School of Pharmaceutical Sciences, Vels Institute of Science, Technology and Advanced Studies (VISTAS), Chennai, Tamil Nadu, India 600117
Hypertension is a common affliction, particularly following middle age. While it is not a disease on its own, it poses a major risk factor for cardiovascular illness and death.In 1990, there were 650 million adults with hypertension; by 2019, that figure had doubled to 1.28 billion. For the treatment of hypertension, there are numerous recognized national and international guidelines. Historically, diuretics were considered the primary treatment for hypertension, but the latest guidelines from the Joint National Commission (JNC8 guidelines) now suggest that both calcium channel blockers and angiotensin-converting enzyme inhibitors should be used as first-line treatments alongside diuretics. Combinations of antihypertensive medications are typically utilized to address comorbid disorders and provide excellent long-term control. The usage of antihypertensive drugs, their economic considerations, patient treatment compliance, and doctors' adherence to prescription recommendations in various contexts, including India, are the main topics of this review. Studies on prescribing patterns for antihypertensive drugs aid in monitoring, assessing, and modifying prescribing practices as needed to provide logical and economical treatment. Furthermore, the sensible use of antihypertensive medications that may be customized to meet the needs of patients, especially those in developing nations, is aided by novel drug formulations, prescription monitoring studies, and the periodic updating of suggested recommendations.
The silent killer is a common description of hypertension. Consistently high blood pressure is a common cause of premature death, even though symptoms are typically absent. It damages several organs over time and can lead to overt cardiovascular disease, chronic kidney impairment, and stroke.[1].It is the second leading cause of chronic kidney disease (CKD).Worldwide, an estimated 1.28 billion persons between the ages of 30 and 79 suffer from hypertension; the majority (two- thirds) reside in low- and middle-income nations.[2].Clinical data showed that individuals with hypertension who took antihypertensive drugs were less likely to suffer from coronary artery disease, stroke, heart failure, revascularization, and end-stage renal diseases. [3] Increasing populations, aging populations, and behavioral risk factors like poor food, excessive alcohol consumption, sedentary lifestyles, obesity, and chronic stress have all been linked to the rising prevalence of hypertension. An astounding 9.4 million people die from hypertension each year worldwide[4],From 1990 to 2019, the global CVD death rate decreased from 354.5 deaths per 100,000 people to 239.9 deaths per 100,000 people. However, this decrease was not uniform across areas; high-income nations had the fastest drop in the death rate[5].Indian hypertension prevalence is rising quickly, according to epidemiological research, with rates ranging from 4 to 15% in urban areas and 2 to 8% in People living in rural ares[6].Clinical professionals use the various guidelines developed globally for the treatment of hypertension as benchmarks. However, a lot of doctors manage hypertension patients using their own prescription regimen based on their professional background. Primary care physicians must be trained in the proper, evidence-based treatment of hypertension. The idea of individualized, yet economical, pharmacological management of hypertension can be better understood by reviewing these prescribing patterns and the usage of anti-hypertensive medications in accordance with guidelines.
Fig 1: The Society of Hypertension in Europe A comprehensive strategy for managing hypertension.
Guidelines and medication for hypertension
The purpose of anti-hypertensive medications is to prevent, control, or treat hypertension by utilizing a variety of chemical classes..Patients frequently need more than one medication to effectively control their hypertension. It has been demonstrated that several kinds of anti-hypertensive medications, such as diuretics, rein-angiotensin system inhibitors, calcium channel blockers (CCB), and beta blockers (BB), can lessen the difficulties associated with hypertension and can be used as first-line medication[7]. Since it is widely known that hypertension needs to be better controlled, a number of classification and management guidelines have been produced. American organizations are among those that have created guidelines. The Joint National Committee (JNC) on Detection, Evaluation, and Treatment of High Blood Pressure, the Japanese Society of Hypertension, the European Society of Hypertension (ESH)/European Society of Cardiology (ESC), the National Institute for Health and Care Excellence (NICE), and the Society of Hypertension/International Society of Hypertension (ASH/ISH) are all involved. The latest recommendations for hypertension management from various clinical trials are found in the JNC 8 guidelines, issued in 2014. Following a comprehensive analysis of the information, the subsequent principles were developed to assist specialists, particularly primary care physicians. .[8]. Despite these suggestions highlighting hypertension as a significant public health issue, many specialists do not routinely monitor blood pressure and, after diagnosis, neglect to initiate treatment or properly adjust medication dosages.[9]. In all, 19,258 patients were found to have hypertension: 4,000 in the post-JNC 7 cohort and 15,258 in the pre-JNC 7 group. In the pre-JNC 7 cohort, blood pressure control was 40.8%, but in the post-JNC 7 cohort, it was 49.3% (P <.0001). Compared to the after-JNC 7 cohort, patients in the before-JNC 7 cohort had a 45% lower chance of achieving blood pressure control after adjusting for demographic and clinical factors (odds ratio, 0.551; P <.0001)[3]. According to a different, older study that examined whether the WHO/ISH (1999) and JNC 6 (1997) guidelines were being followed, 43.7% of the sample had optimal or normal blood pressure, 13.4% had high-normal blood pressure, 12.9% had stage 1 hypertension, and 30.0% had stage 2 or higher hypertension or the medication. The proportion of participants in group A fell as blood pressure levels rose, however the proportion of patients in group C soared.In risk categories A, B, and C, the proportion of people with hypertension or high-normal blood pressure was just 2.4% (all women), 59.3%, and 38.2%, respectively. According to JNC VI criteria, 39.4% of the high-normal or hypertensive group met the requirements for lifestyle change as the first intervention, and 60.6% of them were either on medication therapy or eligible to start medication therapy[10]. Jeschke et al. condition the antihypertensive medications supplied by German specialist who training complementary and alternative medicine (CAM) accord to the recommendations organized by the German Hypertension Society. Conventional antihypertensives, such as ACEIs and BBs, were used to treat the majority of patients. ACEI and a thiazide diuretic were the most commonly prescribed combo[11].
Table 1: Comparisons between goal blood pressure and first-line medication for persons with hypertension according to guidelines
|
Guideline |
Population |
Goal BP, mmHg |
Initial drug treatment options |
|
JNC8:2014 Guideline for Hypertension [3] |
General≥60y |
<150/90 |
Nonblack: ACEI, AR, CCB, or thiazide-type diuretics; black: CCB or thiazide-type diuretics |
|
General <60y |
<140/90 |
||
|
Diabetics |
<140/90 |
||
|
CKD |
<140/90 |
ACEIs (Angiotensin-Converting Enzyme Inhibitors)& ARBs (Angiotensin II Receptor Blockers) |
|
|
ESH/ESC 2013 [34] |
General non elderly |
<140/90 |
Diuretic, CCB,BB,ACEI, or ARB |
|
|
General elderly <80 y |
<150/90 |
|
|
General ≥80 y |
<150/90 |
||
|
Diabetes |
<140/85 |
ACEI or ARB |
|
|
CKD no proteinuria |
<140/90 |
||
|
CKD + proteinuria |
<130/90 |
||
|
Program for the Education of Canadian Hypertension (CHEP)) [35] |
General<80 y |
<140/90 |
ARB, ACEI (nonblack), BB (age <60 years), or thiazide
|
|
General≥80 y |
<150/90 |
||
|
Diabetes |
<130/80 |
ACEI, ARB, thiazide, or dihydropyridine CCB without an increased risk of cardiovascular disease ACEI, ARB, or ACEI with an increased risk of CVD |
|
|
|
CKD |
<140/90 |
ACEI or ARB |
|
In 2013, the American Diabetes Association (ADA)[36] |
Diabetes |
<140/80 |
ACEI or ARB |
|
Enhancing Kidney Disease Worldwide (KDIGO) 2012[37] |
CKD, no proteinuria |
≤140/90 |
ACEI or ARB |
|
CKD+ Proteinuria |
≤130/80 |
||
|
.NICE (2011) [38] |
General <80 y |
<140/90 |
<55y: ACEI or ARB |
|
General ≥80y |
<150/90 |
≥55y or black:CCB |
|
|
Blacks' International Society for Hypertension (ISHIB) 2010 [39] |
Black, lower risk |
<135/85 |
Diuretics or CCB |
|
Target organ damage or CVD risk |
<130/80 |
||
|
Hypertension Management Guidelines, Korean Society of Hypertension, 2013 [40] |
Elderly(<65 years) |
140/90 |
ACEIs, CCBs, and diuretics; BBs ought to be reserved for certain situations. |
|
Diabetes |
<140/85 |
||
|
Stroke, CAD and CKD |
140/90 |
Combine therapy with diuretics, CCBs, and ARBs |
Evaluation of prescription trends for antihypertensive drugs
Numerous studies have assessed the global prescription trends for antihypertensive medications. Over the past 20 years, the usage of ACEIs, ARBs, and CCBs has steadily expanded, and numerous thorough clinical trials have revealed no appreciable variations in the antihypertensive efficacy, adverse effects, or quality of life of these medication classes[12]. In their study, Avinash Janardan Pujari and Rahul V. Kedare found that most of the participants were prescribed monotherapy first, then two medications. A handful of others needed three or more medications. The most often recommended medications in combination therapy were diuretics, but ACEIs were the most often prescribed medications in monotherapy. Researchers also found that most patients did not reach target blood pressure management, suggesting that monotherapy may not be enough to achieve optimal blood pressure control in most people[13] Maryam Salem Alkaabi evaluated 588 people with hypertension. Antihypertensive medications were taken by most patients in two-drug combinations (n = 210, 35.5%) after monotherapy (n = 188, 32.1%) and three-drug combinations (n = 136, 23.1%). The most frequently prescribed class for both solo and combination therapy was calcium channel blockers (51%), although the most typically given drugs for monotherapy were angiotensin receptor blockers and angiotensin-converting enzyme inhibitors (55.9%). The results indicated that, whether used alone or in combination, amlodipine was the most often prescribed antihypertensive medication (266 prescriptions)[14]. A cross-sectional study on tertiary hospitals was carried out by Rajeev Mishra and Priyanka Kesarwani. 34.8% of patients in the current study received combination therapy, whereas 65.2% of patients received monotherapy. The most often given combination medication was angiotensin receptor blockers (ARBs) + diuretics, and Calcium channel blockers (CCBs) were the monotherapy that was most commonly prescribed[15]. In Ethiopia, 423 patients participated in a randomly selected study in south zone Gondar hospitals to examine the antihypertensive medication prescription trend. The average percentage that met WHO criteria was 93.5%. Monotherapies made up over 53% of all prescriptions for hypertension. Diuretics were the most commonly recommended medication, both alone and in combination with calcium channel blockers (CCBs) as dual treatment, according to a study[16] In a National Health and Nutrition Examination Survey of people aged ≥18, combination treatment plans were found to assist reach blood pressure targets. Single-pill fixed dose combination (FDC) and multiple-pill combinations were associated with a 55% and 26% higher chance of blood pressure management, respectively, compared to monotherapy. The percentage of those using specific antihypertensive drugs increased from 36.8% to 47.7% (p<0.01), with thiazide diuretics, BBs, ACEIs, and ARBs being used at rates of 23%, 57%, 31%, and 100%, respectively[17]. Table 2. As far as we know, there isn't any recent information on how antihypertensive medication prescriptions vary among countries, which would enable doctors to stay abreast of current developments.
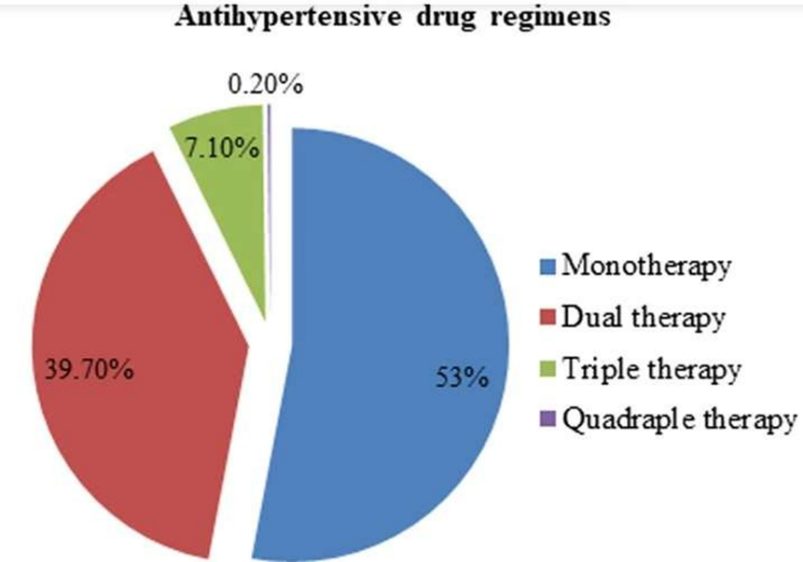
Fig :2 Antihypertensive drug regimen
Table 2 Results from several investigations was out to assess the prescribing practices of antihypertensive medications
|
Author name |
No. subjects involved |
Mono- /combination therapy prescribed |
Antihypertensive drug class |
Observation/Remarks |
|
Caceres et al[12]. |
100 % of the Extremadura population |
Monotherapy |
ARBs, ACEIs |
ARBs use increased compared to ACEI use |
|
Kedare, R. K., Pujari et al [13]. |
240 Patients |
Two or more |
ARBs, CCB, Diuretics, ACEIs |
Monthly consultations and twice-daily dosage were linked to fewer cases of uncontrolled blood pressure. |
|
Maryam Salem Alkaabi et al[14]. |
588 Patients |
Monotherapy |
CCB, ARBs, ACEIs |
Amlodipine was the most often prescribed medication, irrespective of if it was used alone or in combination. |
|
Rajeev Mishra et al[15]. |
128 Prescriptions |
Monotherapy and combination therapy |
CCB, ARBs, ACEIs |
The most often prescribed antihypertensive medications were discovered to be CCBs, with ARBs coming in second in monotherapy. |
|
Taklo Simeneh Yazie et al[16] |
423 Prescriptions |
Monotherapy and combination therapy |
Diuretics, CCB |
90% of prescriptions followed WHO guidelines. |
Cost outcomes of antihypertensive prescription drugs
An efficient course of treatment has always been hampered by the expense of pharmaceuticals. The rising incidence of hypertension and the steadily rising cost of treating it have an impact on how doctors prescribe and how well patients adhere to their treatment plans. Patients in developing nations like India pay for their medical care out of pocket because they are not covered by insurance plans, in contrast to industrialized nations.As a result, they would gain from doctors offering better services that are founded on sensible and economical medication prescriptions[18]. Therefore, there is a significant chance that pharmacotherapy for hypertension will result in cost reductions. Pharmacoeconomic evaluations of antihypertensive medication treatments, their prices, and the associated savings in medical expenses provide a helpful framework for improving the methods used to treat hypertension today. [19]. Alpha-blockers were the most costly drug used annually, according to a cost analysis study by Rachana et al., followed by ACEIs, ARBs, CCBs, BBs, and diuretics in that order.[20].In the same way, Marta Ku?an et al. observed that the most economical medications for hypertension were diuretics[21]. Notably, following recommendations while prescribing antihypertensive medications leads to significant prescription expense savings.[22].

Fig:3 Cost-Effectiveness of Medication for Patients with Hypertension
In the 2017 ACC/AHA guidelines, drug treatment is advised for stage I hypertension individuals (SBP/DBP: 130-139/80-89 mm Hg) who are 265 years of age and free of cardiovascular disease; however, this recommendation is not included in the 2018 Chinese guidelines.Fig: 2 According to Paudel, the most economical class of antihypertensive medications was calcium channel blockers. Hypertensive individuals in all four groups incurred significant costs due to direct medical expenses[23]. Furthermore, the price for medications differed by hospital type (private or public), per a study by Rimoy et al. that discovered the cost of Furosemide, Bendroflumethiazide, and nifedipine in private hospitals were approximately five to six times higher than those in government-owned pharmacies. [24].Comorbid conditions exacerbate the issue of a greater financial load. According to a Markov model, ARB plus CCB combination therapy is a more economical lifelong antihypertensive approach in Japan for individuals with essential hypertension than either drug alone[25].
The conclusions about the cost implications from the aforementioned investigations are compiled in Table 3.
|
Author Name |
Number of subjects involved |
Mono-/combination therapy prescribed |
Observation/Remarks |
|
Rachana et al [20]. |
300 prescriptions |
Mono (48.94 %), CCB |
Costliest - Alpha-blocker |
|
Cost effective - Diuretic |
|||
|
Marta kucan et al [21]. |
2 Patients (Markov model) |
angiotensin converting enzyme inhibitors/angiotensin- II receptor blockers (A) |
Cost effective -Diuretic |
|
Fisher and Avorn et al [22]. |
133,624 patients |
Combination (CCB + ACEI) |
Following the guidelines leads to savings |
|
Sabita Paudel et |
20-69 age patients |
CCB, Diuretics, |
Cost effective/ High –CCB + ARB |
Antihypertensive medication uses and adherence
Studies in various contexts have examined the use of antihypertensive drugs, patient adherence to therapy, and doctors' adherence to prescription recommendations. Several of them have reported complete, partial, or nonexistent adherence in certain investigations. According to studies, guidelines should be developed that adapt treatment methods that require less regular physician monitoring to patients in underdeveloped nations. Every advice in the world stresses that doctors must use a patient-centric approach and that they are only intended to be used as guidelines. In order to reach as many patients as possible, treatment plans in developing countries with access to healthcare systems is less developed than in developed countries should be simple to reasonably, inexpensive, and require time-bound titration by primary care physicians rather than specialists or tertiary care physicians. An Indian investigation revealed a common pattern: the study participants were taking at least two antihypertensives as part of several therapy. Guidelines advise as this pattern advised since moderate doses of various antihypertensive medication classes are advantageous to high doses of one.[26]. Latest research found that excellent adherence to antihypertensive treatment was associated with exercise, concomitant medication, and various types of hypertension medications, whereas poor adherence was associated with a high salt intake. These factors should be considered in order to better control hypertension.[27].Odili et al. investigated how doctors manage hypertension generally and how well they follow JNC 7, WHO/ISH, and ESH guidelines. They came to the conclusion that doctors in this study complied with the standards for managing hypertension fairly. But they didn't seem to advise their patients to change their lifestyles[28]. According to the results of another study by Luca Degli Esposti, a significant percentage of patients had unsatisfactory adherence to AHT, which is linked to negative health outcomes in the primary prevention of CV disorders. This early data highlights the necessity of tracking and enhancing drug adherence in clinical practice for health authorities[29].As assessed by the MMAS-8, co-morbidity, alcohol consumption, drug self-purchase, and the mix of antihypertensive medications were found to influence the unsatisfactory adherence level to the prescribed antihypertensive medications[30]. Even though doctors self-reported that they were aware of and adhered to the hypertension recommendations in their daily practice, a multicenter study revealed a significantly lower agreement rate between physicians' practices and European standards. Furthermore, it was shown that almost 40% of low-risk patients received medications that were not recommended, more than one-fourth of high-risk hypertension patients stay untreated, and half of them remain uncontrolled [31]. Interestingly, According to this large cohort study, diuretics had the lowest 2-year adherence and persistence rates among antihypertensives. Compared to products containing just one drug, fixed-dose combos with diuretics may make adherence easier. Regardless of medication class, however, there is a need for efficient methods to increase adherence to antihypertensives[32]. Table 4 enumerates the findings of the investigations mentioned above. Clinical trials on treatment compliance for hypertension showed that compliance rates were adequate when using monotherapy, mediocre when using two different medications (pills), and poor when using more than two pills. It should be noted that medical professionals seemed to be aware of these trials. They switched from monotherapy to single-pill FDC as a result. This method will offset the adverse effects of the maximal dosage of a single drug class while also attracting the synergistic effects of many drug classes at low dosages. The single tablet FDC has the added advantage of being less expensive than several pills of various drug classes, in addition to better compliance.
Table 4: Findings from various research emphasizing the use of antihypertensive medications and adherence
|
Author Name |
Number of Patients |
Observation/Remarks |
|
Xavier et al [25]. |
380 patients |
Several antihypertensive medication groups work better in small doses than in large dosages. |
|
Hyo Yoon Choi et al [26]. |
1,523 patients |
Medication adherence lower among patients regularly consumed amounts of salt. |
|
Odili et al [27]. |
501 case notes |
Fair adherence to the rules as indicated |
|
Luca Degli Esposti et al [19]. |
105,512 patients |
Poor AHT adherence is widespread and has a detrimental effect on primary CV disease prevention, highlighting the need for improved clinical practice and better monitoring. |
|
Solomon Weldegebreal Asgedom et al[29]. |
280 patients |
Medication combinations, alcohol consumption, comorbidities, and self- purchasing all contributed to suboptimal adherence to antihypertensive medications. |
CONCULSION
Special consideration must still be given to the ongoing difficulties in managing hypertension. The management of hypertension has been outlined in several national and international guidelines that emphasize either monotherapy or combination therapy based on blood pressure levels and related comorbidities. Treatment strategies for hypertension have evolved over time, moving from diuretics to ACEI/ARB/CCB as the primary medication of choice, and from monotherapy to low dose combination single pill therapy. If national health policy makers wish to reduce the morbidity and mortality rates from hypertension, they should consider of the analysis and treatment of hypertension as a right in the public health system. Doctors are often forced to customize therapy based on the individual characteristics of each patient and how they respond to treatment because there are still differences in treatment techniques despite these facts and established guidelines.
More detailed research is needed in developing nations like India to analyze prescribing patterns and the adoption of guidelines-based antihypertensive medications that can be adjusted to match the needs of individual patients.
REFERENCES


S. Harrish Raj, J. Kabilan, A. Bestiya Benedict, An Overview of Recent Studies on The Prescribing Pattern of Antihypertensive Medications, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 186-197. https://doi.org/10.5281/zenodo.15788069
 10.5281/zenodo.15788069
10.5281/zenodo.15788069
