
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
School of Pharmacy and Emerging Sciences, Baddi University of Emerging Sciences & Technology, Makhnumajra, Distt Solan, Tehsil Baddi, Himachal Pradesh 173205
Hair is a keratinized epithelial structure, provides defense against exposure to sunlight. The anagen, catagen and telogen phases are the successive cycles that the hair growth goes through. An autoimmune disease called alopecia areata occurs when there is early transition of hair growth phase from anagen to the catagen, telogen, and exogen phase and results in hair loss. This review paper includes hair physiology, alopecia areata pathophysiology and herbal plants potential of alopecia areata over allopathic treatment.
Keratinization of germinative cells results in better epithelial structure, which is what is known as hair, that provides the scalp with the best defense against exposure to sunlight [1, 2]. It serves as the body’s protective appendages and is regarded as an integumentary accessory structure, together with sweat and sebaceous glands. Chemical components, including carbon, nitrogen and oxygen, combine with keratin to form hair [3]. Human existence is significantly impacted by hair, which serves as a statement of pride. Having beautiful, healthy hair is crucial to one’s image [2, 15]. Although each person’s hair grows differently, on average, it grows 15-30 mm every month [1].
An autoimmune disease called alopecia areata causes variable hair loss on scalp, face or body, which significantly lowers quality of life [7, 8, 23]. Non-scaring type hair loss is the second most prevalent form [7]. Worldwide, the disease’s lifetime incidence is 2% and its prevalence is 1 in 1000 [16]. In 75% of cases of alopecia areata, the scalp’s bald lesions are concentrated in one or more localized patches. Eye lashes and eyebrows may be affected by more widespread hair loss [17]. Although alopecia areata frequently causes psychological distress, it is not a life-threatening condition [7, 18, 19, 20]. Chronic conditions include lupus erythematosus, vitiligo, autoimmune hemolytic anemia, atopic dermatitis, thallium acetate poisoning, hormonal changes and thyroid illness are frequently linked to alopecia areata [7, 9, 21]. Moreover, ocular and nail disorders may be linked to alopecia areata [22]. Although in alopecia areata the leukocyte-mediated inflammation was discovered almost a hundred years ago, the immune system’s role in the pathophysiology of the condition has only been acknowledged as the main underlying cause since the late 1950s [7,9,24,25].
DIAGNOSIS:
Alopecia areata can influence any skin that bears hair, however, it usually influences the scalp first [9]. A well-defined bald patch free of itching, redness, peeling or scarring is the common clinical investigation of alopecia areata [7, 26]. Eight questions in the Alopecia Areata diagnostic form are used to separate patients with alopecia areata [7]. The instrument’s specificity is 97.8%, and it’s sensitivity is 89.9% [7, 27]. In roughly 10% to 15% of instances, alopecia areata can affect the nails; in certain populations, it can affect up to 44% [9, 28, 29, 30]. If alopecia areata’s clinical manifestation is unclear, a punch biopsy is performed [7].
PATHOPHYSIOLOGY:
The anagen, catagen, telogen phase are the successive cycles that the hair growth goes through [4, 12]. The primary factor influencing hair length is the anagen phase, lasts for two to six years on average. 85% of hair follicles on the scalp are in the anagen phase. When the growing cycle ends and a follicle starts to become dormant, the anagen phase is followed by a brief resting phase known as catagen [4, 5, 13, 14]. The catagen phase lasts 10-14 days. When the hairs enter the telogen phase, they go into a resting state. For 90-100 days, this period lasts [6, 10, 11]. 15% of hair follicles on the scalp are in the telogen phase [5].
The early transition of hair follicles from the anagen phase into the catagen, telogen, and exogen phase results in alopecia areata and causes a decrease in hair growth and a rise in hair fall. It is crucial to remember that the cause of alopecia areata, like any autoimmune disease, is complex [32].
|
Factor |
Explanation |
|
Genetic Factor |
Concerning the hereditary predisposition to alopecia areata; Class II Human Leukocyte Antigen (HLA-D) gene (region on human chromosome 6) [9, 31, 33, 34]. |
|
Concomitant Factors |
Multiple concomitant disorders are linked to alopecia areata, which includes
|
|
Oxidative Stress |
There is higher levels of Superoxide Dismutase (SOD) antioxidant activity in the blood of alopecia areata patient [9, 42]. |
|
Vasculative System |
Generally speaking, inflammation is frequently linked to increased blood flow to the affected areas. Lesions of alopecia areata exhibit elevated temperature, attributed to increased vascularization [9,43]. |
|
Environmental Factors |
Many triggers variables have been suggested to be responsible for the commencement of an alopecia episode. Most often, it is described as either physical or emotional stress [9, 36, 44]. |
Alopecia areata’s precise pathophysiology is not fully known [32]. The collapse of immunological privilege is thought to be the cause of alopecia areata [31, 45]. Our body has immune privilege in a number of cells and organs, including testes, eyes and central nervous system [32]. Hair follicles also possess immune privilege, as evidenced by their immune privilege site and low expression levels of Major Histocompatibility Complex (MHC) [31, 32, 46]. Immune privilege is thought to be associated with low levels of Major Histocompatibility Complex 1 (MHC 1) and MHC 2 expression in hair follicles, results in loss of this immunological privilege. It was discovered that NKG2D, an activating receptor frequently linked to the natural killer (NK) cell lineage, was expressed by CD8+ T cells in close proximity to the hair follicle. In the cell-transfer murine model of AA, it was discovered that this population of CD8+ NKG2D+ T cells was adequate for causing illness. Pro-inflammatory cytokines like IFNg, which are strongly produced by activated CD8+ T cells, tilt the microenvironment of hair follicles in favor of inflammation [80]. Major Histocompatibility Complex expression is stimulated by interferon gamma, which also enables the follicle’s secreted antigen to be delivered to T cells. The antigen hair follicles damaged by interleukin 15 (IL-15), which causes the regulatory T cells to be suppressed and CD8+ T cells to proliferate. This cause the follicles to accelerate into the catagen phase [32].
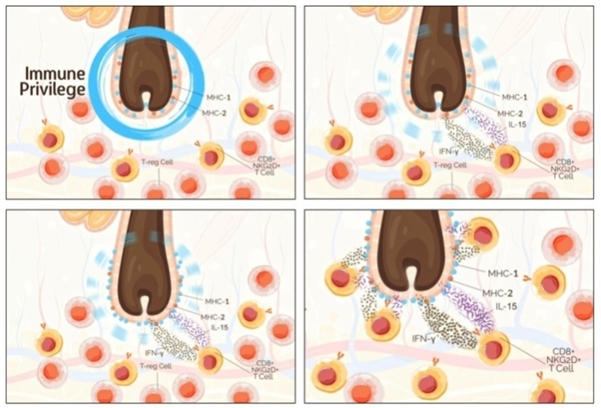
Fig.1. Pathophysiology of Alopecia Areata [32]
MANAGEMENT:
There are various drug therapies to treat alopecia areata. All therapies for alopecia areata focus on reducing hair loss and encouraging re-growth because there is no solution for the underlying issues. Additionally, because alopecia areata progresses in an unpredictable manner, treatment does not ensure regrowth, andrelapse is always possible. 34-50% alopecia patients experience a spontaneous recovery in hair growth within a year [7, 49].
|
Drug |
Mode of Action |
Adverse Effect |
|
Corticosteroids [7,50,51] |
Suppression of the pro-inflammatory cytokines and expression of anti-inflammatory cytokines |
Folliculitis, atrophy, telangiectasia, acneiform eruptions |
|
Minoxidil [5,47] |
Peripheral vasodilator |
Dermatitis or pruritus |
|
Methotrexate [7,52] |
Inhibiting dihydofolate reductase (DHFR) |
Loss of appetite, headache |
|
Sulfasalazine [5,7,47,53] |
Prodrug activated to sulfapyridine and 5-aminosalicylic acid (5-ASA) act on T cells. |
Gastro-intestinal distress, rash, hepatotoxicity, headache |
|
Cyclosporine [5,7] |
Inhibits calcineurine, prevents transcription of cytokines |
High blood pressure, gum overgrowth |
|
Apremilast [5,7] |
Inhibits PDE4, reduce inflammation by increasing cyclic adenosine monophosphate (cAMP) levels |
Weight loss, decreased appetite, insomnia |
|
Anthralin [5,47] |
Antimitotic |
Swollen lymph nodes, skin staining (yellow-brown) |
|
Anti-depressants [48,54-56] |
Stress reduction |
Acneiform eruptions |
|
JAK inhibitor [48,57-60] |
Down regulation of inflammatory cytokines |
Risk of infections |
|
Interlukin-2 (IL-2) [48,61] |
Lowers lesional CD+8 count |
Fatigue, local reaction at injection site |
|
Platelet rich plasma (PRP) [48,62-65] |
Reduce apoptosis of dermal papilla cells |
Swelling, redness at injection sites |
|
Parathyroid hormone- collagen binding domain [48,66] |
Hair cycle stimulator |
Hypercalcemia, localized irritation |
|
Quercetin [48,67] |
Reduction in inflammatory cytokines |
Headache, tingling |
|
Statins [48,68,69] |
Inhibit lymphocyte function |
Headache |
|
Valproic acid [48,70] |
Increase growth singnaling pathways |
Hair loss |
|
finasteride / dutasteride [5] |
5-α -reductase |
erectile dysfunction |
|
Spironolacton [5] |
inhibit production of androgen |
Gynecomastia |
|
Cimetidine [5] |
Anti-androgen |
Gynecomastia |
Alopecia areata can be treated in a no. of ways by various medical systems, such as allopathic, ayurveda or surgery. The majority of people use herbal medicine to prevent or lessen undesirable side effects from allopathic medications. Several herbs are used to stop hair loss and promote hair growth, these are described below [5].
|
Common Name |
Biological Name |
Family |
Parts used |
References |
|
Shoeblack plant |
Hibiscus rosa-sinensis Linn |
Malvaceae |
Leaves & Flower |
(kuldeeep singh, 2016) |
|
Giant Dodder |
Cuscuta reflexa Roxb |
Convolvulaceae |
Stems |
(kuldeeep singh, 2016) |
|
Maek |
Asiasari radix |
Aristolochiaceae |
Roots & Rhizomes |
(kuldeeep singh, 2016) |
|
African basil |
Ocimum gratissum Linn |
Lamiaceae |
Leaves |
(kuldeeep singh, 2016) |
|
Aloe Vera |
Aloe vera L. |
Liliaceae |
Leaves |
(kuldeeep singh, 2016) |
|
Ginkgo |
Ginkgo biloba |
Ginkgoaceae |
Leaves |
(kuldeeep singh, 2016) |
|
Coat button |
Tridax procumbens L. |
Compositae |
Leaves |
(kuldeeep singh, 2016) |
|
Shrubby Sophora |
Sophora flavescens |
Leguminous plants |
Roots |
(kuldeeep singh, 2016) |
|
Bitter Apple |
Citrullus colocynthis Schrad |
Cucurbitaceae |
Fruits |
(kuldeeep singh, 2016) |
|
Indian Spikenard |
Nordostachys jatamansi |
Valerianaceae |
Rhizomes & Roots |
(kuldeeep singh, 2016) |
|
False Daisy |
Eclipta alba L . Hassak |
Asteraceae |
Whole plant |
(kuldeeep singh, 2016) |
|
Shikakai |
Acacia concinna |
Mimosaceae |
Leaves |
(Pushpender kumar jain, 2016) |
|
Neem |
Azadirachta indica |
Meliaceae |
Leaves |
(Pushpender kumar jain, 2016) |
|
Brahmi |
Bacopa monnieri |
Scrophulariaceae |
Leaves |
(Pushpender kumar jain, 2016) |
|
Camphor |
Cinnamomum camphora |
Lauraceae Camphor |
Leaves |
(Pushpender kumar jain, 2016) |
|
Cinnamon |
Cinnamomum zeylanicum |
Lauraceae |
Bark |
(Pushpender kumar jain, 2016) |
|
Lemon |
Citrus limon |
Rutaceae |
Fruits |
(Pushpender kumar jain, 2016) |
|
Amla |
Emblica officinalis |
Euphorbiaceae |
Fruits |
(Pushpender kumar jain, 2016) |
|
Eucalyptus |
Eucalyptus sp. |
Myrtaceae |
Bark |
(Pushpender kumar jain, 2016) |
|
Alfalfa |
Medicago sativa |
Fabaceae |
Leaves |
(Pushpender kumar jain, 2016) |
|
Indian olive |
Olea europaea |
Oleaceae |
Fruits |
(Pushpender kumar jain, 2016) |
|
Avocado |
Persea americana |
Lauraceae |
Fruits |
(Pushpender kumar jain, 2016) |
|
Sandalwood |
Santalum album |
Santalaceae |
Bark |
(Pushpender kumar jain, 2016) |
|
Ritha |
Sapindus mukorossi |
Sapindaceae |
Dried fruit |
(Pushpender kumar jain, 2016) |
|
Bhringraj |
Tridax procumbens |
Asteraceae |
Leaves |
(Pushpender kumar jain, 2016) |
|
Greater Burdock |
Arctium lappa L. |
Asteraceae |
leaves and root |
(Skowronska W., 2021) |
|
Indian pennywort |
Centella asiatica L. |
Apiaceae |
leaves |
(Saansoomchai P., 2018) |
|
Indian Mulberry |
Morinda citrifolia |
Rubiaceae |
fruits |
(Susanti L, 2022) |
|
Muskrat root |
Acorus calamus |
Acoraceae |
roots |
(Park Sang Oh , 2015) |
|
Shell Ginger |
Alpinia zerumbet |
Zingiberaceaea |
leaves |
(Taira N., 2017) |
|
Japanese flowering cherry |
Cerasus serrulata |
|
flower |
(Zhang B., 2023) |
|
Fragrant glory bower |
Clerodendrum fragrans |
Lamiaceae |
leaves |
(Anggraini I., 2019)
|
|
Indian coral tree |
Erythrina variegata |
Fabaceae |
leaves |
(Mustarichie R., 2017) |
|
Guava |
Psidium guajava L. |
Myrtaceae |
Leaves |
(Ruksiriwanich W., 2022) |
DISCUSSION:
Human existence is significantly impacted by hair, which serves as a statement of pride. Alopecia areata, an autoimmune condition causes patchy hair loss. Non-scarring type hair loss is the second most prevalent form. The early transition of hair growth phase from anagen into the catagen, telogen, and exogen phases results in alopecia areata. Although its pathophysiology is not fully known. The collapse of immunological privilege is thought to be the cause of alopecia areata. Alopecia areata can be treated with the allopathic method but to prevent undesirable side effects, several herbal plants are used. This article has covered hair cycle physiology, alopecia areata’s pathology, and herbal plants potential over allopathic treatment.
REFERENCES


Savita Verma, Anupama Kumari, Shaistah Zahrah Maqbool, Anjali Chauhan, Muskan, Abhay Sharma, Alopecia Areata: Pathophysiology, Current Treatments, and The Emerging Role of Herbal Remedies, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 681-690. https://doi.org/10.5281/zenodo.18185816
 10.5281/zenodo.18185816
10.5281/zenodo.18185816