
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Sharda School Of Pharmacy Gandhinagar, Gujarat, India.
Background: Alzheimer’s disease (AD) is a progressive neurodegenerative disorder and the leading cause of dementia worldwide. It is characterized by cognitive decline, memory impairment, and behavioral changes, significantly impacting patients’ quality of life. As the Global population ages, AD has become a significant public health concern. Objective: This poster provides a comprehensive overview of AD, focusing on its etiology, pathological hallmarks, risk factors, current treatment strategies, and recent advancements in Disease-modifying therapies. Methods: A review of scientific literature was conducted to evaluate the underlying mechanisms of AD, including amyloid-beta (A?) plaque deposition, tau protein hyperphosphorylation, oxidative stress, and neuroinflammation. Genetic predisposition (e.g., APOE ?4 allele), lifestyle factors, and comorbid conditions were analyzed. Furthermore, available pharmacological and Non-pharmacological treatment approaches were reviewed. Results: AD progresses through distinct stages, from mild cognitive impairment (MCI) to severe dementia, with key pathological features including synaptic dysfunction and neuronal loss. While current treatments, such as cholinesterase inhibitors and NMDA receptor antagonists, provide symptomatic relief, they do not halt disease progression. Recent research on monoclonal antibodies targeting A? (e.g., aducanumab, lecanemab) and tau-based therapies offers potential disease-modifying effects. Advances in biomarker-based diagnostics, such as cerebrospinal fluid (CSF) and PET imaging, are improving early detection. Conclusion: Alzheimer’s disease remains a complex neurodegenerative disorder with no definitive cure. Continued research on early detection, precision medicine, and novel therapeutic Strategies is essential to mitigate disease burden and improve patient outcomes. A deeper Understanding of AD pathophysiology may pave the way for innovative interventions and Preventive measures.
Alzheimer’s disease (AD) is the most common cause of dementia, accounting for nearly two-thirds of all cases worldwide (Mayeux& Stern, 2012). First described over a century ago by Alois Alzheimer in 1906, the condition is now recognized as one of the greatest medical and social challenges of the modern era (Cipriani et al., 2011). With the continuous rise in life expectancy, the prevalence of AD is expected to grow dramatically, making it not only a neurological disorder but also a global public health priority.[1,2]
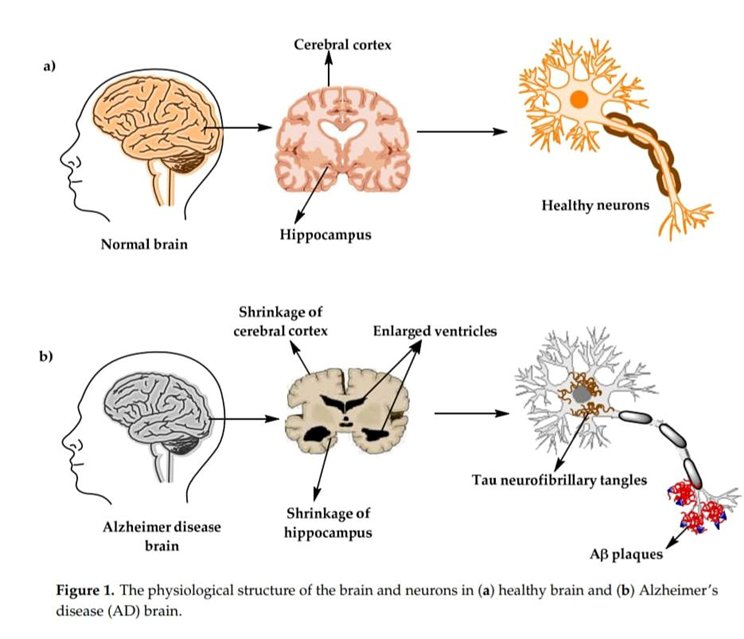
The disease Is clinically characterized by a gradual decline in memory, reasoning, language, and daily functioning, often accompanied by changes in mood and behavior (McKhann et al., 1984). Neuropathologically, AD is defined by the abnormal deposition of amyloid-beta (Aβ) plaques and tau neurofibrillary tangles, which disrupt neuronal communication and trigger widespread synaptic and neuronal loss (Serrano-Pozo et al., 2011; Brion, 1998). These biological alterations translate into progressive cortical atrophy, most prominently affecting the hippocampus and other memory-related regions of the brain.[3]
Beyond the clinical and pathological hallmarks, Alzheimer’s has profound social, emotional, and economic consequences. It affects not only patients but also families and caregivers who face the burden of long-term care and psychological distress (Livingston et al., 2020). Despite decades of research, there is currently no curative therapy. Available treatments mainly target symptoms and provide only modest benefits, underscoring the urgent need for disease-modifying strategies (Yiannopoulou&Papageorgiou, 2020).[4,5,6]
In light of these challenges, continuous research is directed toward unraveling the complex pathophysiology of AD, identifying risk factors, and developing innovative therapeutic approaches (Breijyeh&Karaman, 2020; Zhang et al., 2024).[7]
This review aims to provide an in-depth understanding of Alzheimer’s disease by examining its pathophysiology, exploring key risk factors, and highlighting promising new approaches that are shaping the future of AD treatment and management.
Alzheimer’s disease (AD) is increasingly recognized as a multifaceted disorder with complex biological, social, and clinical implications. Despite being described more than a century ago, it continues to pose unanswered questions regarding its causation, progression, and management (Cipriani et al., 2011). With rising life expectancy and demographic transitions worldwide, the burden of AD is projected to increase substantially, making it imperative to revisit the disease from multiple perspectives (Mayeux& Stern, 2012; Livingston et al., 2020).[8]
The overarching goal of this review Is to synthesize current evidence and provide a comprehensive perspective on Alzheimer’s disease by addressing the following detailed objectives:
This involves examining the neuropathological hallmarks—amyloid-beta (Aβ) plaques, tau neurofibrillary tangles, synaptic degeneration, and cortical atrophy (Serrano-Pozo et al., 2011; Brion, 1998)—while also incorporating recent insights into mitochondrial dysfunction, oxidative stress, and impaired brain glucose metabolism (Blass, 1985; Thakur et al., 2018). The review will highlight how these interconnected mechanisms contribute to progressive neurodegeneration.[9.10]
Age remains the strongest determinant of AD, but genetic mutations in APP, PSEN1, and PSEN2, as well as the APOE ε4 allele, significantly increase susceptibility (Breijyeh&Karaman, 2020). Beyond genetics, modifiable risk factors such as cardiovascular disease, diabetes, sedentary lifestyle, poor diet, social isolation, and low educational attainment contribute to disease vulnerability (Livingston et al., 2020). Understanding these factors is essential for designing preventive strategies.[11]
By tracing the early descriptions of AD and its clinical recognition (Cipriani et al., 2011; McKhann et al., 1984), the review aims to contextualize how diagnostic criteria have evolved—from purely clinical observations to biomarker-based approaches in the preclinical stage (Dubois et al., 2016).[1,12]
Symptomatic treatments such as cholinesterase inhibitors and NMDA receptor antagonists remain the standard of care but offer limited benefits (Yiannopoulou&Papageorgiou, 2020). This review will explore promising new avenues, including monoclonal antibodies against Aβ, tau-targeted therapies, neuroprotective and antioxidant agents, lifestyle-based interventions, and advanced drug delivery systems such as nanotechnology (Singh et al., 2016; Zhang et al., 2024).[2,3,13]
Given the absence of curative therapies, strategies aimed at delaying onset or slowing progression are critical. Multidomain interventions—combining lifestyle modification, cognitive training, and management of cardiovascular risk factors—hold potential for reducing global dementia burden (Livingston et al., 2020).[7,14]
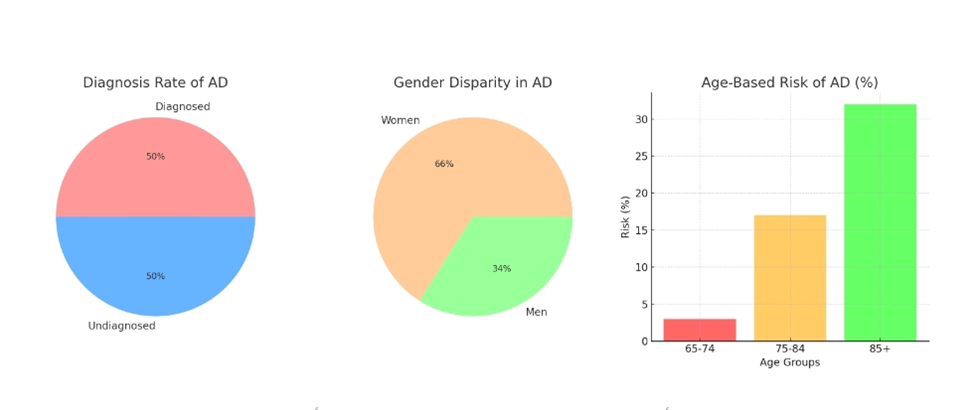
Research across Europe shows that the age-standardized prevalence of Alzheimer’s disease (AD) among people aged 65 and above is about 4.4%. In the United States, a study on adults over 70 reported a higher prevalence of 9.7%. On a global scale, approximately 3.9% of individuals over the age of 60 are affected, although the rates vary by region. In industrialized countries, about one in ten people aged 65 or older, and more than one-third of those over 85, live with some form of dementia.
Incidence studies further highlight the growing burden of AD. In the United States, the incidence among adults aged 65 and above is around 15 per 1,000 person-years, with slightly higher rates in women (16.9) compared to men (13.0). A Swedish follow-up study of older adults found that dementia incidence increased significantly with age: in those aged 75–79, the rates were 19.6 for women and 12.4 for men per 1,000 person-years, while among those 90 years and older, women showed a strikingly higher rate (86.7) compared to men (15.0). A similar pattern of higher female risk is observed in AD overall, with women being about three times more likely to develop the disease and roughly twice as likely to develop dementia of any form.
Other cohort studies also confirm these trends. In Britain, tracking older adults over three years revealed an annual dementia incidence of 9.2 per 1,000 people, with AD specifically responsible for 6.3 cases per 1,000. Historical data from Central Europe reflect similar concerns: in 1983, there were an estimated 35,000 AD patients aged 65 or older in the former Czechoslovakia. Today, the Czech Alzheimer Association reports around 130,000 dementia cases in the country, with two-thirds attributed to AD.[15]
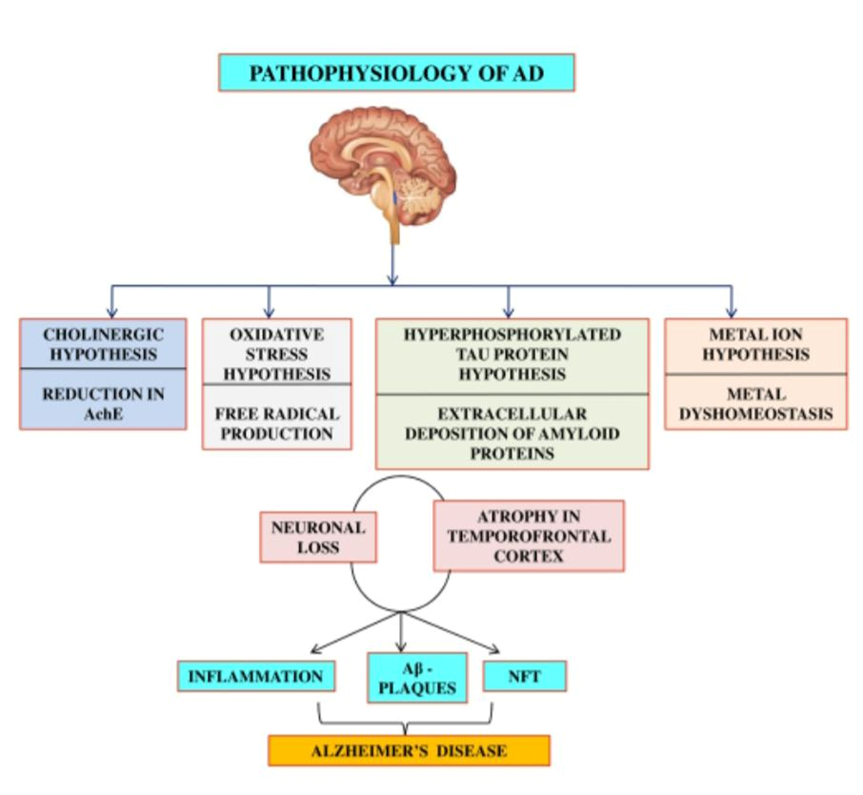
Alzheimer’s disease (AD) is a progressive neurodegenerative disorder characterized by complex and multifactorial mechanisms that collectively impair neuronal communication, synaptic plasticity, and cognitive functions. Its pathophysiology is not attributable to a single abnormality, but rather to a convergence of molecular, cellular, and structural changes within the brain. The following mechanisms represent the core pathological features of AD:
Aβ peptides aggregate into toxic oligomers, fibrils, and plaques. Imbalance between Aβ production and clearance leads to neurotoxicity. Amyloid plaques disrupt neuronal communication and trigger neuroinflammation.[1,2]
Tau stabilizes microtubules, essential for neuronal function. Hyperphosphorylated tau forms NFTs, disrupting neuronal transport and causing cell death.[1,16]
Increased reactive oxygen species (ROS) cause oxidative damage. Mitochondrial dysfunction leads to impaired energy metabolism and apoptosis.[4,17]
Loss of cholinergic neurons leads to decreased acetylcholine. Reduced neurotransmission impairs learning and memory. Acetylcholinesterase inhibitors (e.g., donepezil) provide symptom relief.[1,16,17]
Chronic activation of microglia and astrocytes sustains inflammation. Pro-inflammatory cytokines (e.g., IL-1, TNF-α) worsen neuronal damage.[16,17]
Imbalance of metal ions (e.g., Cu, Fe, Zn) promotes Aβ aggregation. Metal chelation therapy is an emerging treatment option.[1,17]
Neuronal loss affects the hippocampus, amygdala, and cortex. Ventricular enlargement and cortical thinning correlate with disease severity. Neuroimaging techniques (MRI, PET) aid in diagnosis.[17]
Clinical Stages:
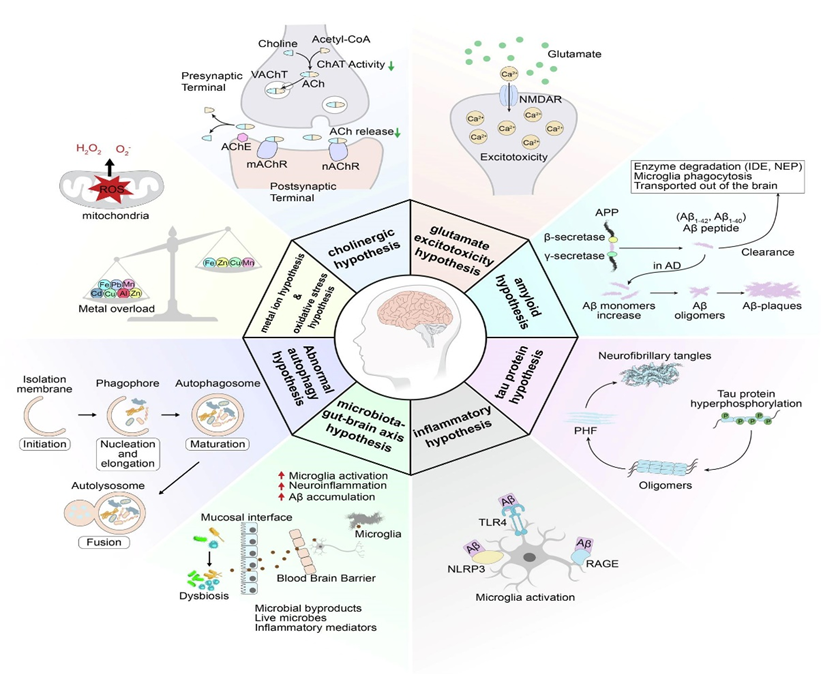
Alzheimer’s disease results from amyloid accumulation, tau hyperphosphorylation, oxidative stress, neuroinflammation, and cholinergic dysfunction. Current treatments manage symptoms, while research explores disease-modifying therapies.
5. Risk Factors:

Ageing:
With age, the risk of neurodegenerative diseases like Alzheimer’s and Parkinson’s increases, affecting about one in ten people over 65. These conditions progress over time, lack curative treatments, and impose a heavy burden on patients and society. Key aging-related changes—such as genetic alterations, mitochondrial dysfunction, protein imbalance, and cellular senescence—play a major role in disease onset. Ongoing research is exploring therapies that target these mechanisms, including boosting NAD?, repairing mitochondria, and slowing cellular aging.[18]
Early-onset familial Alzheimer’s disease, which makes up only 2–5% of cases, is usually caused by inherited mutations in the APP, presenilin 1, or presenilin 2 genes. A strong family history also raises the risk of developing Alzheimer’s. Among genetic factors, the apolipoprotein E (APOE) gene—especially the apoE4 variant—is the most significant, influencing both early- and late-onset forms. Carrying one or more copies of apoE4 increases risk and may lead to earlier disease onset, although its effect lessens with age. Around 15–20% of cases are linked to this gene. Other genes, such as BACE1, ABCA1, ACE, IL-1, and those involved in protein processing, microtubule stability, and cell signaling, also play a role in disease susceptibility.[15]
3.10 Infection:
The role of inflammatory processes in the development of Alzheimer’s disease has led to increased research on how infectious agents contribute to these reactions in the central nervous system. In recent years, many studies have shown a link between various microbial infections, cognitive decline, and Alzheimer’s disease. Systemic infections caused by bacteria and viruses, such as human herpesviruses, spirochetes, Chlamydia pneumoniae, or Borreliaburgdorferi, may raise the level of inflammation and increase the risk of developing Alzheimer’s disease. Certain pathogens may be connected to the onset of Alzheimer’s disease.[19]
3.11 Environmental Factor:
Neurodegenerative diseases like Alzheimer’s are influenced by a mix of genetic, lifestyle, and environmental factors. Recent research highlights that long-term exposure to heavy metals (such as aluminum, lead, mercury, cadmium, and arsenic), air pollution, pesticides, and metal-containing nanoparticles may raise the risk of Alzheimer’s. These exposures can promote amyloid-β buildup, tau hyperphosphorylation, and gene expression changes, leading to neuronal damage. Environmental factors may therefore accelerate or worsen disease progression, making them an important focus for understanding and managing Alzheimer’s. [20]
The global prevalence of Alzheimer’s disease has risen sharply in the past decade, with strong evidence linking it to diabetes mellitus (DM), particularly type 2 diabetes. Insulin resistance and impaired glucose use in the brain contribute to memory loss, inflammation, oxidative stress, and abnormal protein buildup, making diabetes a key risk factor for Alzheimer’s. In the Middle East and North Africa, the rapid rise in DM is tied to urbanization, sedentary lifestyles, and obesity. This review explores how insulin signaling, ApoE genetics, and diabetes-related mechanisms drive Alzheimer’s progression, while also examining genetic studies in Arab populations and the potential of anti-diabetic drugs as therapeutic strategies.[21]
Certain lifestyle factors—such as air pollution, smoking, heavy drinking, poor sleep, and low education—can raise the risk of Alzheimer’s disease. However, healthy habits like eating a balanced diet, exercising regularly, avoiding smoking, limiting alcohol, maintaining a healthy weight, staying mentally active, and getting regular medical checkups can help protect brain health and reduce the chances of memory loss and dementia.[22]
A significantly increased risk of dementia and AD was found in patients who hadsuffered a stroke as well as clinically silent cerebral infarction confirmed by magnetic resonance imaging. Also cardiovascular diseases are associated with an increaseincidence of dementia and AD, with the highest risk of dementia in persons with peripheral artery disease, suggesting that extensive peripheral atherosclerosis is a risk factor for AD. Neuropathological studies have suggested that cerebro-vascularlesions, atherosclerosis and neurodegenerative changes often coexist with each other in the brain, producing a clinical manifestation of the dementia syndrome.[15]
Traumatic brain injury (TBI) is linked to long-term brain changes that resemble Alzheimer’s disease, although the exact connection is still unclear. TBI can damage blood vessels, disrupt the blood–brain barrier, and trigger amyloid-β buildup and tau hyperphosphorylation. These changes worsen cerebrovascular health and may set off degenerative processes leading to Alzheimer’s or related disorders. Current research using biomarkers, animal models, and human studies is helping clarify how TBI contributes to Alzheimer’s-like brain degeneration.[23]
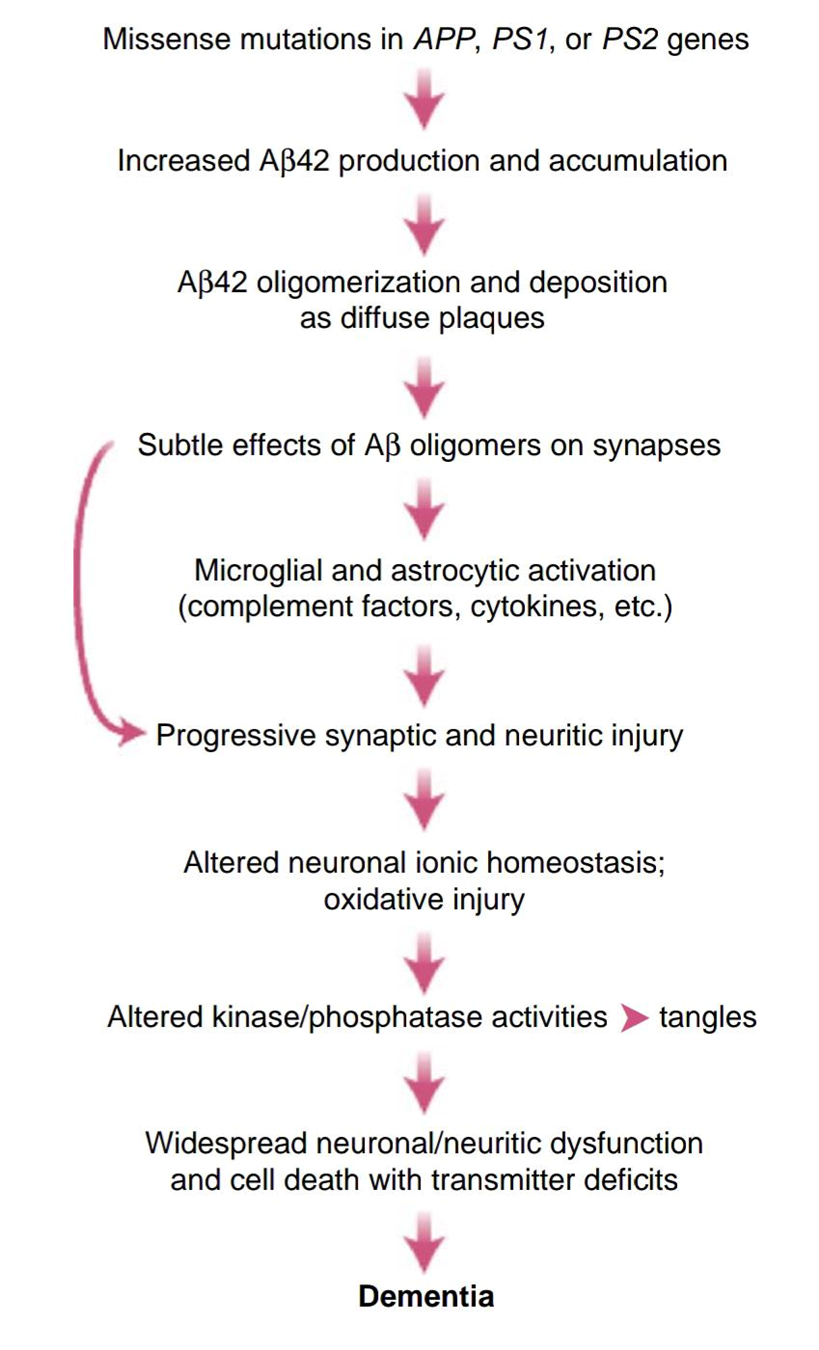
Abnormal buildup of amyloid-beta (Ab) has long been recognized as a key factor in the start and progression of Alzheimer’s disease (AD). These Ab peptides are created when a larger protein, called amyloid precursor protein (APP), is cut by specific enzymes known as beta-secretases (BACE1 and BACE2) and the gamma-secretase complex.[24]
Two important proteins, presenilin 1 and 2 (PS1/2), are crucial for the gamma-secretase to work properly. Mutations in the genes for APP and PS1/2 are often found in people with early-onset, inherited forms of Alzheimer’s.[24]
Because of this central role of Ab and related proteins, many drugs have been developed to try to reduce their levels or block their production, in hopes of treating or slowing down Alzheimer’s disease. [24]
The first attempt at an Alzheimer’s disease vaccine aimed to remove amyloid-beta (Ab) from the brain. This began in 2000 with a clinical trial for a vaccine called AN1792. Unfortunately, some patients developed serious brain inflammation, so the trial had to be stopped early. Researchers then tried a safer approach with a new vaccine, vanutidecridificar, which used a modified carrier to reduce side effects. While this new vaccine was safer, it didn’t lead to any real improvements in memory or thinking, so its trial was also discontinued.[24]
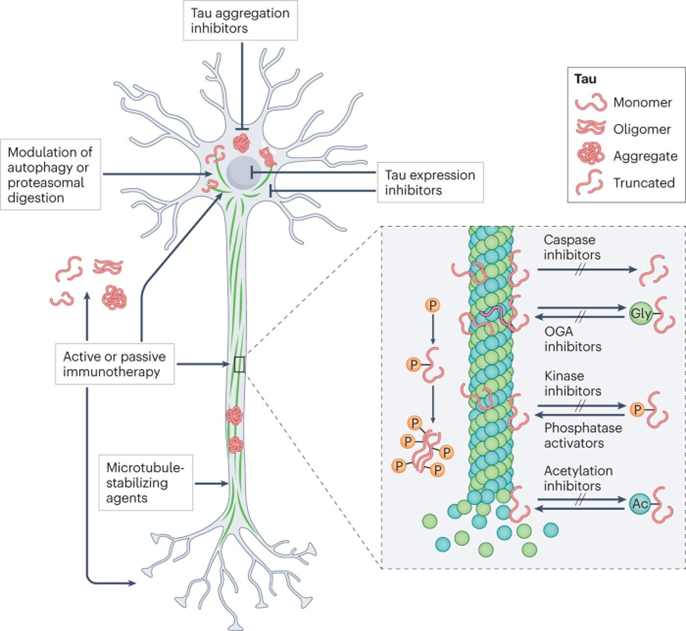
It Prevent tau tangles and Tau protein can generate aggregation finsistantoly to proteolysis and this provides a means for the Tau aggregrates with NFTs. These tau inclusions are Competent to seed and to spread the pathology into other Regions.Blocking p-tau aggregation could be very beneficial in treating Alzheimer’s disease. By preventing these harmful proteins from clumping together, p-tau aggregation inhibitors have the potential to become one of the next disease-modifying therapies (DMTs) for Alzheimer’s. This approach offers hope for slowing down or even stopping the progression of the disease. Phenothiazine Derivative Methylene blue can impart the inhibition ability on p-tau to form filaments. [25]
Tau lesions are better associated with the extent of dementia than Aβ lesions, and therefore the removal Of aggregated p-tau might be more efficient when AD Cognitive symptoms are marked. Currently, immunotherapy is the most promising manner to enhance p-tau clearance, including Active immunity (mainly vaccine) and Passive immunity (mainly monoclonal antibody). In the context of active immunity, the ACI-35 vaccine can trigger a fast immune response in wild.
Right now, three different types of antitau monoclonal antibodies called IIB076, JNJ-63733657 and LY3303560—are being tested in early stage (phase 1) clinical trials.[25] These Anti-tau antibodies are designed to help blocking the buildup and spread of tau proteins, neutralizing harmful forms of tau and helping the body clear them away.[25-29]
Anti-tau antibodies are gosuranemab, semorinemab, tilavonemab, zagotenemab, etc.
Fig: Researchers are exploring several ways to target tau protein in the fight against Alzheimer’s disease and related conditions. Some promising approaches are alreadybeing tested in labs and clinical trials. For example, antisense oligonucleotides can help lower the amount of tau produced in the brain. There are also drugs like curcumin and LMTX (a methylene blue derivative) that aim to stop tau proteins from clumping together.Since tau normally helps stabilize microtubules in brain cells, scientists are also testing microtubule stabilizers such as TPI-287 and NAP to make up for this lost function. Another strategy is to help the brain clear out abnormal tau by boosting natural processes like autophagy or proteasomaldegradation.Immunotherapy is another exciting area. Both active and passive immunotherapies use antibodies to find and remove harmful tau, whether it’s inside or outside of cells.Tau proteins can undergo many changes after they’re made, such as hyperphosphorylation, acetylation, and truncation. These changes can make tau more toxic, but some, like glycosylation, can be either helpful or harmful. Scientists are also developing drugs that block the enzymes responsible for these modifications, hoping to prevent tau from becoming dangerous in the first place.[29]
Anti-tau therapies.In AD, NFTs, a dense accumulation of paired helical filaments of hyperphosphorylated tau, are one of the main pathogenetic elements. According to the β-amyloid hypothesis, first postulated in 1991, the NFT formation follows the aggregation of β-amyloid . A shift between an overproduction and a deficiency of the amyloid peptide in the brain tissue causes the amyloid peptide to aggregate and deposit in the form of toxic senile plaques. This activates hyperphosphorylation of tau.[26]and acetylation , truncation and glycosylation it is themodification type of tau in AD result hyper phosphorylation are increase the activity of tau.[29]
Tau positron emission tomography (tau PET), neurofilament light, and neurogranin are the new biomarkers that are Increasingly used by clinical trials.[28]
Aggregation inhibitors interact directly with the Aβ Peptide to inhibit Aβ42 fiber formation, thus they are considered potential therapeutic for AD.[28]
Alzheimer’s disease has been recognized for nearly a century (Ramirez-Bermudez, 2012), yet treatment options remain limited. And now the only 4 cholinesterase inhibitors and memantine are approved from the US by FDA.While these medications can help manage symptoms, they do not change the underlying progression of the disease. As a result, there is growing interest in developing new therapies that can actually modify the course of Alzheimer’s. However, the complex and varied mechanisms involved in the development of this condition make it challenging to create truly effective treatments.[27]
Since the early 2000s, scientists have tried many different ways to target amyloid-beta (Aβ) in the hopes of treating Alzheimer’s disease. Unfortunately, most of these attempts haven’t worked out—either because of safety issues or because they didn’t show clear benefits for patients. Despite these setbacks, research is still ongoing, and many clinical trials are underway . [30]
One of the most promising strategies to emerge involves using antibodies to target Aβ. This can be done through passive immunotherapy, where patients receive monoclonal antibodies, or through active immunization, which works more like a vaccine.[30]
The recently lecanemab and donanemabhave approved use of Alzheimer’s disease treatment. For the first time, patient have a option to take medication that can slow down the fatal disease giving them more valuable time and helping them hold on to their memories a little longer and these vaccines are given as an IV infusion so, patient and caretaker are often must travels tospeciality healthcare center once or twice a month .and especially who have busy schedules.[31-33]
CRISPR/Cas9 is an exciting gene-editing tool that’s opening up new possibilities for understanding and treating neurodegenerative diseases like Alzheimer’s, which still don’t have truly effective treatments[34]. CRISPR/Cas9 has been applied to identify and edit genes involved in oxidative stress, a key contributor to AD pathogenesis, offering potential therapeutic avenues to mitigate related neuronal damage . Since most mutations in the APP, PSEN1, and PSEN2 genes are associated with increased Aβ production, the use of CRISPR/Cas9 to correct these mutations in brain cells could help reduce Aβ accumulation [34].
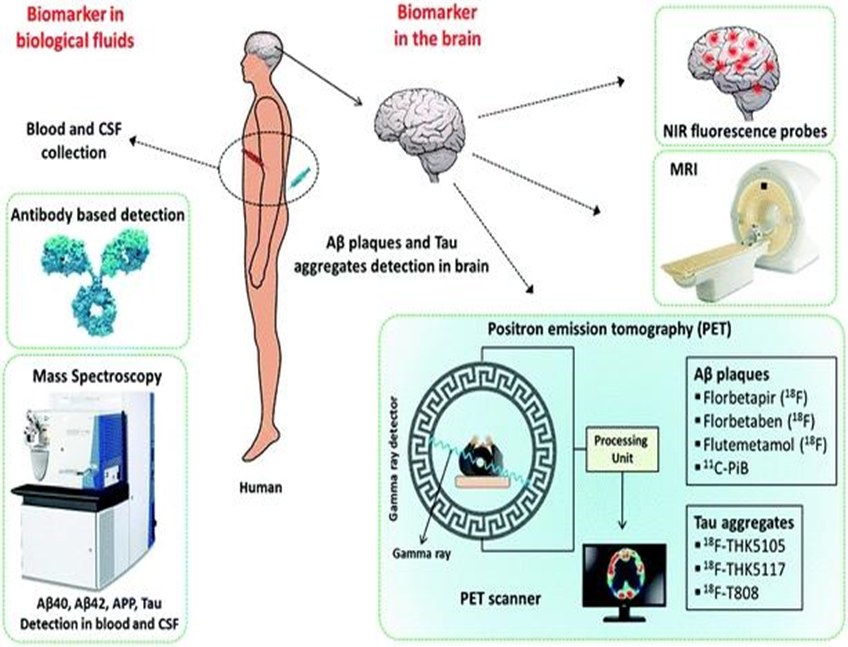
Fig.: Molecular tools and techniques available for the detection of biomarkers in AD.
Fluorescent probes offer a real-time, safe, and affordable way to get detailed images of Aβ species in the brain—without the need for radioactive materials. Among these, far-red fluorescent probes stand out. They’re especially useful for detecting and imaging Aβ species, and they come with unique benefits that set them apart from standard probes.[32]
PET is considered to be a potential technique that may serve this purpose. In this context, 11C-labelled Pittsburgh compound B (11C-PiB), which is a radioactive analogue of ThT, was one of the first tracers used to image Aβ plaques in the brain.[35]
Magnetic resonance imaging, or MRI, is a safe and non-invasive way to look at the brain’s structure and how it works. There are two main types of MRI: structural MRI (sMRI), which shows us what the brain looks like, and functional MRI (fMRI), which helps us understand how the brain is working in real time.[36]
fMRI is especially useful for exploring how our brains function—like how we form memories, how our thinking changes as we age, and how our brain cells communicate with each other. Research using fMRI has revealed that the brain’s networks can change quite a bit as we get older, and these changes are even more noticeable in conditions like mild cognitive impairment (MCI) and Alzheimer’s disease (AD).[36]
When it comes to treating Alzheimer’s disease (AD), there are only a handful of medications that have been approved. These include drugs known as AChE inhibitors, such as Aricept (donepezil), Nivalin (galantamine), Rivastach (rivastigmine), and Cognex (tacrine). These medications work by helping to boost levels of a chemical in the brain that’s important for memory and thinking. There’s also Namenda (memantine), which works a bit differently as a weak antagonist of the NMDA receptor, helping to regulate another brain chemical involved in learning and memory. While these treatments can help manage symptoms, they don’t cure Alzheimer’s disease.[37]
It was discovered that Aβ is released into the cerebrospinal fluid (CSF), which opened the stage for scientists to develop tests that could measure Aβ levels in the CSF. However, the first studies that looked at the overall amount of Aβ in the CSF didn’t deliver the results researchers had hoped for. And no more or minor differences between controls and Alzheimer’s patient.[33]
Alzheimer’s disease continues to touch millions of lives around the world, presenting a significant challenge for families and communities. While we don’t yet have a cure, there is growing hope. New therapies are beginning to slow the progression of the disease, and exciting research into areas like amyloid, tau, neuroinflammation, and regenerative medicine is opening doors to more effective and personalized treatments.
REFERENCES


Anamika Koshti, Jinal Jadeja*, Mayuri Vaja, Ashok Kumar, Divyakant Patel, Alzheimer’s Disease: Pathophysiology, Risk Factors and Emerging Therapeutic Strategies, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 688-703 https://doi.org/10.5281/zenodo.17532576
 10.5281/zenodo.17532576
10.5281/zenodo.17532576