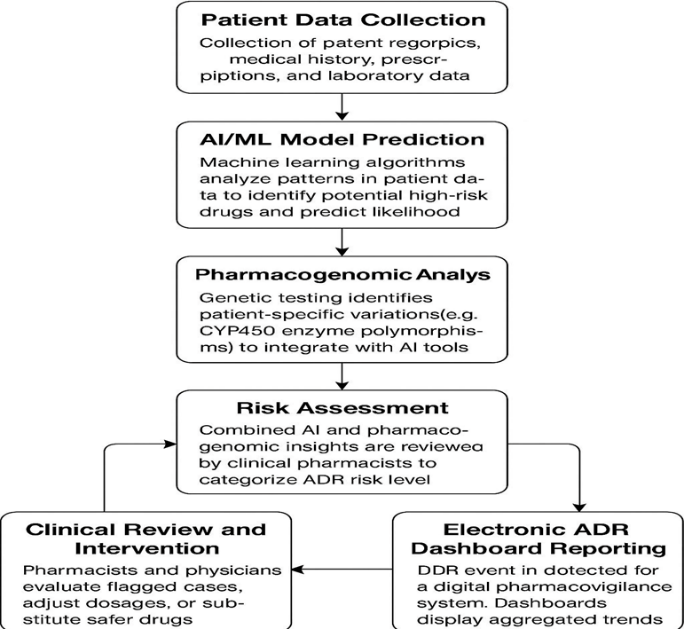
Fig.8 Recent advances of ADR monitoring in hospital pharmacy
Barriers and challenges in ADR monitoring:
Adverse-drug-reaction (ADR) monitoring in India runs on a mix of national coordination and local reporting. The Pharmacovigilance Programme of India (PvPI) is now coordinated through the Indian Pharmacopoeia Commission (IPC) and, as of the Kalaiselvan et al. review, 179 Adverse Drug Reaction Monitoring Centres (AMCs) reported into the National Coordination Centre. India’s contribution to the global safety database was about 3% and the WHO-UMC “completeness score” for Indian Individual Case Safety Reports
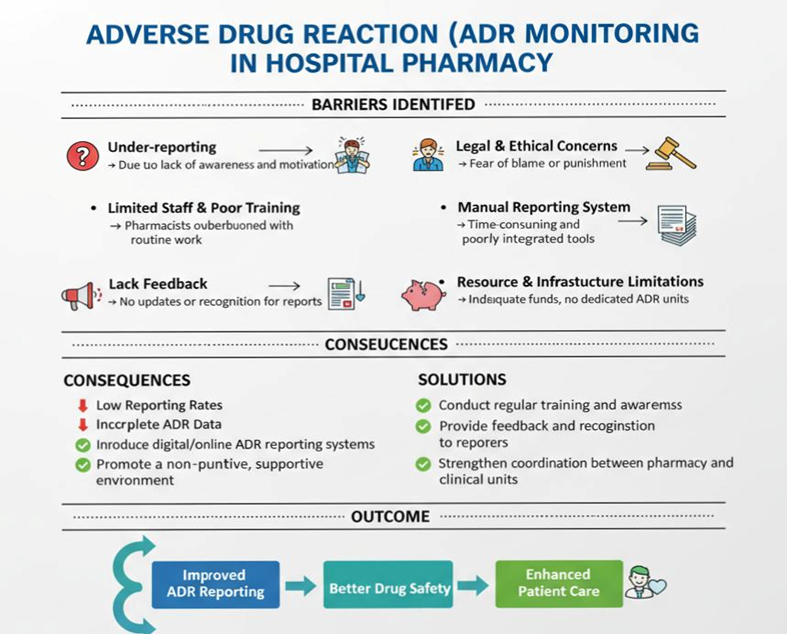
Fig.9 Barriers and challenges in ADR monitoring
(ICSRs) was reported as 0.93/1 A useful indicator that submitted reports are relatively complete. The NCC (IPC) has been working to build capacity, coordinate AMCs, and support regulatory action (for example, safety label changes notified in 2015 for drugs such as carbamazepine and piperacillin tazobactam). These figures show that the structural backbone exists many centres, fairly complete reports but they also imply the system is still growing relative to worldwide reporting and needs broader hospital level engagement to increase reporting volumes.[37] Despite the national framework, many practical barriers remain at the hospital level. The Sahu & Das 2024 review describes how PvPI processes work in practice (AMCs, PV associates, VigiFlow, and consumer reporting routes) and highlights operational bottlenecks that reduce frontline reporting.
The review notes that PvPI uses the WHO-UMC software, Flow to convert submitted ADR forms into ICSRs, which are validated locally at AMCs and then forwarded to NCC and ultimately the Uppsala Monitoring Centre. It also lists consumer/patient reporting options (web forms, the “ADR PvPI” Android app, a toll-free helpline 1800-180-3024, and dedicated email addresses).
These digital routes make reporting easier in principle, but Sahu & Das point out that awareness and training gaps mean many staff and patients still do not use them.
Under-reporting remains a human and system problem. Kalaiselvan et al. emphasise capacity building (workshops, AMC training) and collaboration with national health programmes to increase reporting; yet the PvPI contribution (≈3% of the global database at that time) indicates room to grow. Sahu & Das describe practical reasons for under-reporting encountered across Indian hospitals: lack of awareness about what to report, uncertainty about causality, perceived time burden, and the absence of visible feedback when reports are filed. Together these two reviews make the same point from complementary angles: national infrastructure and software exist, but hospital-level culture, training, and feedback loops must improve for ADR reporting to become routine. Practical weaknesses highlighted in the reviews include workforce and workflow issues. Kalaiselvan et al. report efforts to expand AMC coverage and strengthen central coordination, but they also note the importance of local analytic capacity so AMCs and hospitals can triage reports and act locally (formulary changes, alerts). Sahu & Das list the PvPI operational elements PV associates, coordinator roles at AMCs, monthly reporting to NCC and emphasise that without protected time for pharmacists or dedicated PV staff, ADR monitoring often becomes a low priority in busy wards. In human terms: the system can collect a report, but it needs people with time and training to interpret it and turn it into safer practice. [35,36]
Future Prospects of ADR Monitoring in hospital pharmacy:
Adverse Drug Reaction (ADR) monitoring plays a crucial role in ensuring patient safety, optimizing therapeutic outcomes, and improving rational drug use in hospitals. As the healthcare landscape in India continues to evolve, hospital pharmacies are expected to become the central hubs of pharmacovigilance activities. The future prospects of ADR monitoring are deeply tied to the adoption of digital tools, integration of technology, patient participation, and enhanced training of healthcare professionals. Recent Indian review studies published on PubMed Central (PMC) highlight how these future directions can transform ADR monitoring from a reactive system into a proactive and predictive one.
One of the key areas of development for the future of ADR monitoring in hospitals is digitalization and electronic reporting. According to Suke et al. (2015) in their review “Role of Pharmacovigilance in India: An Overview” published in the Indian Journal of Pharmacology, underreporting of ADRs in India remains a major concern due to lack of awareness, heavy workloads, and manual documentation systems. The authors emphasize that the integration of ADR reporting into electronic medical records (EMR) and hospital information systems could simplify reporting, reduce delays, and allow automatic detection of potential ADRs through data mining algorithms. They also suggest that hospital pharmacists should be trained to use these systems efficiently, making them active participants in data-driven pharmacovigilance. The study concludes that linking the hospital’s pharmacy database to the Pharmacovigilance Programme of India (PvPI) could ensure a faster, standardized, and nationwide ADR monitoring network. [38]
Another emerging direction is the use of hospital-based pharmacovigilance units and active surveillance models. In a review by Ahmad et al. (2016) titled “Pharmacovigilance: An Overview and Its Role in India” published in the International Journal of Pharmaceutical Sciences and Research, the authors explain that hospital pharmacists must take a leading role in detecting, assessing, and documenting ADRs through structured pharmacovigilance units. They propose that future hospital pharmacy departments in India should adopt active surveillance systems, where ADR monitoring is not dependent only on voluntary reporting but also on continuous observation of patient data, prescription audits, and laboratory results. This model can be enhanced by involving clinical pharmacists in ward rounds and drug review committees, where they can identify ADR trends early. The review further suggests that collaboration with national centers such as the Indian Pharmacopoeia Commission (IPC) will strengthen data reliability and national reporting consistency. Such institutionalization of pharmacovigilance practices within hospitals will mark a significant leap in ADR management in India. [39]
The future of ADR monitoring will also rely heavily on advanced technologies such as artificial intelligence (AI), big data analytics, and patient centered reporting systems. Kalaiselvan et al. (2019), in their article “Pharmacovigilance Programme of India: Recent Developments and Future Perspectives” published in the Indian Journal of Pharmacology, highlight how the implementation of intelligent data analysis tools can enhance the detection of ADR signals and predict adverse reactions before they occur. The authors suggest that AI-based algorithms can analyze large volumes of hospital and national pharmacovigilance data to identify hidden trends, drug interactions, or population-specific risks. They also emphasize the importance of empowering patients through mobile ADR reporting apps, awareness campaigns, and hospital-based counselling. The study envisions a future where ADR monitoring becomes an integral, technology-driven part of healthcare, supported by strong collaboration between the IPC, hospital pharmacists, and clinicians across India. [37]
CONCLUSION:
Monitoring of adverse drug reactions is an ongoing, ceaseless, and continuing process. Though pharmacovigilance is still in its infancy in India, this is likely to expand in the times to come. This is because, as the newer and newer drugs hit the market, the need for pharmacovigilance grows more than ever before. Therefore, monitoring of the adverse effects of newer drugs particularly of serious nature is mandatory. Physicians should report death due to drugs, life threatening complications, hospitalisation (initial or prolonged), disability if significant, persistent, or permanent, congenital anomalies, a reaction which requires medical intervention to prevent damage, such as the administration of N-acetylcysteine following acetaminophen overdose. It is important to remember that most adverse drug reactions would subside once the offending agent is discontinued or dosage reduced; however, many result in permanent damage. The need is to spread awareness about using minimal doses of the drugs, at least in the beginning of the treatment. for this, students (both undergraduates and postgraduates) need to be trained in drug safety, and a habit of rational drug use should be inculcated in them from the beginning. Continuing Medical education programmes for physicians and other health professionals should be conducted to make them aware of the methodologies and other technical aspects of the drug Monitoring process. The review discusses different aspects of ADRs, their reporting and monitoring. It examines the reporting of the ADR by a common man to health professionals and by health professionals to higher authorities. Pharmacovigilance, the working programme with respect to ADRs and their function described to understand the established system in India. All the government programs, Committees and systems and systems are discussed for better understanding of ADR monitoring and reporting. A country like India has vast population that demands proper medication use and appropriate drug monitoring system. Drugs can be used in the lengths and breadths of this vast country and ADR monitoring is thus a challenge. Use of different varieties of drugs for different indications in different ethnic groups and age groups add in the complexities of the process. However, in India there is a systematically structured programme on ADR monitoring. The awareness in urban citizens is better than the rural citizens and can always be improved though different awareness programs.
REFERENCES

Mutthe Prashant, Adverse Drug Reaction Monitoring in Indian Hospital Pharmacy: A Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 357-374. https://doi.org/10.5281/zenodo.18470511
 10.5281/zenodo.18470511
10.5281/zenodo.18470511