
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Department of pharmaceutics, Punjab college of Pharmacy.
2Department of pharmaceutics, Maharaja Agrasen school of Pharmacy.
Cervical cancer remains a leading gynecological malignancy and an important global health challenge, particularly in low- and middle-income regions. The disease originates in the cervix when epithelial cells undergo genetic and molecular changes, most often triggered by persistent infection with high-risk human papillomavirus (HPV) strains, mainly HPV-16 and HPV-18. While HPV infection is widespread, additional cofactors—including smoking, high parity, long-term oral contraceptive use, immunosuppression, and lack of screening—contribute to malignant progression. Histologically, squamous cell carcinoma represents the majority of cases, followed by adenocarcinoma, adenosquamous carcinoma, and rarer aggressive variants. Clinical presentation ranges from asymptomatic disease detected through screening to symptoms such as abnormal bleeding, unusual discharge, pelvic pain, and advanced complications involving the urinary or gastrointestinal tract. Diagnostic evaluation integrates screening tools (Pap smear and HPV DNA testing), colposcopy with targeted biopsy, and imaging for staging. Treatment strategies depend on disease stage, ranging from fertility-sparing surgery in early cases to chemoradiotherapy and systemic therapy for advanced or recurrent disease. In recent years, therapeutic advances have significantly expanded options for patients with persistent or metastatic disease. These include immune checkpoint inhibitors, antibody–drug conjugates, precision-targeted therapies guided by molecular profiling, and experimental immunotherapies such as therapeutic HPV vaccines. Integration of these modalities into multidisciplinary care has improved survival and quality-of-life outcomes. This review highlights the epidemiology, pathogenesis, clinical features, diagnostic pathways, and evolving therapeutic landscape of cervical cancer, with emphasis on recent innovations that may contribute to the World Health Organization’s goal of eliminating cervical cancer as a public health problem.
Cervical cancer remains a significant gynecological malignancy and a major public health concern, particularly in low- and middle-income countries. It arises in the cervix, the lower part of the uterus that connects to the vagina. The disease develops when cervical epithelial cells undergo genetic alterations, leading to uncontrolled proliferation and invasion of surrounding tissues1. The most important causative factor is persistent infection with oncogenic human papillomavirus (HPV) strains, particularly HPV 16 and HPV 18, which are collectively responsible for the majority of cases worldwide2. Although HPV infection is common, only a subset of women progress to cancer due to the influence of cofactors such as early sexual activity, multiple pregnancies, long-term use of oral contraceptives, smoking, immunosuppression, and lack of routine screening3,4. Cervical cancer is largely preventable through the implementation of HPV vaccination and regular screening. The vaccines currently available are highly effective in reducing the incidence of precancerous lesions and invasive disease5. Screening methods, including Pap smears and HPV DNA testing, allow for early identification and treatment of precancerous changes before malignant transformation occurs4. Despite these preventive strategies, cervical cancer continues to cause considerable morbidity and mortality worldwide. More than 600,000 new cases and over 340,000 deaths are reported annually, with the highest burden in resource-limited regions2. To address this, the World Health Organization (WHO) has developed a global strategy aiming to eliminate cervical cancer as a public health problem through universal vaccination, screening, and timely treatment2.

Figure1: Cervical Cancer
Types of Cervical Cancer
Cervical cancer is classified based on the type of epithelial cell from which it originates. The two main histological types are squamous cell carcinoma and adenocarcinoma, while several rare variants also exist.
1. Squamous Cell Carcinoma (SCC)
2. Adenocarcinoma
3. Adenosquamous Carcinoma
4. Rare Types
Although uncommon, other histological subtypes include:
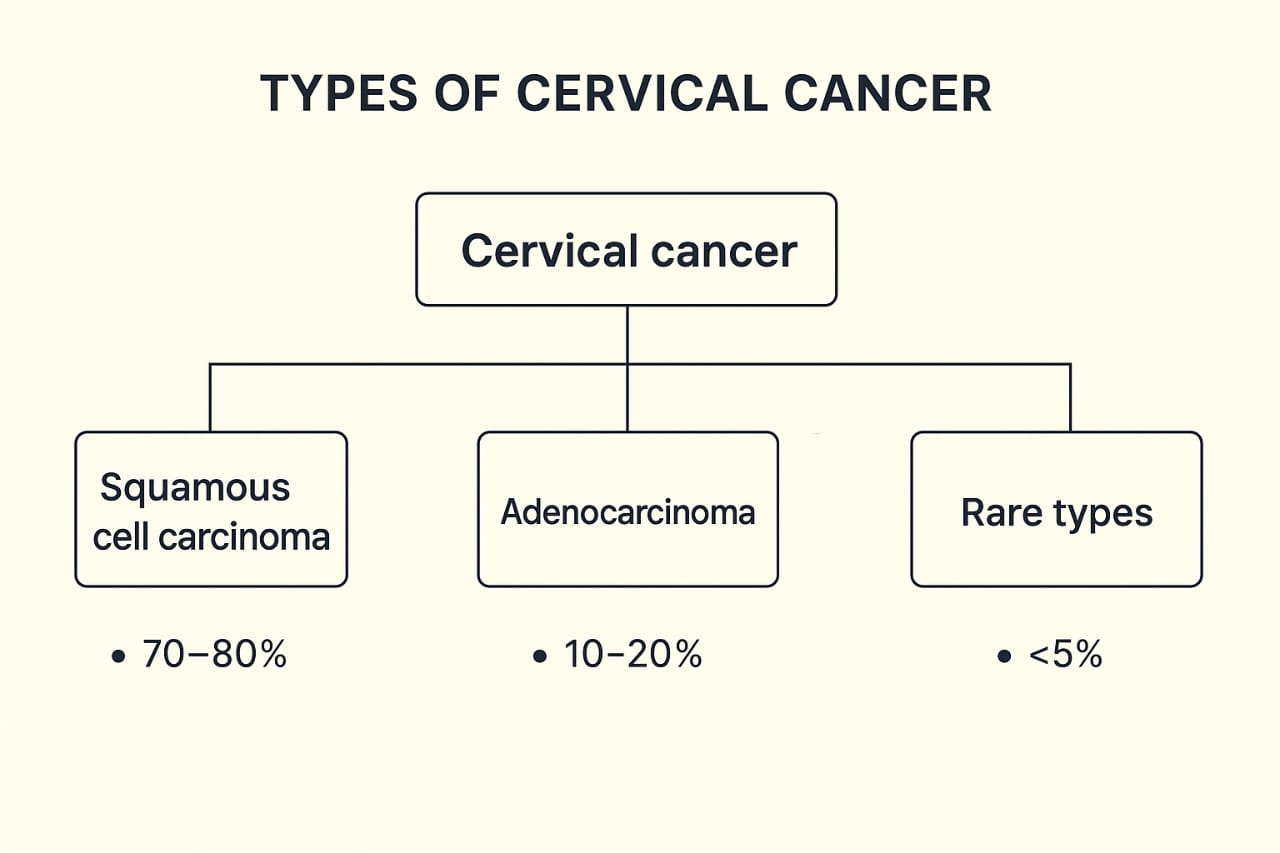
Fig 2- Types of cervical cancer
Causes of Cervical Cancer
Cervical cancer primarily arises from persistent infection with high-risk human papillomavirus (HPV) types, particularly HPV-16 and HPV-18. These oncogenic viruses produce proteins (E6/E7) that disrupt the function of tumor suppressor genes, triggering abnormal cell growth and potentially cancerous progression10. However, the presence of HPV alone does not always lead to cancer. A number of cofactors influence the progression from HPV infection to cervical cancer:
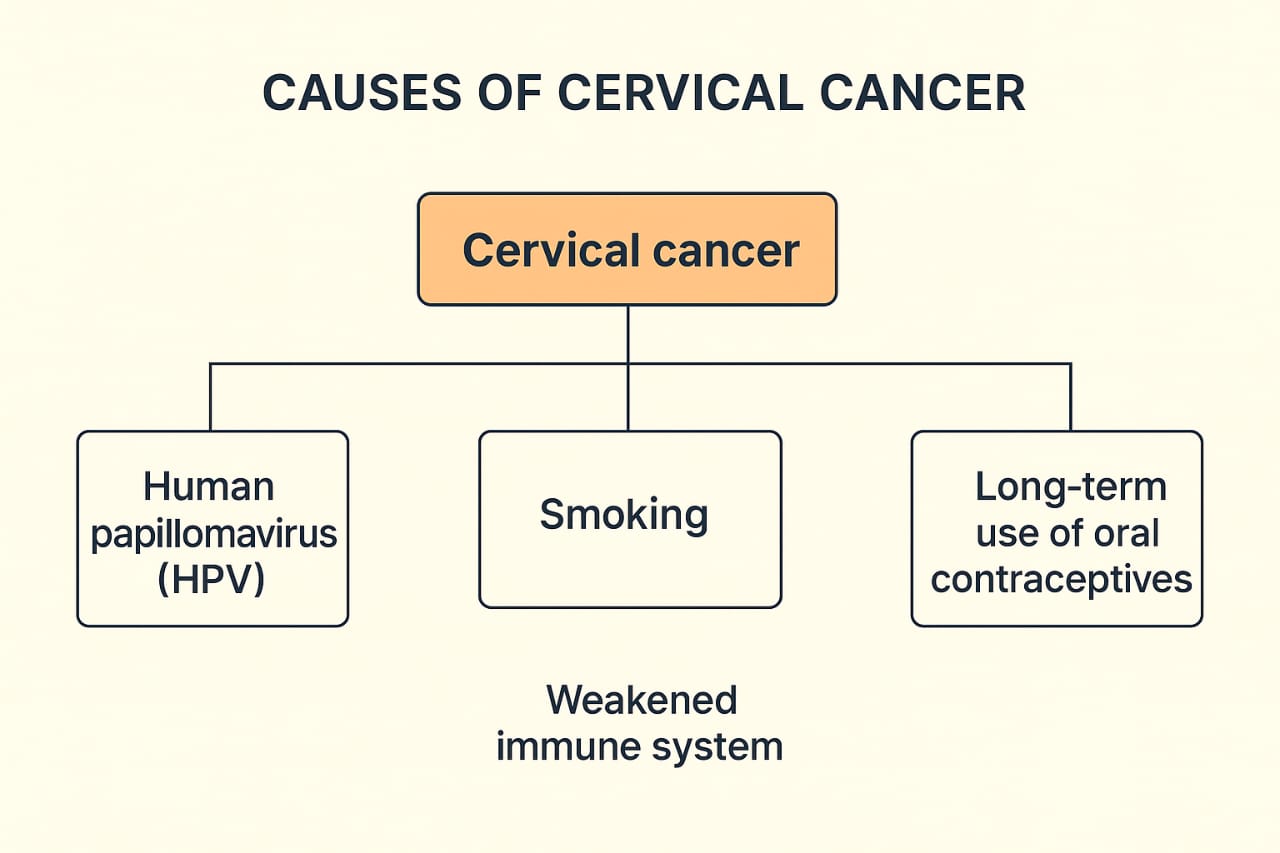
Figure 3- Causes Of Cervical Cancer
Signs and Symptoms of Cervical Cancer
Cervical cancer often develops slowly and may remain asymptomatic in its early stages, which is why regular screening plays a crucial role in detection. When symptoms appear, they may indicate disease progression.
1.Abnormal Vaginal Bleeding-The most common presenting symptoms may occur between menstrual periods, after sexual intercourse, or post-menopause 15.
2.Unusual Vaginal Discharge-Discharge may be watery, pink, or foul-smelling.Often associated with advanced disease due to necrosis or infection in cervical tissue16.
3.PelvicPain-Persistent pain in the pelvic region or lower back may develop. Pain can radiate to the legs or hips in advanced stages17.
4. Pain During Sexual Intercourse (Dyspareunia)-Caused by tumor growth in the cervix or invasion into surrounding structures18.
5. Urinary and Bowel Symptoms-In later stages, cervical cancer may invade the bladder or rectum, leading to painful urination, hematuria, constipation, or rectal bleeding19. The diagnosis of cervical cancer is a stepwise process that begins with screening, followed by confirmatory tests and staging investigations. Early detection is essential for effective treatment and improved survival outcomes.
Biopsies—such as punch biopsy, endocervical curettage, or cone biopsy—provide definitive confirmation of invasive cervical cancer. Histology also determines the cancer type (squamous cell carcinoma or adenocarcinoma) and grade22,23.
Once cancer is confirmed, imaging helps determine local and distant spread. MRI(magnetic resonance imaging) is considered the most accurate for local tumor assessment, while CT (computed tomography)and PET (positron emission tomography scan),CT are used to detect nodal and distant metastases 23,24.
Cure and Treatment of Cervical Cancer
The management of cervical cancer depends on the stage of disease, patient’s age, comorbidities, fertility desires, and overall health status. Treatment typically involves a combination of surgery, radiotherapy, chemotherapy, or targeted therapies.
1. Early-Stage Disease
2. Locally Advanced Disease
Concurrent Chemoradiotherapy (CCRT):
The gold-standard treatment for stages IIB–IVA involves external beam radiotherapy (EBRT)combined with intracavitary brachytherapy, given concurrently with cisplatin-based chemotherapy27.
3. Advanced and Recurrent Disease
Recent advances in treatment of cervical cancer
Despite progress in prevention and screening, treatment options for recurrent, persistent or metastatic cervical cancer have historically been limited. During the past few years several important advances have changed practice and expanded options for patients.
1. Immune checkpoint inhibition in advanced disease- Immune checkpoint inhibitors (ICIs) have become an established option for PD-L1–positive advanced cervical cancer. Randomized data showed that adding pembrolizumab (an anti-PD-1 antibody) to platinum-based chemotherapy (with or without bevacizumab) improved progression-free and overall survival in patients with persistent, recurrent or metastatic disease, establishing chemo-immunotherapy as a new standard in selected patients. ICIs are also being evaluated in earlier lines and in combination with radiation or targeted agents. 30,31
2. Antibody–drug conjugates (ADCs) — a new drug class with proven survival benefit Tisotumab vedotin (an ADC targeting tissue factor and carrying a cytotoxic payload) has demonstrated clinically meaningful activity in previously treated recurrent/metastatic cervical cancer and gained regulatory approval. Recent randomized data and regulatory decisions have supported its role as an option after progression on prior chemotherapy, representing the first ADC to show an overall-survival benefit in this setting. Ongoing trials are exploring combinations (e.g., ADC + ICI or ADC + chemotherapy) to increase response rates and durability.32,33
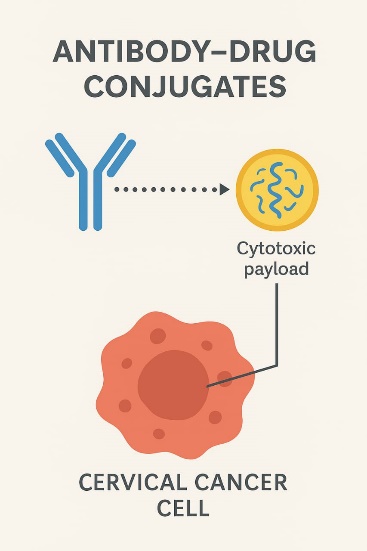
Figure 4
3. Precision/targeted approaches and biomarker-driven therapy- Molecular profiling of cervical tumors is uncovering actionable alterations in small subsets of patients (e.g., DNA damage repair gene alterations). Case reports and early studies suggest that PARP inhibitors and other targeted agents may benefit molecularly selected patients, prompting prospective trials of PARP inhibitors, tyrosine kinase inhibitors and other small molecules in genomically defined cohorts. Wider use of next-generation sequencing is enabling personalized therapy for a minority of patients.34
4. Therapeutic vaccines and novel immunotherapies- Therapeutic (non-prophylactic) vaccines directed against HPV oncoproteins (E6/E7) and combination vaccine + ICI strategies are an active area of clinical research. Early-phase trials have shown immune activation and clinical responses in premalignant lesions and some invasive cancers; larger combination studies are underway to assess whether vaccines can improve outcomes when added to standard therapies. Adoptive T-cell therapies (including engineered T-cell approaches) are also in early clinical testing for HPV-driven cancers.35
5. Improvements in multimodality care and guideline updates- Clinical practice guidelines have adapted to incorporate these new systemic options and emphasize multidisciplinary care. Better integration of systemic therapy advances (immunotherapy, ADCs, targeted agents) with contemporary radiation techniques (image-guided brachytherapy) and surgical decision algorithms has refined treatment sequencing and palliation — leading to improved disease control and quality-of-life outcomes for many patients.31,36
6. Future directions- Research priorities include rational combinations (e.g., ADC + ICI, vaccine + ICI), identification of predictive biomarkers to select patients most likely to benefit, and expanding access to clinical trials globally. The goal is to convert more durable responses into long-term control while maintaining tolerability.
CONCLUSION
Cervical cancer continues to be a significant global health concern despite being largely preventable through HPV vaccination and effective screening programs. Persistent infection with high-risk HPV types remains the central etiological factor, with additional cofactors contributing to progression from precancerous lesions to invasive disease. Early detection through cytology, HPV testing, and timely diagnostic evaluation is critical for improving survival outcomes. Treatment strategies are stage-specific, ranging from fertility-preserving surgical techniques for early-stage disease to concurrent chemoradiotherapy for locally advanced cases and systemic therapy for metastatic disease. The emergence of immune checkpoint inhibitors, antibody–drug conjugates, targeted therapies, and therapeutic vaccines has revolutionized management, offering hope for improved survival and quality of life even in advanced or recurrent settings. A multidisciplinary approach integrating prevention, early detection, and personalized treatment strategies remains the cornerstone for reducing cervical cancer incidence and mortality worldwide. Continued research and equitable access to vaccination and novel therapies will be key to achieving global cervical cancer elimination goals.
REFERENCES


Rashmi Sumbria*, Anjana Thakur, An Overview of Cervical Cancer and Its Prevention, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 2265-2273 https://doi.org/10.5281/zenodo.17165743
 10.5281/zenodo.17165743
10.5281/zenodo.17165743