Konkan Gyanpeeth Rahul Dharkar College of Pharmacy and Research Institute, Karjat, Maharashtra, India.
Buccal mucoadhesive drug delivery systems offer a promising alternative to conventional oral and parenteral routes by enabling drug absorption directly through the buccal mucosa. This route bypasses first-pass hepatic metabolism and gastrointestinal degradation, thereby improving bioavailability and ensuring a rapid onset or sustained release of action. The buccal mucosa’s rich vascular supply, ease of access, and relatively stable surface make it an attractive site for local and systemic drug delivery. Formulations such as mucoadhesive tablets, films, patches, gels, and nanoparticles rely on polymers that ensure prolonged adhesion, optimal drug release, and patient comfort. The choice of polymer, mucoadhesive strength, drug solubility, and formulation design significantly influence therapeutic performance. This approach is particularly advantageous for drugs with poor oral bioavailability, short half-lives, or susceptibility to enzymatic degradation. It finds application in delivering analgesics, cardiovascular drugs, hormones, and emerging biologics. Although challenges like salivary washout and limited absorption area exist, innovative polymer blends and permeation enhancers are addressing these issues. Overall, buccal mucoadhesive systems represent a patient-friendly, non-invasive, and efficient platform for achieving enhanced therapeutic outcomes.
Mucoadhesive drug delivery has emerged as a versatile and efficient approach in modern pharmaceutics, offering multiple therapeutic advantages over conventional dosage forms. Among its key benefits are the ability to circumvent first-pass hepatic metabolism, thereby improving systemic drug availability; ease and convenience of administration without the need for invasive procedures; enhanced drug permeation across the mucosal barrier; and protection of sensitive drug molecules from degradation by salivary or gastrointestinal enzymes. Moreover, by reducing fluctuations in plasma concentration, this approach can minimize dose-related adverse effects and improve patient compliance. [1] These systems are designed to adhere to the oral mucosal surface, enabling both local and systemic drug delivery. The buccal, sublingual, and gingival routes are particularly suited for sustained- or extended-release dosage forms, which can prolong therapeutic action while reducing the frequency of dosing. As a result, they have found wide application in improving the pharmacokinetic and pharmacodynamic profiles of various drugs. [2]
In recent years, the pharmaceutical industry has shown increasing interest in the development of oral mucoadhesive formulations. Currently, marketed products in this category include a range of dosage forms such as gels, sprays, tablets, ointments, creams, lozenges, and medicated chewing gums. A survey of scientific literature and patent databases reveals a substantial number of clinical trials and granted patents involving oral mucoadhesive systems, underscoring their potential as a platform for delivering diverse therapeutic agents directly to the oral mucosal surface. [3] The scope of this delivery route is rapidly expanding beyond small-molecule drugs. Researchers are now exploring its use for the administration of complex biotherapeutics, including proteins, peptides, and nucleic acids. Polymeric systems carrying antimicrobial peptides (AMPs) have shown significant promise for treating challenging and resistant infections such as bloodstream infections, which are often difficult to manage with conventional antibiotics. [4] A broad spectrum of natural, semi-synthetic, and synthetic polymers has been investigated for the oral delivery of biologics, with results ranging from moderate to highly successful. The rapid rise of biological and biosimilar pharmaceuticals in the global market has intensified the need for innovative drug delivery solutions that can improve their stability, absorption, and overall pharmacokinetic profile. [5]
From a pharmacokinetic perspective, drugs delivered via the oral mucosa are typically absorbed rapidly through the epithelial tissue, entering the systemic circulation while avoiding gastrointestinal degradation and hepatic first-pass elimination. This route can provide higher bioavailability and controlled drug release, as well as favorable alterations in pharmacokinetic parameters such as maximum plasma concentration (Cmax), area under the curve (AUC), and time to reach maximum concentration (Tmax). [6] For instance, Garhy et al. reported the development of a buccoadhesive gel incorporating carvedilol nanoparticles, which significantly enhanced drug solubility and absorption. Their study demonstrated a twofold increase in bioavailability compared to conventional formulations, attributed to improved dissolution and the bypassing of first-pass metabolism. [7] Despite substantial advances in mucoadhesive drug delivery technology over the past two decades, the fundamental mechanisms underlying mucoadhesion remain incompletely understood. Moreover, most research studies tend to evaluate qualitative and quantitative aspects of mucoadhesion separately rather than through integrated methodologies, limiting a holistic understanding of the process. [8] This review aims to provide a comprehensive overview of the field, with a focus on mucoadhesive polymers, various oral mucoadhesive dosage forms, therapeutic implications, key patents, current trends in clinical trials, and marketed products. By summarizing recent advancements and identifying existing challenges, this work aims to contribute to the future development of more effective and patient-friendly oral mucoadhesive drug delivery systems. [9]
Structural and Functional Characteristics of the Buccal Mucosa
The buccal mucosal lining consists of both keratinized and non-keratinized epithelial regions (Figure 1). The keratinized epithelium is predominantly composed of non-polar lipid components such as ceramides and acylceramides, which render it largely resistant to water penetration. This characteristic makes it more favorable for localized therapeutic applications within the buccal cavity. In contrast, the non-keratinized epithelium contains a higher proportion of polar lipids, including cholesterol sulfate and glucosylceramides, resulting in greater permeability compared to the keratinized type. Consequently, it is well-suited for both systemic drug administration and localized treatment within the buccal region. [10] The buccal cavity serves as an effective route for drug delivery, largely due to the presence of salivary mucins and their inherent negative charge. Within the mucosal secretions, mucins form a protective coating over the buccal surface and can bind with positively charged drug molecules, enabling targeted interaction with specific tissues and facilitating efficient drug delivery. This property makes mucins valuable in the design and evaluation of mucoadhesive systems. Understanding how different polymers interact at the mucin–polymer interface provides insights into the mechanisms underlying mucoadhesion. The adhesive strength primarily arises from the formation of molecular bridges between mucin chains and the polymers. Furthermore, the electronic characteristics of mucin contribute significantly to this adhesion process. Therefore, mucoadhesion results from a combination of mucin’s electrical properties and the intermolecular bonding established between mucin and polymer molecules. [11]
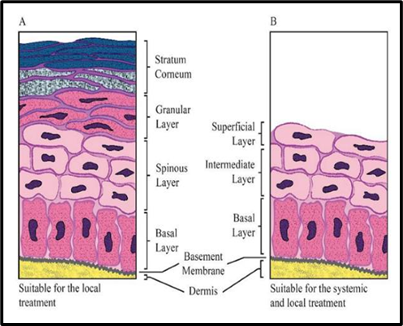
Figure 1. (A) The oral keratinized epithelium (B) non-keratinized epithelium
There are differences in permeability, blood flow, and residence time in various areas of the oral mucosa based on multiple tissue properties. [12] The oral mucosa can be classified into three main routes for drug administration:
Mucoadhesion Theories
Mucoadhesion is a multifaceted phenomenon, and several theories have been proposed to elucidate its underlying mechanisms. These include the mechanical interlocking theory, electrostatic interaction theory, diffusion theory, polymer–mucin interpenetration concept, adsorption theory, and the fracture theory describing bond failure at the interface.
Wetting Theory
This concept proposes that mucoadhesion occurs when a mucoadhesive polymer spreads across and penetrates the microscopic irregularities of the mucosal surface, eventually solidifying to form an adhesive bond. The degree of affinity between the polymer and the surface can be assessed by determining the contact angle. [14]
Absorption Theory
According to this model, adhesion results from chemical interactions between the adhesive polymer and the mucus layer. These interactions primarily involve hydrogen bonding and Van der Waals forces. After the initial contact, the bond strength is derived from the intermolecular forces acting between atoms on the two surfaces. [15]
Electronic Theory
This theory attributes mucoadhesion to differences in the electronic structures of the interacting surfaces. Electron transfer between the polymer and mucosal membrane leads to the formation of an electronic double layer, generating attractive forces that promote adhesion. [16]
Fracture theory
The mechanical evaluation of mucoadhesion generally relies on measuring the force required to detach two surfaces after an adhesive bond has been established. This force, denoted as Sm, is commonly determined in rupture-resistance experiments as the ratio between the maximum detachment force (Fm) and the total contact area (A?) involved in adhesion, expressed as:
Sm = Fm / A?
This approach is particularly applicable for assessing rigid or semi-rigid bioadhesive materials whose polymer chains are unable to significantly penetrate the mucus layer. [17]
Diffusion Theory
This theory suggests that mucoadhesion occurs through mutual interpenetration of the polymer chains and the glycoprotein network of mucus, driven by a concentration gradient. Effective adhesion is achieved when the interpenetration layer reaches a thickness of approximately 0.2–0.5 µm. Factors influencing this process include the molecular weight, mobility, flexibility, and chain length of the polymer, as well as its hydrodynamic size and concentration gradient. [18]
Mechanism of Mucoadhesion
The process of mucoadhesion generally occurs in two sequential stages:
Two main theories describe the events occurring during the consolidation stage:
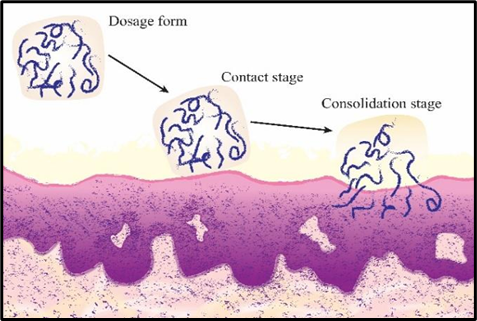
Figure 2: Steps involved in mucoadhesion
Factors Affecting Buccal Mucoadhesive Drug Delivery Systems
A. Polymer-related factors
1. Hydrophilicity: Mucoadhesive polymers possess a variety of hydrophilic functional groups, notably hydroxyl and carboxyl moieties that enhance their ability to form hydrogen bonds with the target surface. In aqueous environments, these groups facilitate polymer swelling, thereby exposing a greater number of potential binding sites. As the polymer network hydrates, the increased distance between chains improves their flexibility, enabling more effective penetration and interaction with the substrate. [21]
2. Molecular Weight: Polymers possessing a molecular weight exceeding 100,000 generally exhibit enhanced mucoadhesive strength. In the case of polyoxyethylene-based polymers, this adhesive capability shows a direct correlation with molecular weight, typically falling within the range of 200,000 to 7,000,000. [22]
3. Flexibility of Polymer Chains: The initiation of mucoadhesion involves the spreading of polymer chains across the interfacial region. For effective entanglement with the mucus layer, these chains must exhibit sufficient flexibility. Incorporation of polyethylene glycol enhances the structural flexibility of polymers, thereby facilitating deeper chain interpenetration. The viscosity and diffusion coefficient of a polymer directly affect its mobility and flexibility, with greater flexibility enabling more efficient penetration and distribution within the mucus network. [23]
4. Cross-Link Density and Swelling: The key structural parameters of a polymer network include pore size, degree of cross-linking, and the average molecular weight between cross-links. According to Flory’s findings, there is an inverse relationship between the extent of swelling and the cross-link density of a polymer. Higher cross-linking restricts water diffusion into the network, thereby reducing swelling capacity and consequently lowering the rate of interpenetration with the mucus layer. [24]
B. Environmental Factors
1. pH: The pH at the polymer–mucosal interface, along with the pH of saliva, which serves as the dissolution medium, significantly affects the performance of mucoadhesive polymers. Salivary pH typically falls within the range of 6.5 to 7.5, varying with flow rate and testing conditions. This microenvironmental pH can alter the ionization state of functional groups in the polymer, thereby influencing its adhesive strength and overall mucoadhesive behavior. [25]
2. Strength: To use a solid bioadhesive system, a particular strength is necessary.
3. Initial contact time: Increased mucoadhesive strength causes longer initial contact times. [26]
C. Physiological variables
1. Mucin turnover: Mucin turnover is important for two reasons. The mucoadhesive's residence time on mucus layers is anticipated to be short due to mucin turnover. Mucin turnover produces a high amount of soluble mucin molecules. [27]
2. Diseased states: Mucus features can vary across a variety of disorders, including common colds, gastric ulcers, ulcerative colitis, cystic fibrosis, female reproductive system infections, and eye inflammation. [28]
Classification of Polymers based on generation
First Generation of Mucoadhesive Polymers
These polymers, whether of natural or synthetic origin, are predominantly hydrophilic and contain organic functional groups such as carboxyl, hydroxyl, or amino groups, which facilitate hydrogen bonding. Common examples include carbomers, various cellulose derivatives, chitosan, and alginates. They are generally categorized into three types:
Carbopol
Carbopol, a lightly cross-linked polyacrylic acid (PAA), is widely recognized as a benchmark material for mucoadhesive polymers. It is favored in pharmaceutical formulations due to its advantages, including prolonged drug release, safety and efficacy in oral administration, enhanced bioavailability, and the ability to protect proteins and peptides from degradation. Its protective role is largely attributed to its ability to alter the rate of degradation reactions. With a pKa of approximately 6.05, carbopol can influence enzymatic activity.[30] For example, in one study, a sublingual buprenorphine tablet was prepared containing Carbopol 974, lactose, and PEG 3350. This formulation demonstrated an optimal sustained-release profile, with complete drug release occurring within 2 hours. Moreover, research has shown that oral insulin absorption can be significantly improved using thiolated polyacrylic acid (thiomer)–cysteine derivatives. [31] These derivatives not only enhance mucoadhesion and protect against enzymatic breakdown but also swell in aqueous environments, thereby increasing the viscosity of the surrounding medium. This higher viscosity can limit enzyme access to the substrate, ultimately reducing degradation. [32]
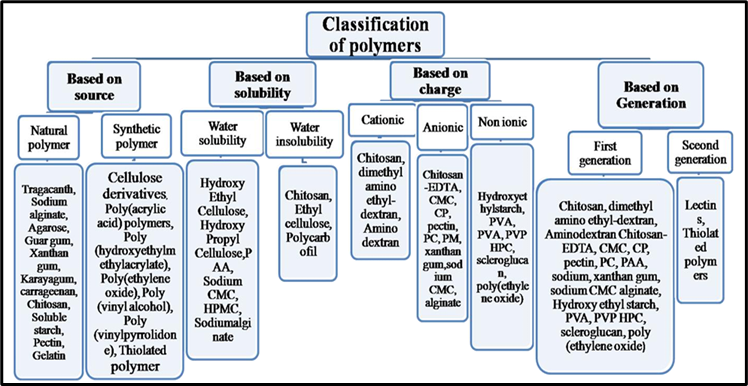
Figure 3. Classification of mucoadhesive polymers based on source, solubility, charge, and generation
Chitosan
Chitosan, a cationic polysaccharide, has become a key material in the design of mucoadhesive drug delivery systems owing to its excellent biocompatibility, biodegradability, and non-toxic nature. Its mucoadhesive properties arise from ionic interactions between its amino groups and the sialic acid residues present in mucin. Onishi and Machida reported that chitosan and its metabolic by-products are rapidly cleared from the body via renal excretion. [33] Ayensu et al. developed lyophilized chitosan wafers incorporating chitosan, bovine serum albumin (as a model protein), glycerol (as a plasticizer), and d-mannitol (as a cryoprotectant). Their findings demonstrated the potential of such wafers for buccal delivery of protein-based therapeutics. In another investigation, low molecular weight chitosan was optimized for gene delivery applications. [34] Additionally, AMP-loaded liposomes coated with chitosan were found to enhance bioavailability and improve oral efficacy. Li et al. encapsulated the antimicrobial peptide KSL (KKVVFWVKFK-CONH?) into PLGA/chitosan composite microspheres for targeted delivery against Fusobacterium nucleatum, achieving sustained antimicrobial and inhibitory activity for up to 80 days. Similarly, Sharma et al. encapsulated the peptide pep-H into chitosan nanoparticles, producing a cationic surface charge that resulted in an 80% reduction in intracellular Mycobacterium tuberculosis load. [35]
Pectin
Pectin is a naturally occurring polysaccharide composed primarily of D-galacturonic acid units linked through glycosidic bonds. Due to its excellent biocompatibility and distinctive physicochemical characteristics, pectin has been widely explored for controlled drug delivery applications. Its strong adhesion to mucosal surfaces enhances the retention time of bioactive agents such as antimicrobial peptides (AMPs). [36] In a study by Krivorotova et al., nisin-loaded pectin nanoparticles (NPs) demonstrated significant antimicrobial activity in vitro against two Gram-negative bacteria (Escherichia coli and Klebsiella spp.) and two Gram-positive strains (Arthrobacter sp. and Bacillus subtilis) using an agar-diffusion assay. The results revealed that the nanoparticles were more effective against Gram-positive bacteria compared to Gram-negative species. [37] Moreover, the antimicrobial effect of nisin-loaded pectin NPs was approximately 100 times greater than that of sodium benzoate, a commonly used preservative, against both Gram-positive and Gram-negative organisms. These findings suggest that pectin-based nanoparticles represent a promising polymeric carrier for antimicrobial drug delivery systems. [38]
Second Generation of Mucoadhesive Polymers
This generation possesses the ability to bind directly to cell surfaces via specific receptor recognition or through covalent linkages, thereby enhancing the strength and specificity of chemical interactions. Notable examples in this category include lectins and thiomers.
Lectins
Lectins are non-immunological proteins or glycoproteins capable of selectively recognizing and binding to specific sugar residues present in glycosylated membrane components. These sugars are typically found in the glycolipids and glycoproteins of mammalian mucosa, either on the epithelial cell surface or within the mucous layer. [39]Upon binding, lectins may remain attached to the cell surface or be internalized through endocytosis. Certain plant-derived lectins, such as those obtained from Ulex europaeus, soybean, peanut, and Lens culinaris, exhibit a strong affinity for mucosal cells, while wheat germ agglutinin is noted for its comparatively low immunogenicity. [40] Their ability to resist acidic and enzymatic degradation makes lectins a promising carrier system for oral drug delivery. [41]
Thiolated Polymers
Thiolated polymers, commonly referred to as thiomers, are modified forms of hydrophilic polymers such as polyacrylates, chitosan, or deacetylated gellan gum. Their unique feature lies in the ability to form covalent bonds with cysteine residues present in mucus, thereby prolonging residence time while enhancing structural rigidity and cross-linking capacity. These polymers also exhibit notable permeation-enhancing effects and possess enzyme-inhibitory activity. [42] In research conducted by Langoth and colleagues, matrix-based tablets incorporating the novel pentapeptide leu-enkephalin (a pain-modulating agent) and the thiolated polymer polycarbophil (PCP) demonstrated improved stability and mucoadhesive performance, with the adhesion effect persisting for over 24 hours. [43]
Miscellaneous Mucoadhesive Polymers
Acrylates
Mucoadhesive polymers such as hydroxypropyl cellulose (HPC), chitosan, and derivatives of poly(acrylic acid) (PAA) are widely utilized across various pharmaceutical formulations. Among these, PAA is regarded as one of the most effective mucoadhesive agents, largely due to its high aqueous solubility, which makes it an excellent carrier for sustained drug release. The strong hydrogen bonding capacity of PAA enables robust complexation with polyvinylpyrrolidone (PVP), a feature that can be exploited in the fabrication of mucoadhesive microspheres. When the water-soluble polymers PVP and PAA come into contact, they form a stable complex that subsequently precipitates, allowing for controlled formulation development. [44]
Hyaluronic Acid
Hyaluronic acid (HA) is an anionic polymer naturally distributed throughout epithelial, connective, and neural tissues. Its molecular weight can vary widely, ranging from approximately 5,000 to 20,000,000 Da. HA is a key constituent of synovial fluid, where it plays a crucial role in maintaining viscosity. Interestingly, a reduction in its molecular weight has been associated with enhanced mucoadhesive performance, making it a valuable candidate in targeted drug delivery applications. [45]
Gellan Gum
Water-soluble polymers capable of forming gels at the site of administration have gained considerable attention for drug delivery applications. These materials offer advantages over other polymers, as their liquid form can be applied directly to the target site, where subsequent swelling produces a robust gel, thereby prolonging residence time. Gellan gum is a microbial polysaccharide synthesized by the water-soluble bacterium Sphingomonas elodea. Alternative gums, such as xanthan gum and karaya gum, have also been explored for their potential in controlled drug delivery systems. [46]
Alginate
Alginate is an anionic mucoadhesive polymer that forms strong hydrogen bonds with mucin glycoproteins through interactions between its carboxyl and hydroxyl groups. This linear, water-soluble polysaccharide has attracted considerable interest for its versatility in pharmaceutical and biotechnological applications. Thiolated sodium alginate derivatives have been used to produce mucoadhesive microbeads for localized drug delivery in periodontal pockets. These formulations demonstrated prolonged drug release after application, highlighting their potential in the effective management of periodontal diseases. [47]
Poloxamers
Poloxamers are widely utilized in the pharmaceutical industry due to their high viscosity, compatibility with a broad range of drugs and excipients, and suitability for developing controlled-release delivery systems. Their thermoreversible gel-forming capability makes them particularly valuable in mucoadhesive formulations, enabling drug administration through multiple routes while ensuring prolonged retention at the application site. [48]
Starch
Owing to their hydrophilicity and biocompatibility, polysaccharides such as starch, alginate, chitosan, and various cellulose derivatives are widely applied in mucoadhesive drug delivery systems. Starch (amylum) is a polysaccharide composed of numerous glucose units linked via glycosidic bonds. Its strong moisture-absorbing capacity enables the formation of a mucoadhesive gel-like matrix. [49] This hydration process can dehydrate the mucosal membrane, facilitating drug transport through paracellular tight junctions. Studies have shown that spray-dried starch and Carbopol 974P exhibit superior mucoadhesive performance compared to equivalent physical mixtures, without irritating, supporting starch’s safety and suitability as a bioadhesive carrier. [50] Furthermore, in combination with polymers such as Carbopol 974P and hydroxypropyl methylcellulose (HPMC), starch-based matrices have demonstrated enhanced drug release, as observed in formulations containing propranolol hydrochloride. [51]
Polyethylene Glycol
Polyethylene glycol (PEG) is a well-recognized mucoadhesive polymer that is safe, non-immunogenic, non-antigenic, and FDA-approved for pharmaceutical applications. Its high water solubility and rapid in vivo clearance are influenced by its molecular weight. [52]PEG’s mucoadhesive behavior is primarily attributed to its ability to form hydrogen bonds with sugar residues present on glycosylated proteins. Studies have also reported that incorporating linear PEG chains into hydrogel matrices enhances adhesion to mucosal surfaces. This improvement is linked to chain interpenetration at the mucus hydrogel interface, resulting in stronger and more stable attachment. [53]
Sulfated Polysaccharides
Sulfated derivatives of polysaccharides have attracted significant attention over the past decade due to their notable chemical and biological properties. Extensive research has explored their anticoagulant, antioxidant, and antithrombotic activities. [54] Sulfation generally enhances water solubility and induces conformational changes in the polymer chain, which can alter and improve biological functionality. [55] Studies have also evaluated the combined effects of sulfated polysaccharides with cyclophosphamide, while sulfated forms of chitosan and chitin have demonstrated potential as effective carriers for delivering various therapeutic agents across mucosal membranes. [56]
Carrageenan
Carrageenan is a gel-forming polysaccharide extracted from red seaweed and is often used as a plant-based alternative to gelatin, making it suitable for vegan and vegetarian applications. Traditionally, it has been utilized in medicine for purposes such as protection against herpes simplex virus, as a personal lubricant, and in the management of HIV. It has also shown antiviral activity against the common cold. An increase in sulfated ester content lowers the solubility temperature of carrageenan and results in weaker gel formation. In the pharmaceutical sector, carrageenan is incorporated into various formulations as a mucoadhesive excipient.[57]
Gelatin
Gelatin is a polyelectrolyte whose net charge depends on both the pH and the type of gelatin used. Type A gelatin is derived from collagen via acidic hydrolysis and has an isoelectric point between 7 and 9, whereas type B gelatin is obtained through alkaline hydrolysis with an isoelectric point ranging from 4.7 to 5.3. Studies have shown that aminated gelatin microspheres exhibit greater gastric mucoadhesion compared to unmodified gelatin microspheres. This enhanced adhesion is attributed to the increased number of amino groups, which confer greater chain flexibility. [58]
Buccal Mucoadhesive Dosage Forms
Solid Dosage Forms
Tablets
The most commonly employed polymers for formulating mucoadhesive tablets include Carbopol (such as CP934, CP940, and PCP), sodium carboxymethyl cellulose (SCMC), pectin, chitosan, hydroxypropyl methylcellulose (HPMC), and carboxymethyl cellulose (CMC). These materials can be utilized individually or in combination to prepare compressed bioadhesive dosage forms. HPMC and pectin generally exhibit weaker bioadhesive strength, whereas SCMC and chitosan demonstrate stronger adhesion. Among the available options, polyacrylic acid derivatives (CP934, CP940, and PCP) display the highest mucoadhesive capacity and the longest residence time. In one formulation study, an optimized combination of mucoadhesive excipients comprising 5% CP934, 65% HPMC, and spray-dried lactose achieved effective bioadhesion with a residence time of approximately 2 hours. Another investigation developed a tablet containing CP and CMC in proportions of 35% and 15%, respectively, resulting in desirable mucoadhesive performance and controlled drug release. An alternative design is the bilayer mucoadhesive tablet, consisting of a drug reservoir layer combined with an adhesive backing layer, further protected by an inert ethylcellulose coating. This configuration offers distinct advantages over single-layer tablets by improving retention, targeted drug delivery, and drug release control. [59]
Bioadhesive Lozenges
Bioadhesive lozenges represent an alternative dosage form with significant potential for sustained drug release and improved patient compliance. They are particularly suitable for individuals who experience difficulty swallowing conventional tablets or capsules. While traditionally employed for systemic drug delivery, lozenges are often formulated to provide localized therapeutic action within the oral cavity or throat. Common applications include the delivery of antibiotics, local anesthetics, antimicrobials, and antifungal agents for the treatment or prevention of oral and pharyngeal conditions. [60]
Polymeric Micelles
Polymeric micelles (PMs) are nanoscale carriers particularly suited for the delivery of poorly water-soluble drugs, including those administered via the oral route. Their ability to provide controlled drug release and enhanced stability contributes to improved oral bioavailability. Specific functional attributes such as pH sensitivity and mucoadhesive behavior have attracted considerable attention, offering a promising strategy for optimizing oral drug delivery. Bernkop-Schnürch and co-workers demonstrated that thiolation of conventional PMs significantly increases mucoadhesive capacity, thereby enhancing the intestinal absorption of therapeutic proteins. Similarly, Kumar et al. reported that PM-based formulations of docetaxel exhibited superior pharmacokinetic performance compared to conventional docetaxel suspensions. [61]
Bioadhesive Micro/Nano Particles
Bioadhesive micro and nanoparticles offer several advantages, including small particle size, high patient acceptability, and the ability to establish close contact with mucosal surfaces. Their reduced size minimizes local irritation and discomfort within the oral cavity. These systems can be formulated as aqueous suspensions, gels, ointments, or pastes. Commonly used polymers for preparing bioadhesive microparticles include Carbopol, polycarbophil, chitosan, alginate, and Gantrez, a copolymer composed of alternating methyl vinyl ether and maleic anhydride units. Studies have shown that chitosan- and gantrez-based particles exhibit prolonged retention on mucosal tissues. [62] Oral transmucosal nanoparticles are suitable for systemic therapy due to their capacity to penetrate the epithelial barrier. In one study, Monti et al. developed a poloxamer 407-based microsphere formulation of atenolol and tested it in rabbits against a marketed tablet. Results demonstrated that the microsphere formulation maintained higher plasma atenolol levels than the commercial product, with comparable bioavailability despite a lower dose, suggesting potential for dose reduction via transmucosal administration. [63] Furthermore, nanoparticle systems allow for modulation of antimicrobial peptide (AMP) release rates by altering delivery system composition, such as the polymer’s molecular weight. Encapsulation of AMPs in solid lipid nanoparticles can enhance their stability for oral delivery. Biocompatible and biodegradable polymers, copolymers, and lipids have also been employed in designing micro- and nanoparticle-based vaccine delivery systems. [64]
Bioadhesive Wafers
Bioadhesive wafers are structured dosage forms composed of a bulk layer and an adhesive surface layer designed to anchor to mucosal tissues. They typically incorporate an antibacterial agent along with matrix-forming and biodegradable polymers. Such systems have been explored for localized drug delivery, with one notable example being a novel periodontal formulation developed for the targeted treatment of periodontitis. [65]
Powder dosage forms
Powder-based drug formulations consist of a physical blend of the active pharmaceutical ingredient and a bioadhesive polymer, designed to be applied directly often by spraying onto the buccal mucosa for the treatment of oral disorders. In a study by Yamamoto et al., a powder containing hydroxypropyl cellulose and beclomethasone dipropionate was administered to the buccal cavity of rats. The formulation prolonged mucosal residence time to approximately 4 hours and demonstrated greater therapeutic effectiveness compared to oral solutions containing the same drug–polymer combination at identical concentrations. [66]
Semisolid Dosage Forms
Bioadhesive Patches/ Films
Buccal patches are of two main types of patches employed for drug delivery via the oral mucosa:
In one study, a buccal patch containing acyclovir, polyethylene glycol (PEG), acrylic acid copolymer, monomethyl ether, and monomethacrylate with an impermeable backing layer demonstrated a sustained drug release for approximately 22 hours in vivo, suggesting its potential for effective buccal delivery. Rana et al. developed a nanoparticle-in-microparticle structured buccal patch as a novel approach for delivering drugs with significant first-pass metabolism. [67]
Buccal films offer greater flexibility, mechanical strength, and ease of removal compared to other dosage forms, making them suitable for controlled release applications. Commonly used polymers include sodium carboxymethyl cellulose (CMC), carbopol 934P, hydroxypropyl methylcellulose (HPMC), and PEG 400. HPMC-based buccal films have been shown to possess superior elasticity, bioadhesion, and swelling tolerance compared to sodium CMC films. [68]
Gels and hydrogels
Gels and hydrogels are semi-solid mucoadhesive systems commonly applied to the buccal mucosa or directly into periodontal pockets to prolong residence time and enhance drug absorption. Gels provide the advantage of forming intimate contact with the mucosal surface, enabling localized and rapid drug release at the application site, making them particularly suitable for oral cavity drug delivery. Carbomers are frequently incorporated into gel formulations to improve mucoadhesion, thereby extending the duration of action. Compared to liquid solutions, gels offer longer drug release profiles and improved bioavailability. An example is Corsodyl®, a mucoadhesive oral gel containing chlorhexidine gluconate as the active agent, which is applied to teeth to prevent plaque buildup and promote oral hygiene. Its formulation also includes hydroxypropyl cellulose (HPC), which helps retain the gel within the oral cavity. [69]
Liquid dosage forms
Mucoadhesive liquid formulations, such as solutions and suspensions, are utilized for local drug delivery within the oral cavity. Among polymer-based solutions, chitosan, carbopol, methylcellulose, sodium carboxymethylcellulose (CMC), gelatin, and polycarbophil demonstrate the highest mucoadhesive potential. Viscous liquids can be formulated with these polymers to serve as protective coatings or as vehicles for delivering therapeutic agents to mucosal surfaces. Artificial saliva preparations are an example of such dosage forms, designed to alleviate xerostomia by adhering to mucosal tissues and providing prolonged lubrication. These formulations often incorporate Sodium CMC to enhance retention time and maintain moisture on the mucosal surface. [70]
Recent Patents, Clinical Trials, And Commercial Products
The effectiveness of mucoadhesion for controlled drug release has been evaluated in numerous formulations through both in vitro and in vivo studies. In recent years, several patents for oral mucoadhesive delivery systems have emerged in the pharmaceutical sector. Most clinical trial formulations are conventional dosage forms, particularly tablets, films, and oral liquids. Tables 1 and 2 summarize recent patents, ongoing clinical trials, and marketed oral mucoadhesive products. [71]
Table 1. Patented buccal mucoadhesive formulations.
|
Active Ingredient |
Patent Number |
Dosage form |
Route of administration |
Year |
|
Apomorphine Hydrochloride |
US10888499 |
Film |
Sublingual |
2021 |
|
Buprenorphine Hydrochloride |
US10874661 |
Tablet |
Sublingual |
2020 |
|
Asenapine maleate |
A205960 |
Tablet |
Sublingual |
2020 |
|
Sufentanil citrate |
N209128 |
Tablet |
Sublingual |
2018 |
|
Desmopressin acetate |
N022517 |
Tablet |
Sublingual |
2018 |
|
Extracts of the Marzeh Khuzestani |
96840 |
Gel |
Buccal |
2018 |
|
Nicotine |
US20060198873A1 |
Film |
Buccal |
2017 |
|
Zolpidem tartrate |
A201509 |
Tablet |
Sublingual |
2016 |
|
Naloxane |
US 10617686B2 |
Liquid spray |
Buccal |
2014 |
|
Bupernorphine |
US201140378497A1 |
Film |
Buccal |
2014 |
|
Acyclovir |
N203791 |
Tablet |
Buccal |
2013 |
|
Fentanyl |
N202788 |
Spray |
Sublingual |
2012 |
|
Miconazole |
022404 |
Tablet |
Buccal |
2010 |
|
Buprenorphine Hydrochloride |
N207932 |
Film |
Buccal |
2015 |
Table 2. Commercial and clinical trial of buccal mucoadhesive tablets
|
Active Ingredient |
Dosage form |
Status |
|
Desmopressin |
Buccal Tablet |
Commercial |
|
Nicotine |
Buccal Tablet |
Commercial |
|
Fentanyl |
Buccal Tablet |
Commercial |
|
Glyceryltrinitrate |
Buccal Tablet |
Commercial |
|
Lorazepam |
Buccal Tablet |
Commercial |
|
Lobeline |
Buccal Tablet |
Phase I/I |
|
Riluzole |
Buccal Tablet |
Phase I/II/III |
|
Alprazolam |
Buccal Tablet |
Phase I/II/III completed |
|
Misoprostol |
Buccal Tablet |
Phase III/IV |
|
Zolmitriptan |
Buccal Tablet |
Phase IV |
Therapeutic approaches for buccal mucoadhesive drug delivery systems
Oral mucoadhesive drug delivery is employed in the treatment of various diseases (Figure 4), offering controlled drug release, enhanced bioavailability, convenient administration, and reduced dosage and dosing frequency.
Antiemetics
Ondansetron hydrochloride, a 5-HT? serotonin receptor antagonist, is commonly prescribed to prevent nausea and vomiting associated with emetogenic cancer chemotherapy. To bypass hepatic first-pass metabolism and enhance drug bioavailability, administration via the buccal route is preferred. [72,73] Ali et al. developed a buccal adhesive tablet containing ondansetron, CP 934, sodium alginate (ALG), sodium carboxymethylcellulose (SCMC, low viscosity), HPMC 15 cps, and ethyl cellulose. Their findings demonstrated that both the drug and the delivery system remained stable in natural human saliva for up to 6 hours. [74] In another study, Koland et al. prepared a fast-dissolving sublingual film incorporating ondansetron, polyvinyl alcohol (PVA), polyvinylpyrrolidone (PVP), and carbopol. Results showed that carbopol-containing films exhibited the highest swelling capacity compared to PVP-based films. Bhalekar et al. formulated buccal bioadhesive hydrophilic matrix tablets using domperidone, HPMC, and carbopol. [75]Their work revealed that increasing the concentration of these polymers enhanced mucoadhesive strength but simultaneously slowed the drug release rate. [76]
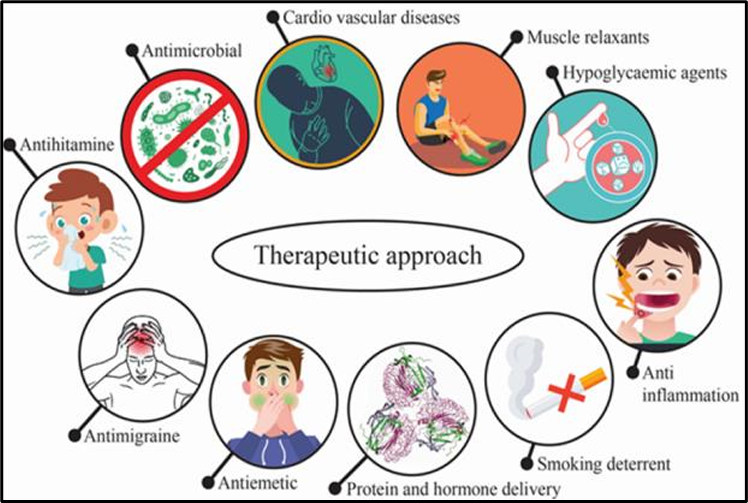
Figure 4. Therapeutic approaches to buccal mucoadhesive drug delivery systems in common diseases.
Antimigraine
Sumatriptan succinate, a 5-HT? receptor agonist, is widely used for the management of migraine attacks. Shidhaye et al. formulated mucoadhesive bilayer buccal patches containing sumatriptan succinate, chitosan, and PVP K30. Their results indicated that increasing the proportion of chitosan enhanced mucoadhesive strength, whereas increasing PVP K30 while reducing chitosan content improved drug release. Interestingly, simultaneously increasing both chitosan and PVP K30 led to a greater swelling capacity of the patches. Due to sumatriptan succinate’s inherently low permeability through the buccal mucosa, the study also investigated the use of penetration enhancers, including polysorbate 80, Transcutol, and dimethyl sulfoxide (DMSO). Findings demonstrated that the combination of these enhancers with buccal administration significantly improved drug permeation while avoiding hepatic first-pass metabolism, making it a promising delivery approach. [77]
Cardiovascular Medicines
Carvedilol, a non-selective β-adrenergic receptor antagonist, is commonly prescribed for the management of hypertension and stable angina pectoris. Yamsani and colleagues developed mucoadhesive carvedilol tablets containing Carbopol 934 in combination with hydroxypropyl methylcellulose (HPMC K4M and K15M) to achieve controlled, zero-order release. Their findings indicated that a higher polymer concentration resulted in a more sustained drug release profile. [78] Similarly, lercanidipine hydrochloride (LER), a calcium channel blocker used for hypertension, was formulated into buccal mucoadhesive controlled-release tablets by Charde et al. The formulations incorporated polyethylene oxide and various viscosity grades of HPMC, either alone or in combination. In vivo experiments in rabbits demonstrated a notable enhancement in LER bioavailability compared to conventional oral dosing. Placebo studies in human volunteers showed that the tablets maintained firm adhesion to the buccal mucosa for over 4 hours without causing irritation or discomfort. [79]
Smoking Deterrents
The addictive nature of smoking is largely attributed to the presence of nicotine (NCT), a psychoactive compound. Nicotine can be delivered via the skin or mucosal membranes, including nasal and buccal routes, due to its ability to permeate membranes in both neutral and protonated forms. [80] Pongjanyakul et al. developed sodium alginate–magnesium aluminum silicate (SA–MAS) buccal films loaded with NCT as a potential smoking cessation aid. These films demonstrated high nicotine loading capacity, a slower release rate, and strong bioadhesive properties, enabling prolonged adhesion to mucosal surfaces. [81] The findings suggested their strong potential as a buccal drug delivery platform. [82] In another investigation, Rao et al. formulated a tri-layered buccal mucoadhesive patch in which a medicated dry tablet was combined with a mucoadhesive film, ensuring stable placement within the oral cavity. [83] Similarly, a bilayer patch containing NCT was designed using xanthan gum as the bioadhesive polymer. This system provided biphasic release, with an initial rapid dose followed by controlled release over 10 hours. [84] The authors concluded that such patches could be promising nicotine replacement therapies, warranting further in vivo evaluation. [85]
Proteins and Hormones
Buccal mucosal delivery offers a convenient and potentially safer alternative for the administration of proteins and peptide-based hormones compared to other routes. [86] In a study by Cui et al., bilaminated insulin films were developed and tested in healthy rats via the buccal route. [87] The films produced a notable hypoglycemic effect and achieved a 17% increase in bioavailability compared to subcutaneous insulin injections. Colonna et al. prepared mucoadhesive films incorporating 5-methylpyrrolidinone chitosan (MPC) and myoglobin (MHb). MPC, a chitosan derivative with favorable mucoadhesive characteristics, proved to be an excellent polymer for bioadhesive film formulation. [88] Nakane et al. designed buccoadhesive tablets containing luteinizing hormone-releasing hormone (LHRH). In vivo studies in beagle dogs showed that plasma LHRH levels reached a plateau within 30 minutes and were sustained for 2 hours, in contrast to the rapid elimination seen after intravenous administration. [89] Giovino et al. developed chitosan-based mucoadhesive films loaded with insulin encapsulated in polyethylene glycol methyl ether-block-polylactide (PEG-b-PLA) nanoparticles. These formulations demonstrated a biphasic sustained release profile, delivering protein steadily over five weeks. [90]
Anti-Inflammatory Drugs
Inflammation is a major contributing factor to various oral cavity disorders. [91] Topical administration of anti-inflammatory drugs such as flurbiprofen, flufenamic acid, and ibuprofen offers the advantage of reduced dosage requirements and minimized systemic side effects. [92,93] In a study by Ghorbani et al., zinc-containing mucoadhesive tablets were prepared using Carbopol 940, sodium alginate, zinc sulfate, and starch. Clinical and statistical evaluations demonstrated that these tablets were effective in reducing pain, decreasing wound diameter, and shortening the recovery period in patients with recurrent aphthous stomatitis compared to the control group. [94] Perioli et al. developed bilayered sustained-release mucoadhesive tablets combining mucoadhesive polymers with an inorganic hydrotalcite matrix for buccal delivery of flurbiprofen. The formulation provided sustained release over 12 hours, enabling a reduction in daily dosage (40 mg vs. 70 mg) while maintaining therapeutic effect.[91] Mura et al. prepared mucoadhesive films containing flufenamic acid complexed with hydroxypropyl β-cyclodextrin (HPβCD) to enhance solubility and dissolution. The complexed drug achieved complete release within 4–5 hours, which aligns with the optimal time window for buccal drug delivery. [95] Additionally, Milani et al. demonstrated that HPβCD exhibits versatile functionality in protein formulation stabilization across a wide concentration range. [96]
Antimicrobials
Conventional dosage forms such as suspensions, solutions, and mouthwashes are often ineffective for oral cavity diseases due to their rapid clearance from the site of application. To overcome this limitation, various mucoadhesive formulations have been investigated for prolonged retention and enhanced therapeutic action. Juan et al. developed a bilayered mucoadhesive tablet containing nystatin, with a lactose layer and a polymeric layer for sustained drug release. The polymeric component enabled a controlled release profile lasting approximately 6 hours. [97] Fini et al. formulated a mucoadhesive gel of chlorhexidine using hydroxypropyl methylcellulose (HPMC), carboxymethyl cellulose (CMC), and hydroxypropyl cellulose (HPC) to improve local antimicrobial activity. [98] In another study, Domb et al. prepared mucoadhesive tablets comprising iodine complexes with ethylcellulose (EC) and HPC for the treatment of oral infections. [99] Obaidat et al. designed mucoadhesive patches containing carvacrol and tetracycline hydrochloride for mouth infection therapy. The formulation exhibited potent activity against Pseudomonas aeruginosa, demonstrating a synergistic effect between carvacrol and tetracycline, as neither compound alone was effective against this strain. The combination also showed antimicrobial activity against Bacillus cereus. [100]
Hypoglycaemic Agents
Mucoadhesive buccal delivery systems have been explored for the administration of hypoglycaemic agents to improve therapeutic efficacy and patient compliance. Semalty et al. developed mucoadhesive buccal films containing glipizide, formulated with hydroxypropyl methylcellulose (HPMC), Carbopol 934 (CP-934), sodium carboxymethyl cellulose (SCMC), and Eudragit RL-100. The study demonstrated that buccal administration could maintain therapeutic plasma levels of glipizide effectively. [101] Muzib et al. investigated mucoadhesive buccal films of glibenclamide prepared using various HPMC grades. The findings revealed that matrix integrity was influenced by both the quantity and physicochemical properties of the polymer. A higher content of hydroxyl groups in HPMC K15 enhanced swelling but reduced residence time. Drug release kinetics were found to be dependent on the polymer composition, with low concentrations of HPMC 3000 being particularly suitable for achieving controlled buccal delivery of glibenclamide. [102]
CONCLUSION
Buccal mucoadhesive drug delivery systems represent a promising and patient-friendly platform for both local and systemic therapy. By enabling direct drug absorption through the buccal mucosa, these systems effectively bypass first-pass metabolism, protect labile drugs from enzymatic degradation, and enhance bioavailability. Advances in polymer science, nanotechnology, and formulation design have facilitated the development of dosage forms with improved adhesion, controlled or zero-order release profiles, and enhanced therapeutic efficacy. The versatility of buccal systems has been demonstrated across a wide spectrum of therapeutic categories, including cardiovascular drugs, hormones, proteins, anti-inflammatory agents, antimicrobials, and hypoglycaemic drugs.
However, despite significant progress, certain challenges remain, such as limited drug permeability for large biomolecules, patient acceptability of dosage forms, and the need for long-term stability under varying physiological conditions. Future research should focus on innovative polymer combinations, permeation enhancers, and nanocarrier-based delivery to address these limitations and achieve more predictable, sustained, and targeted drug release. With continuous advancements, buccal mucoadhesive delivery is poised to evolve into a robust alternative to conventional oral and parenteral routes, offering enhanced therapeutic outcomes and improved patient compliance.
REFERENCES

Ayush Ghosalkar, Dr. Rajani Shettigar, Swapnil Phalak, Buccal Mucoadhesive Drug Delivery Systems: An Innovative Approach for Enhanced Therapeutic Outcomes, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 2243-2265. https://doi.org/10.5281/zenodo.16919099
 10.5281/zenodo.16919099
10.5281/zenodo.16919099
