
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Swamy Vivekanandha College of Pharmacy, Namakkal, Tamil Nadu, India 637205
Anosmia the loss of smell-impacts quality of life significantly in terms of nutrition, safety, and emotional well-being. Olfaction is a complex chemosensory process involved in several activities of daily living, from the detection of environmental threats to enhanced enjoyment of food and social interplays. This review studies the epidemiology, prevalence, and physiological mechanisms related to olfactory dysfunction, including functions of olfactory neurons and neurogenesis. Anosmia with respect to aging, neurodegenerative diseases, viral infections, and environmental factors often indicates its clinical importance. To address this, psychophysical, electrophysiological, imaging, and biochemical studies are performed in order to assess olfactory function. Although emerging research has increased, gaps still remain in the treatment and management of anosmia. Future directions emphasize neuroplasticity, olfactory training, biomarker discovery, genetic therapies, and the psychosocial impact of anosmia. Understanding anosmia as an early sign for neurodegenerative diseases allows for enhanced diagnostic and therapeutic approaches, providing substance for interdisciplinary research on olfactory dysfunction.
Few individuals deliberately appreciate the extend of data given by the sense of scent, from identifying caution destructive odors from the environment to shaping a major portion of numerous of life's pleasurable encounters, whether eating a feast, a walk within the wide open, or closeness with one's accomplice. Consequently, failure to scent or losing the sense of smell—anosmia—can have a serious affect on wellbeing and quality of life.Normosmia is the typical sense of scent. Chemosensory brokenness includes scent, taste, and chemesthesis clutters (1). The misfortune of the faculties of smell (anosmia) are the foremost common chemosensory brokenness, and the diminished capacity to scent (hyposmia) are too common. This case definition will center on the misfortune of olfactory work (anosmia) (2). Scent and taste are specialized tangible visceral faculties that have a place to chemoreceptors and empower acknowledgment of the world in various ways . Quickly after birth, the child recognizes its mother by the sense of smell. Scent could be a common work that's performed unnoticed and ceaselessly, it is comparative to gulping, breathing, flickering, activities that happen ceaselessly without cognizant exertion. The preparing of the olfactory sensation incorporates the location, recognition, separation and distinguishing proof of odors . Effective messages can be conveyed by scent by pheromones, odors that are particular for the creature species and through a exceedingly specialized and practically coordinates olfactory framework; it is conceivable for imperative exercises to be performed within the creature world for the reason of survival, nutrition, propagation, etc. Within the human population, of all the five faculties, scent is the foremost energizing and slightest caught on or “forgotten” first cranial nerve or n.olfactorius. The olfactory framework is portrayed as the foremost primitive, and the physiological centrality of odor is minimized within the recognizable proof of natural factors and potential dangers. Due to early phylogenetic improvement and synchronous inclusion of various and most seasoned and subliminal brain structures within the handling of olfactory sensations (without a various leveled organization), the olfactory framework is particular and contrasts from other tangible systems (3).
EPIDEMIOLOGY AND PREVALENCE:
Anosmia-an impaired sense of smell-is a sensory disorder dependent on various other factors such as age, medical conditions, exposure to the environment, and genetics(4). About 50% of people aged 65 and older have olfactory dysfunction, with anosmia being the first clinical sign in 70 to 90% of those with neurodegenerative diseases like Parkinson's or Alzheimer's. The emergence of post-viral anosmia after infections with, for example, influenza and COVID-19 has caused a surge in interest worldwide, with a sizeable fraction of patients affected(5). Head trauma causes 5 to 20% of it, and environmental factors such as smoking and pollution also play a role. Congenital anosmia is rare but recognized since it is caused by genetic disorders like Kallmann syndrome. Studies estimate that about 20% of the general populace has some form of olfactory dysfunction and about 3 to 5% complete anosmia. The incidence of this disorder increases with age, at 25% of ages 50 to 60 and almost half at ages 65 and older. Some studies say that in cases of COVID-19, 40 to 80% of infected individuals had temporary or long-term olfactory dysfunction. The burden of anosmia underscores the need for new diagnostic, preventive, and treatment strategies(6).
IMPACT OF ANOSMIA ON QUALITY OF LIFE :
Anosmia, or olfactory dysfunction, significantly impacts the daily living of the individuals at stake by affecting their nutritional needs, safety, and mental well-being or quality of life. Loss of pleasure in eating leads to alterations in eating behavior, poor appetite, and vulnerability to malnutrition. Some 56% of anosmic respondents report a decreased appetite, while 70% report a loss of pleasure in eating, more frequently than not accompanied with weight changes(7).Other attentions devoted to the safety of patients with anosmia are within them as they might not be able to perceive some dangerous odors, like smoke in the event of a fire or gas leaks. They may even be in danger of eating spoiled food since 75% are in fear of consuming spoiled food and 61% are anxious about the undetected gas leak. Anosmia is also a component in the distress of unaddressed psychological issues: the symptomatology of depression in almost 29% of those affected along with the increased anxiety regarding one's own body odor and hygiene compromising self-esteem and complicating social interactions(8).
ANATOMY AND PHYSIOLOGY OF OLFACTION:
The olfactory system is a highly specialized sensory system responsible for first recognizing, encoding, and then interpreting odor molecules. It begins with the olfactory epithelium found in the upper nasal cavity, where the olfactory receptor neurons or ORNs, with their sensory cilia, detect odor molecules dissolved in air(9). Besides the olfactory receptor neurons, sustentacular cells and Bowman glands support the olfactory environment. When an odorant binds to its receptor, a signal passes up through the olfactory nerve, a mellifluous anatomical-tuctum known as the Cranial nerve I, through the cribriform plate into the olfactory bulb, where the glomeruli, mitral, and tufted cells process and refine input(10).Emerging from each bulb is the olfactory tract-that information has to go to the piriform cortex (observation of the smell), amygdala (for emotional processing), hippocampus (for integrating memories), and higher-in-the-group orbitofrontal cortex (for higher-order processing of smell)(11). The olfactory system bypasses the thalamus and therefore is closely associated with emotion and memory. Olfactory receptor neurons, G-protein-coupled receptors (GPCRs), work in conjunction with a signal transduction cascade involving loss of receptor neurons-specific feature-G-proteinied adenylate to form one giant cAMP pathway for neuronal activation and therefore action. Already invisible, the olfactory system has eternal neurogenesis, reconstructing receptor. But dysfunction due to aging, infections, a neurodegenerative disorder causing a mishap can lead to anosmia-a loss of ability to smell-or to hyposmia, a reduction in the sensitivity to smell, with accompanying sensory and emotional consequences(12).
MECHANISM OF ODOR DETECTION AND PROCESSING:
Anosmia (the absolute loss of the sense of smell), is a result of impairment in the complex olfactory pathway that begins in the nasal cavity and terminates in higher order brain regions involved in the perception of odor. During normal physiological conditions, olfactory sensory neurons (OSNs) contained in the olfactory epithelium at the roof of the nasal cavity, which express olfactory receptors (ORs) on their cilia, detect vapour-phase odorants in inhaled air. Once an odorant binds to its specific OR, the receptor activates olfactory specific G-protein subunit Gα-olf, stimulating adenylyl cyclase III (ACIII) to convert ATP into cyclic AMP (cAMP). cAMP opening cyclic nucleotide gated (CNG) channels allowing sodium (Na?) and calcium (Ca²?) ions to enter the neuron causing membrane depolarization and the generation of the action potential. This electrical signal travels along the OSN's axons to synapse on mitral and tufted cells in the olfactory bulb (OB), where the OSNs that express the same OR converge on glomeruli. The OB employs higher order neuronal circuits involving the mitral and tufted cells to relay the excitatory signal appropriately to the brain including the olfactory cortex. In anosmia, this pathway that is normally finely-tuned can be disrupted in multiple ways. The peripheral causes could involve only peripheral damage or peripheral functional impairment of the olfactory epithelium from viral infections (i.e., SARS-CoV-2), chronic inflammation (as with rhinosinusitis), exposure to toxic chemicals, or trauma to the nasal cavity(13). The damage that can occur via these mechanisms can ranges from altered morphology to apoptosis of olfactory sensory neurons (OSNs) or impairment of the olfactory receptors (ORs) that prevent the initiation of the olfactory signal. The olfactory signal may also be halted via the discovery of genetic mutations impairing structure and function of ORs, G-proteins (Gα-olf), ACIII, or ion channels (notably the cGMP-gated nonselective cation channels (CNG channels)). Central causes constructing anosmia are primarily injures of the olfactory bulb, olfactory tract, or further cortical areas due to trauma (e.g. head trauma), neurodegenerative disease (e.g. Alzheimer’s or Parkinson’s disease), or tumors abutting olfactory structures and centers. Lastly, there are occasions in which desensitization and adaptation within the normally functioning olfactory system were disrupted from an improper cyclase subscription (e.g. excessive degradation via phosphodiesterases (PDE), phosphorylation of the receptor via GPCR kinases (GRK), and abnormally high β-arrestin binding) which can all lead to prolonged desensitization and efficacy of the receptor. In situations, such as post-viral anosmia, a germ has the potential to impinge on the olfactory epithelium either by virtue of inflammation indirectly preventing odorant access, or direct invasion and necrosis of sustentacular cells and neurons. Even in instances where the neurons are left intact, prolonged inflammation can prevent neurogenesis, arresting the replacement of OSNs and subsequently cause prolonged or permanent anosmia. Furthermore, there can also be age-on-age degeneration of the olfactory epithelium and olfactory pathways central to processing olfactory information that progressively degrade the central nervous system's (CNS) ability to process syntactically specific odor information. The olfactory system is unlike other sensory systems as it bypasses thalamic pathways that projects to limbic structures. In this manner, the loss of olfaction (anosmia) can significantly impair quality of life, appetite, emotional state, and memory. Anosmia is fundamentally a collapse in the sensory-to-neural conversion, transmission, or processing of odor information, and the mechanisms may differ based upon the type of insult, ranging from reversible inflammation to irreversible neuronal loss. (14).
ROLE OF OLFACTORY NEURONS AND NEUROGENESIS:
Olfactory neurons are responsible for the detection and transmission of odor signals to several brain regions. Continuous neurogenesis is needed in these neurons to keep their function at peak performance. They arise from the olfactory epithelium, where they express specific receptors needed for capturing odorant molecules and allowing the transmission of activity to the olfactory bulb. There, they synapse with glomeruli and further process sensory information in parallel streams within the bulb itself. Neurogenesis in the adult olfactory system originates in the subventricular zone (SVZ), where interneurons-granule and periglomerular cells-are produced (15). They migrate through the rostral migratory stream (RMS) to incorporate themselves into circuits already in place for the purposes of odor discrimination and odor adaptation. This process is modulated by the input of information through sensory experience; neurogenesis is enhanced by odor exposure and suppressed by sensory deprivation. Disruption is brought about from aging and neurodegenerative diseases or environmental-based challenges yielding in a disorder called anosmia or the losing of one's sense of smell. Stimulation of the sensory sensation seems to support the survival of neurons while the lack of stimulation appears to contribute to olfactory dysfunction. Since olfaction is closely bound up with memory and emotion, impaired neurogenesis may also have cascading effects on cognition and psychological well-being (16).
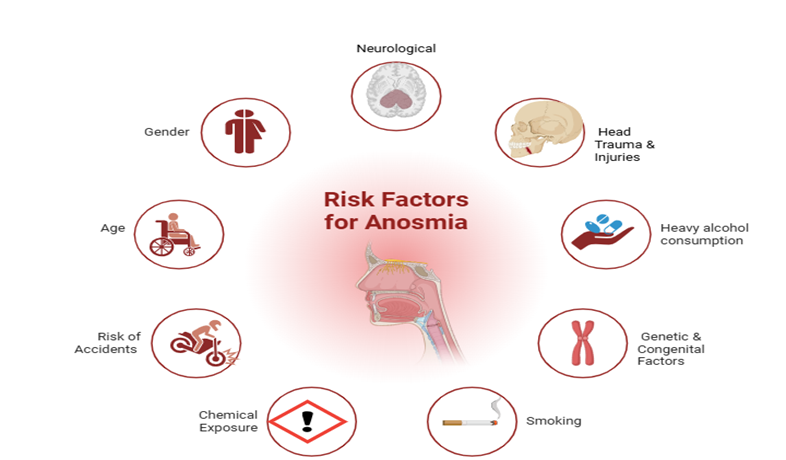
Figure:1 Risk factor for Anosmia
SYMPTOMS:
The inability to detect odors causes the affected individual much trouble in daily life. Anosmics frequently complain that they cannot taste their food, since taste is intimately tied to smell. A person with anosmia then will have a diminished appetite and weight loss as a result. Also, anosmics cannot detect dangerous odors, such as those from smoke, a gas leak, or spoiled food, that would compromise their safety. The loss of sensory enjoyment in eating and environmental stimuli has led some persons to other emotional disturbances such as anxiety and depression, together with withdrawal from social activities. In some cases, these patients also experience concomitant conditions such as parosmia (distorted smell perception) or phantosmia (smell perception in the absence of an external stimulus), which could result in it being more debilitating to one's overall quality of life?(17).
DIAGNOSTIC TESTS:
The diagnostic tests for anosmia include an assessment of olfactory function: psychophysical, electrophysiological, imaging, and biochemical tests. Psychophysical tests, to illustrate this, include: the Sniffin' Sticks Test, the University of Pennsylvania Smell Identification Test and the Connecticut Chemosensory Clinical Research Center Test, respectively for the detection, identification and characterization of odor. The other set of tests is based on some electrophysiological methods. These are as follows: the Olfactory Event-Related Potentials and Electro-olfactogram tests that target the extent of neural activity in response to any odor stimulus. They help differentiate between real anosmia and its psychogenic cases (18).Such imaging studies includeMRI, CT and PET scans, which generally detect structural abnormalities including atrophy of the olfactory bulb, sinus disease or neurodegeneration. Diagnosing anosmia due to neurodegenerative conditions- for example, Kallmann's syndrome- can be enhanced with the use of biochemical and genetic testing like olfactory mucosa biopsy and genetic testing in some cases of enjoyment-induced anosmia- such as COVID-19- in which the area of interest is confirmed through the use of CCCRC with additional testing for gustatory function. These allow confirmation of anosmia with the application of differential diagnosis in order to guide treatment (19).
FUTURE DIRECTIONS AND RESEARCH GAPS:
There exist, however, certain important research gaps concerning anosmia that still warrant exploration related to its diagnosis, treatment, and management. One area of promise involves neuroplasticity and olfactory training, which evaluate the potential for long-term olfactory rehabilitation to promote regeneration and functional recovery at the neural level. Though initial observations support potential efficacy, longitudinal studies are necessary in order to verify long-term results that aspire to implement such training into their programs, especially for post-viral and neurodegenerative cases. Biomarker discovery remains critical in distinguishing and predicting recovery from diverse types of anosmia, especially in the case of Alzheimer’s and Parkinson’s diseases, where abnormalities in the sense of smell often predate clinical characteristics (20). Therefore, advanced imaging strategies, such as high-resolution MRI and PET, must be used to detect early olfactory impairments and identify structural changes. Additionally, recognizing the genetic and molecular architecture of anosmia might provide the rationale for specific therapies that encompass gene or stem cell therapies, even if these are still in their early cousin development phases. Specific investigations focusing on the impacts of viral infections, notably COVID-19, would pay off in regard to their relevant findings about ongoing olfactory loss mechanisms and possible avenues for treating recovery. Underappreciated are the roles of environmental pollution and lifestyle in causing olfactory impairment; thus, large epidemiological studies are desperately warranted (21). Clinical trials on activity mobilization-taking aim at olfactory receptor neurons and central pathways-should, therefore, be organized to establish efficacy moving forward.Beyond purely biological aspects surrounding anosmia, its psychosocial underpinning requires even greater attention. Anosmia presents mental health, nutrition, and quality-of-life challenges that fuel depression and anxiety. Hence, one must engage in comprehensive management approaches that amalgamate avenues from psychological support to sensory rehabilitation. Future studies also ought to investigate the utility of anosmia as an early marker of tardive neurodegenerative pathway disorders. If olfactory deficits turn out to be a reliable early signal of such disorders, then they may well be introduced as routine assessments to contribute greatly to early diagnosis and intervention. It would be critical to engage into a multidisciplinary approach involving neurology, genetics, imaging, and pharmacology in order to fill the gaps in current research about the characterization, diagnosis, and treatment of anosmia (22).
CONCLUSION:
Anosmia is a multi-faceted sensory disorder not greatly documented and mostly neglected but with a major impact on daily living and general health. It is caused by a myriad of both neurodegenerative conditions and infections, the environment bearing the brunt. Reduction in olfaction actually means great losses in detection of odors together with other far-reaching impacts touching on nutrition, emotional well-being, and safety. While improved diagnostic methods and ongoing research into various treatment strategies-from olfactory training to regenerative medicine-are present, considerable research gaps have existed concerning the pathology and long-term management of the condition. Future research, therefore, needs to fill the gaps-by advancing early diagnosis, targeted therapy, and psychosocial considerations-into designing the concept of multi-functional therapy. Bridging such gaps would certainly be paramount in relieving the burden of olfactometry dysfunction, therefore improving inpatient care.
AUTHOR CONTRIBUTIONS: All authors have contributed equally and substantially.
FUNDING: No funding.
CONFLICT OF INTEREST: The author declares no conflict of interest. The manuscript has not been submitted for publication in any other journal.
ETHICS APPROVAL: Not applicable.
AI TOOL DECLARATION: No AI and associated tools are used for writing scientific content in the article.
REFERENCES


Sudhakar Pachiappan, Sneha Sekar, Gayathiri Muthusamy, Sabarinath Chandrasekar, Akshaya Sivakumar, Gayathridevi Senthilkumar, Parkavi Gopalakrishnan, Thendral Jothilingam, Anosmia and Olfactory Dysfunction: Insights into Neurological and Sensory Disorders, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 2033-2040. https://doi.org/10.5281/zenodo.15913922
 10.5281/zenodo.15913922
10.5281/zenodo.15913922