
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Samarth College of Pharmacy, Belhe, Pune, Maharashtra, India, 412410
Cervical cancer is 4th most common cancer among women globally with around 6,60,000 new cases and around 3,50,000 deaths in 2022. Most cervical cancers are caused by Human Papillomavirus (HPV), a sexually transmitted infection. HPV spreads through sexual contact (anal, oral or vaginal) and can lead to cancer. Only certain types of HPV cause cervical cancer. The two types that most commonly cause cancer are HPV-16 and HPV-18. Signs and symptoms of cervical cancer include abnormal vaginal bleeding, such as bleeding after vaginal sex, bleeding after menopause, bleeding and spotting between periods, or having (menstrual) periods that are longer or heavier than usual, bleeding after douching may also occur, an unusual discharge from the vagina which may contain some blood and/or occur between your periods or after menopause, pain during sex, pain in the pelvic region. The four main treatments are surgery, radiation therapy, chemotherapy, targeted therapy.
One of the most common gynaecologic diseases in the world is still cervical cancer. Based on available statistics, it is the fourth most prevalent cancer in women globally and ranks 14th overall. Cervical cells are where cervical cancer begins. The lower, narrow end of the uterus, or womb, is called the cervix. The uterus and vagina (birth canal) are connected by the cervix. Typically, cervical cancer progresses gradually over time. Cervical cells undergo a process called dysplasia, in which aberrant cells start to show up in the cervical tissue, prior to cancer developing in the cervix. The aberrant cells may eventually develop into cancer cells and begin to proliferate and spread farther into the cervix and surrounding regions if they are not eliminated or eliminated. Primary and secondary prevention are the main goals of cervical cancer intervention. The most effective ways to reduce the incidence and mortality of cervical cancer are through primary prevention and screening.[1] With racial, ethnic, and age differences, screening rates are lower in low-socioeconomic and low-resource locations. According to studies, women who are obese and suffer from chronic illnesses may be less likely to get screened for breast and cervical cancer. Cervical cancer is avoidable because it is a STI, and by focusing on education, screening, and prevention, the incidence of cervical cancer can be decreased worldwide. Cervical cancer preventative vaccinations have been available since 2006. When the World Health Organization (WHO) called for the universal eradication of cervical cancer in May 2018, almost 70 nations and international academic bodies responded right once. Subsequently, on November 17, 2020, the World Health Organization unveiled the global strategy to expedite the eradication of cervical cancer as a public health issue in order to illuminate the path for future cervical cancer prevention and control. This means that 194 nations have committed to working together to eradicate cervical cancer for the first time.[2]
2. BIOLOGY OF CERVICAL CANCER
The mucus-secreting columnar epithelium and stratified squamous epithelium that envelop the cervix are especially susceptible to viral neoplastic transformation at the squamocolumnar junction. Adenocarcinomas are more prevalent in endocervix tumors, but squamous cell carcinomas are the most prevalent kind. The majority of cervical cancer cases are caused by HPV infection, which is responsible for 95% of malignant lesions. It may take years or decades for dysplasia to develop into aggressive cancer.
Over 99 percent of cervical malignancies are caused by a persistent HPV infection. Worldwide, there are over 250,000 cervical cancer-related fatalities and over 500,000 new cases of the disease each year. Developing nations account for 80% of instances. About 4,000 women in the US lose their lives to cervical cancer each year. Low-resource communities have a far higher death rate and more disparities in evidence-based care for women, Black people, and Hispanic people. Women who have not been screened in the previous five years and those who do not have regular follow-up when a precancerous cervical lesion is discovered have a higher mortality rate. According to trends, women who are most at risk for mortality might be less likely to get vaccinated against HPV.[3]
Symptoms of Cervical Cancer: Early cervical cancer commonly has no symptoms, which is why screening is necessary to detect it. The most common actual symptoms are:
Vaginal bleeding: Because of the cervix's extremely delicate surface, tumours leak readily. In reality, a woman's overall risk of developing cervical cancer is around 30% if she experiences fresh vaginal bleeding after menopause. Women with premenstrual syndrome are frequently at risk for bleeding throughout their periods, strong menstrual flow, spotting bleeding during periods, or after sexual activity.
Vaginal discharge: White or often yellowish foul-smelling discharge that may occur with particularly advanced or necrotic cancer.
Cervical pain: When inserting a tampon or finger rather than the vagina, cervical pain is felt. This cervical motion pain raises the possibility of an infection or malignancy upon physical examination. Pelvic pain may be widespread in cases of more severe disease.
Urinary symptoms: As the tumour spreads into the vagina and eventually blocks the kidneys' ability to drain urine, urinary symptoms appear as the disease progresses. The most frequent cause of cervical cancer-related deaths is uraemia.
Signs of spread to other areas of the body include: lymph gland enlargement in the groin or collar bone are or the left armpit. Advanced spread may give bone, liver, lung, bowel or brain abnormalities.
The late symptoms: can be weight loss, anaemia and body lethargy.
Human Papillomavirus (HPV) infection: 99% of cervical cancer cases Most cervical cancer cases are caused by the sexually transmitted human papillomavirus (HPV). This is the same virus that causes genital warts. There are about 100 different strains of HPV. Only certain types cause cervical cancer. The two types that most commonly cause cancer are HPV-16 and HPV-18.[5]
10. STAGES OF CERVICAL CANCER [14]
A cancer?stage describes the extent of cancer in the body, especially whether the cancer has spread from where it first formed to other parts of the body. It is important to know the stage of cervical cancer in order to plan the best treatment.
Stage I: cervical cancer?has formed and is found in the?cervix?only. It is divided into stages IA and IB, based on the size of the tumor?and the deepest point of tumor invasion.
Stage II cervical cancer:
In stage II, cervical cancer?has spread to the upper two-thirds of the?vagina?or to the tissue?around the?uterus.
Stage II is subdivided based on how far the cancer has spread.
Stage III cervical cancer:
In stage III, cervical?cancer?has spread to the lower third of the?vagina and/ or to the pelvic wall, and/ or has caused kidney problems, and/ or involves lymph nodes.
Stage III is subdivided based on how far the cancer has spread.
Stage IV cervical cancer:
In stage IV, cervical cancer?has spread beyond the?pelvis, or has spread to the lining of the bladder or rectum, or has spread to other parts of the body.
Stage IV is subdivided into stages IVA and IVB, based on where the cancer has spread.
11. RECURRENT CERVICAL CANCER
Recurrent cervical cancer is cancer that has recurred (come back) after it has been treated. The cancer may come back in the cervix or as metastatic tumors in other parts of the body.?Tests will be done to help determine where the cancer has returned in your body, if it has spread, and how far.?The type of treatment that you have for recurrent?cervical?cancer will depend on how far it has spread.
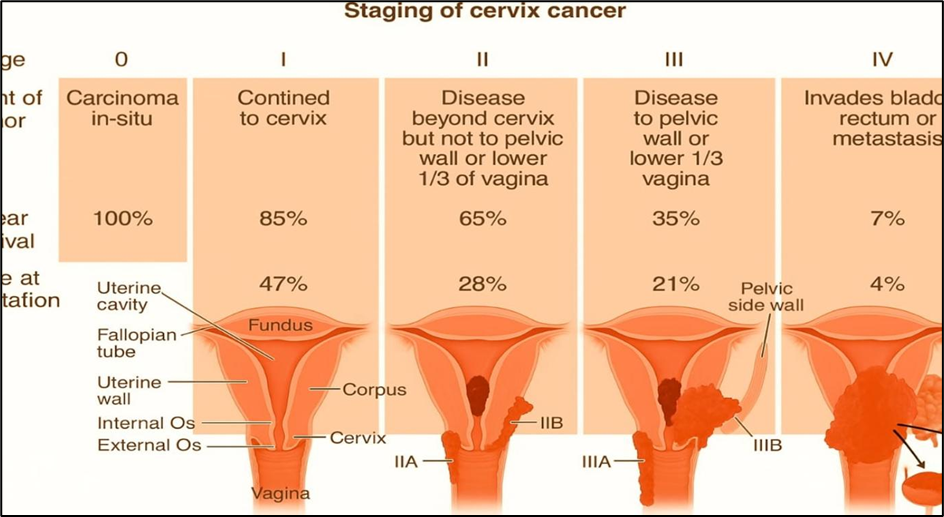
Fig.2 Staging of Cervix Cancer
12. PATHOPHYSIOLOGY OF CERVICAL CANCER
Step 1: HPV Infection
Step 2: Viral Replication
Step 3: Integration and Oncogenesis
Step 4: Immune Evasion
Step 5: Angiogenesis and Metastasis
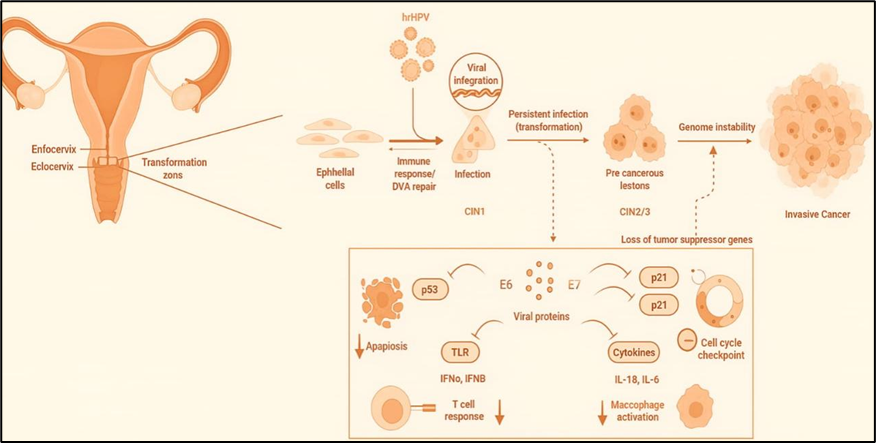
Fig.1 Key Molecular Alteration
13.TYPES OF CERVICAL CANCER
1. Squamous Cell Carcinoma (SCC): 70-80% of cervical cancer cases
2. Adenocarcinoma (AC): 10-20% of cervical cancer cases
3. Adenosquamous Carcinoma (ASC): 3-5% of cervical cancer cases
4. Small Cell Carcinoma (SCC): 1-2% of cervical cancer cases
5. Large Cell Carcinoma (LCC): rare
6. Glassy Cell Carcinoma (GCC): rare
7. Mucoepidermoid Carcinoma (MEC): rare
8. Serous Carcinoma (SC): rare
Rare and Unusual Types
14. MECHANISM OF HPV 16 INDUCED CANCER
Step 1: Viral Entry
Step 2: Viral Replication
Step 3: Expression of Oncoproteins
Step 4: Inhibition of Tumor Suppressor Proteins [19,20,7]
Step 5: Disruption of Cell Cycle Regulation[24]
Step 6: Epigenetic Changes [25,26]
Step 7: Cervical Cancer Development [6]
Step 8: Progression to Invasive Cancer [23]
15. TREATMENT
The treatment of cervical cancer depends on several factors, including the stage of cancer, the patient’s overall health, and whether the cancer has spread to other areas. Treatment options are typically grouped into the following categories:
Surgery is often the primary treatment for early-stage cervical cancer and can also be used in combination with other therapies for more advanced stages. Surgical options include:
Radiation therapy uses high-energy radiation to kill cancer cells or shrink tumors. It is often used for patients with more advanced stages of cervical cancer or as part of adjuvant therapy (after surgery). There are two types of radiation used in cervical cancer treatment:
Chemotherapy involves the use of drugs that kill cancer cells or prevent their growth. It is commonly used for more advanced cervical cancers, cancers that have spread (metastasized), or recurrent cancer. Chemotherapy is often given in combination with radiation therapy (chemoradiation) to enhance treatment efficacy.
Immunotherapy is a newer treatment approach that enhances the body's immune system to recognize and fight cancer cells. It is often used for advanced or recurrent cervical cancer.
Targeted therapies are drugs that specifically target molecules involved in the growth and spread of cancer. These therapies are designed to affect cancer cells more precisely while sparing healthy cells. Some examples include:
Hormone therapy is not typically used for cervical cancer since it is not hormone-driven like other cancers (e.g., breast or prostate cancer). However, in some rare cases where cervical cancer has spread or recurred, hormonal therapy might be considered if there are estrogen receptors on the cancer cells.
For young women diagnosed with early-stage cervical cancer who wish to preserve their fertility, there are fertility-sparing options, including:
For patients with advanced or metastatic cervical cancer, palliative care focuses on alleviating symptoms and improving quality of life. It may include:
16. RECENTLY APPROVED VACCINE
for the prevention of cervical cancer. If given before sexual maturity, these vaccines can provide up to 90% protection against cervical cancer. These vaccines are:
a. Gardasil [32]
In December 2014, the FDA approved Gardasil 9, which protects against nine strains of HPV.
Gardasil is available as Gardasil which protects against 4 types of HPV (6, 11, 16, 18) and Gardasil 9 which protects against an additional 5 types (31, 33, 45, 52, 58).
Gardasil™ is given at 0, 2, and 6 months. This means after you take the first dose, the next dose needs to be taken after two months and thereafter 6 months.
GARDASIL 9 should be administered intramuscularly in the deltoid region of the upper arm or in the higher anterolateral area of the thigh.
The safety of GARDASIL 9 was evaluated in six clinical studies that included more than 13,000 individuals & it is used in both males and females.
Cervarix™ is given at 0, 1, and 6 months. This means after you take the first dose, the next dose needs to be taken after a month and thereafter 6 months.
Immunization with Cervarix consists of 3 doses of 0.5-mL each, by intramuscular injection according to the following schedule: 0, 1, and 6 months. The preferred site of administration is the deltoid region of the upper arm. Cervarix is available in 0.5-mL single-dose vials and prefilled TIP-LOK syringes. Cervarix is used only in female.
The most common local adverse reactions in patients were pain, redness, fatigue, headache, muscle pain, gastrointestinal symptoms, and joint pain and swelling at the injection site.
Cervarix was voluntarily taken off of the market in the US in 2016 due to low demand.
India's first indigenously developed vaccine to prevent cervical cancer, CERVAVAC, is all set to be available later this year, costing between ?200-400 a shot. CERVAVAC will be effective against at least four variants of Human Papilloma Virus (HPV). While the vaccines must be given to both young boys and girls, chances of getting this cancer are more among women.
Several brands of HPV vaccines are available in India, including Gardasil 9, a nonavalent vaccine priced at approximately Rs 10,000 per dose, Gardasil 4 (quadrivalent) at around Rs 4,000 per dose, and Cervavac, an indigenous quadrivalent vaccine by the Serum Institute of India, priced at about Rs 2,000 per dose. All of these vaccines are safe, with no major side effects reported so far.
The FDA has approved several treatments for cervical cancer in recent years, particularly focusing on immune checkpoint inhibitors and targeted therapies. These treatments are typically used for advanced or recurrent cervical cancer, especially after chemotherapy has failed.
B. Atezolizumab (Tecentriq) [35]
C. Niraparib (Zejula) [36]
18. CURRENT RESEARCH AREAS FOR THE TREATMENT OF CERVICAL CANCER [37]
a. Immunotherapy
Immunotherapy continues to be a promising area of research for cervical cancer treatment, especially for advanced or recurrent cases. Several immune checkpoint inhibitors, such as pembrolizumab (Keytruda), nivolumab (Opdivo), and cemiplimab (Libtayo), are already in use for treating advanced cervical cancer. Current research is focused on:
b. Targeted Therapy
Research in targeted therapies is focused on drugs that block specific molecules or pathways driving cervical cancer. Key areas include:
c. Personalised and Precision Medicine
Advances in genomic profiling are helping to develop more personalized treatment plans. By analyzing the genetic makeup of cervical cancer cells, researchers hope to identify specific mutations that can be targeted with drugs or other therapies. Liquid biopsy technologies, which analyze tumor DNA from blood samples, are also being studied to monitor disease progression and tailor treatments to individual patients.
d. Therapeutic Vaccines
While HPV vaccines are primarily used for prevention, therapeutic vaccines are in development to treat existing cervical cancer. These vaccines aim to stimulate the immune system to recognize and attack HPV-infected cells that have progressed to cancer. Some of these therapeutic vaccines are designed to target specific viral proteins (like E6 and E7) that are present in HPV-driven cancers.
e. Adoptive Cell Therapy (ACT)
Adoptive T-cell therapy, including CAR-T cell therapy, is being explored for cervical cancer. This involves extracting and modifying a patient's immune cells to enhance their ability to target and destroy cancer cells. Although CAR-T therapy has shown success in blood cancers, research is ongoing to adapt this approach for solid tumors like cervical cancer.
Advances in radiation techniques are providing more targeted and effective treatments with fewer side effects. Proton therapy and stereotactic body radiation therapy (SBRT) are being researched for cervical cancer, offering the possibility of delivering higher doses of radiation to tumors while minimizing damage to surrounding healthy tissue.
g. HPV Vaccine Development
Researchers are working on new HPV vaccines that target additional strains of the virus, further improving protection against cervical cancer. These vaccines could help reduce the incidence of cervical cancer globally by preventing HPV infection, especially in populations where vaccine uptake is lower.
h. Combination Therapy Approaches
Combinations of chemotherapy, radiotherapy, immunotherapy, and targeted therapies are being explored to improve efficacy. Research is focused on finding the best combinations to treat cervical cancer while minimizing side effects and resistance.[38-42]
CONCLUSION
Cervical cancer remains a significant global health concern, with human papillomavirus (HPV) as the primary cause. While prevention through vaccination has substantially reduced the incidence of cervical cancer, early detection and effective treatment remain crucial for managing the disease, particularly in advanced stages. Recent advancements in cervical cancer treatment, including the approval of novel drugs and vaccines, alongside ongoing research, offer renewed hope for patients and clinicians alike.
In recent years, the approval of immunotherapies such as cemiplimab (Libtayo) and atezolizumab (Tecentriq) marks a significant shift toward immune checkpoint inhibitors as a cornerstone of treatment for advanced, recurrent, or metastatic cervical cancer. These therapies enhance the immune system's ability to target and eliminate cancer cells, especially in tumors expressing PD-L1. Such therapies, either alone or in combination with chemotherapy, have shown promising results, extending survival and improving quality of life for many patients.
The HPV vaccine has revolutionized prevention, significantly reducing the incidence of cervical cancer by targeting the HPV types responsible for the majority of cases. Newer HPV vaccine formulations and expanded coverage to additional strains continue to evolve, offering greater protection and potentially lowering cervical cancer rates globally. Therapeutic vaccines are also under investigation, aiming to treat existing HPV-related cancers by stimulating the immune system to target infected cells, further advancing the promise of personalized cancer immunotherapy.
Ongoing research into targeted therapies, including PARP inhibitors and angiogenesis inhibitors, is providing hope for patients with specific genetic mutations or metastatic disease. These therapies are being explored in combination with other treatments to overcome resistance and increase efficacy. Additionally, the use of genomic profiling and liquid biopsy technologies to personalize treatment is likely to further improve outcomes by identifying patients most likely to respond to particular therapies.
REFERENCES





Prajakta Shingote, Ajay Bhagwat, Aarti Malkapure, Prasad Jadhav, Akshada Thorat, Cervical Cancer: Current Perspectives on Pathophysiology, Diagnosis, Prevention, and Therapeutic Advances, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 2393-2408. https://doi.org/10.5281/zenodo.17432542
 10.5281/zenodo.17432542
10.5281/zenodo.17432542