
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Priyadarshini J. L. College of Pharmacy, Nagpur, 440016 Maharashtra India.
Topical drug delivery for inflammatory conditions has advanced considerably with the introduction of emulgel formulations. Emulgels, which combine the beneficial properties of emulsions and gels, provide improved drug stability, enhanced skin penetration, and user-friendly application. This review presents a detailed overview of current developments in anti-inflammatory emulgels, covering formulation techniques, underlying mechanisms, and evaluation methods. It emphasizes the benefits of emulgels compared to traditional topical dosage forms, particularly their capacity to efficiently deliver both water- and oil-soluble drugs. However, challenges such as maintaining formulation stability, controlling drug release, and ensuring skin compatibility persist. The review also discusses future directions, including the use of novel excipients, incorporation of nanotechnology, and personalized treatment strategies to enhance therapeutic efficacy. By summarizing existing research and highlighting areas needing further study, this article serves as a comprehensive guide for researchers developing advanced topical anti-inflammatory treatments.
When other methods of drug administration fail or for skin conditions, the topical drug delivery system is the dose form that is applied to the skin. One benefit of the topical medication delivery method is its ability to bypass the first-pass metabolism. Additionally, it assists in avoiding the danger and inconvenience of intravenous route therapy. Anywhere in the body, topical medication administration is the most straightforward method of localized drug delivery via the skin, vagina, rectal, and ocular channels. These are used on both healthy and damaged skin as a variety of preparations for dermatological and cosmetic purposes. [1] The skin covers the majority of the body and is the main channel of administration for the local drug delivery system, as well as one of the most accessible organs for topical application. [2] Various drug delivery systems, including nanoparticles, nanoemulsions, nanosuspensions, nanosomes, nanofibers, and nanosponges, have been developed in nanotechnology to reduce side effects and transport the medicine to the target site in a regulated and predictable manner.nanofibers, and nanosponges, have been developed in nanotechnology to reduce side effects and transport the medicine to the target site in a regulated and predictable manner.
TOPICAL DRUG DELIVERY SYSTEM
The topical delivery system's primary benefit is its ability to avoid first-pass metabolism. Another benefit is avoiding the dangers and drawbacks of intravenous therapy, as well as the various conditions of absorption, such as pH fluctuations, the presence of enzymes, and gastric emptying time. When alternative drug administration methods are ineffective, the topical drug delivery method is typically employed. Additionally, research is being conducted to reduce the hazards and inconveniences associated with intravenous therapy and absorption-related issues such as pH fluctuations, enzymatic activity, and gastric emptying time.The simplest and most straightforward method is topical medication administration [1]. For both local and systemic disorders, topical medication delivery is a popular therapeutic approach. The medication is absorbed by the skin and reaches the site of action in the topical delivery system to produce a therapeutic effect [3]. The physiological characteristics of the carrier directly affect the rate of drug release from a topical preparation [4]. Emulsions, creams, ointments, lotions, powders, and other topical delivery forms are commonly used to treat skin-related conditions [4,5]. Topical formulations can be categorized based on their textures, including solid, liquid, semi-solid, and other formulations [6]. Three mechanisms—transcellular, intercellular, and follicular—are used to absorb topical drugs. The medications use passive diffusion to enter the stratum corneum [7]. Diffusion and dissolution are the rate-limiting processes. Three different formulations of topical medications are used: transdermal, endodermal, and epidermal. The quickest and most straightforward method is the transcellular mechanism. The typical method is the intercellular mechanism, while sweat glands and hair follicles are used in the follicular mechanism [8].
STRUCTURE OF SKIN
The primary structural element of the human body, skin makes up around 15% of an adult's total body weight [9]. This demonstrates its large surface area and critical functions in temperature regulation, environmental sensing, and internal organ protection. This broad coverage is essential for sensation, control, and defense [10]. By limiting excessive water loss, regulating body temperature to maintain optimal levels, and serving as a barrier against various substances, biological agents, and physical hazards, the skin helps keep the body hydrated. These processes ensure that the body remains balanced and protected from external threats, which is crucial for preserving overall health and well-being [11]. The skin of an adult provides a significant protective barrier, covering approximately 2 m² [3]. Due to the acids produced by sebum and sweat, which support skin health, its pH is typically low [12].
Skin consists of following layers
Epidermis consists of following layers
2. Dermis
The dermis, which forms the inner layer of the skin, lies between the basement membrane and the deeper layer of fat and tissue. It is between 1 and 5 mm thick—much thicker than the epidermis. Its primary function is to nourish and support the epidermis. The dermis consists of two layers of connective tissue—the papillary and reticular layers—which blend together to provide the skin with elasticity and structural integrity. This layered framework also contains blood vessels, nerves, and other vital components essential for maintaining skin health and function [18].
The uppermost portion, known as the papillary layer, is made of loose connective tissue and is thinner than the epidermis. Beneath it lies the reticular layer, which is thicker, denser, and less cellular. It is primarily composed of dense connective tissue with bundles of collagen fibers, contributing significantly to the skin’s strength and resilience [19].
3. Hypodermis
The hypodermis, which lies beneath the dermis, is primarily composed of connective and adipose tissue. This layer provides the skin with support, cushioning, and insulation while connecting it to underlying structures such as muscles and bones. Also known as the subcutaneous fascia, it functions as an insulating layer, cushion, and energy store. The hypodermis is essential for maintaining skin integrity, regulating body temperature, and enhancing the overall structure and function of the skin [20]. It is the deepest layer of the skin and contains, among other skin appendages, blood vessels, sensory neurons, and hair follicles [21].

Fig 1. Structure of skin
OVERVIEW ON EMULGEL
A specific topical formulation known as an emulgel is made by mixing an emulsion with a gel base. It is crucial for topical medication administration because of its dual release mechanism, which combines gel and emulsion systems [22]. These emulgels have several desirable qualities for dermatological applications, such as a non-greasy texture, ease of spreadability and removal, emollient properties, non-staining qualities, longer shelf life, transparency, attractive appearance, and a lower chance of serious side effects [23]. A gelling agent can stabilize an emulgel made as either water dispersed in oil (w/o) or oil dispersed in water (o/w). It provides a reliable and efficient platform for incorporating drugs that are poorly soluble in water [24]. Emulgel can handle both lipophilic and hydrophilic drugs because of its dual aqueous and non-aqueous phases. By using a biphasic approach to increase drug loading capacity and stability, it also serves as a controlled-release formulation [25]. It functions as a dual-controlled release mechanism, combining the advantageous qualities of emulsions and gels for improved efficacy and delivery [26]. Emulgels are emulsions—either water-in-oil or oil-in-water—that gel upon contact with a gelling agent [27]. Emulsified gels are superior and stable carriers for hydrophobic or poorly water-soluble drugs. Emulsion and gel are combined to create short emulgels [28]. One of the key limitations of gels’ many benefits is their reduced capacity for administering hydrophobic drugs [29].
Delivery of Drug Through Emulgel
By encapsulating drug particles in their internal phase, emulsions serve as controlled-release drug delivery systems that ensure a steady and gradual release of the medication. This configuration allows the drug to slowly permeate the skin and diffuse through the emulsion’s outer layer, resulting in prolonged release that enhances the drug’s efficacy by promoting gradual and sustained absorption. A cross-linked gel network effectively traps small particles and supports regulated drug release, ensuring a consistent supply of the active ingredient over time. Furthermore, the mucoadhesive properties of these formulations extend the duration the drug remains in contact with the skin, further improving therapeutic outcomes. The emollient properties of water-in-oil emulsions make them particularly suitable for treating dry skin disorders [30].
Bottom of Form
Types of Emulgel
Microemulsion Gel [31]
A microemulsion gel is a biphasic oil-in-water formulation stabilized by surfactants, offering optical clarity and thermodynamic stability. The droplets, ranging in size from 10 to 100 μm, are composed of precise proportions of water, surfactant, co-surfactant, and oil. Microemulsions are characterized by high surface area, low interfacial tension, and the ability to dissolve both water- and oil-soluble substances. These properties enhance drug penetration by reducing the stratum corneum's barrier, making them beneficial for transdermal drug delivery. To address the challenge of viscosity and stability, gelling agents such as Guar gum, HPMC K100M, and Carbopol 940 are incorporated into microemulsions to form microemulsion-based gels.
Nanoemulsion Gels [32]
Nanoemulsion gels are clear oil-in-water dispersions stabilized by surfactants and co-surfactants, with globule sizes ranging from 1 to 100 nm. When combined with a gel base, they form nanoemulgels. Nanoemulsions significantly enhance transdermal and dermal drug delivery—both in vitro and in vivo—compared to traditional emulsions and gels. Their high drug-loading capacity and small droplet size improve drug absorption through the skin, leading to a faster onset of therapeutic action.
Macroemulsion Gel [33–35]
Macroemulsion gels are emulgels containing emulsion droplet particles larger than 400 nm. While the droplets are not visible to the naked eye, they can be observed under a microscope. Despite being thermodynamically unstable, macroemulsions can be stabilized using surface-active agents. These gels serve as carriers for drugs in topical formulations where larger droplet sizes are acceptable or required.
Advantages of Emulgel [36]
Disadvantages of Emulgel [37]
Composition of Emulgel
Drug – The way a medication penetrates through the skin is mostly determined by its inherent properties. When creating an emulgel for topical or transdermal application, a number of the drug's physicochemical and biological characteristics are essential. When a medication has an appropriate partition coefficient (log) between 0.8 and 5, its ability to cross epidermal barriers is improved. This suggests that the medication is well distributed in lipids and water. In addition to being non-irritating and having a skin permeability coefficient of 0.5×10?³ cm/h, the drug's low polarity makes absorption easier.[38]
Vehicle – Both aqueous and oily carriers are utilized to handle hydrophilic and hydrophobic medicines in the preparation of an emulgel. In order to provide a well-balanced formulation, aqueous phase vehicles—such as alcohol, water, and other water-based substances—help dissolve and assimilate hydrophilic medications, while oily vehicles aid with hydrophobic drugs.[39]
Oils – The formulation is created by combining a number of ingredients during the oily phase of emulsion manufacturing. For external uses, mineral oils can be used alone or in combination with hard or soft paraffin to deliver medications. These oils have occlusive properties that help retain moisture and give the emulsions sensory features. On the other hand, oils used in oral preparations, such as castor and mineral oils, are not recyclable and often have a localized laxative effect. Fish liver oils and a range of vegetable oils, such as those from corn, cotton seed, and archies, are commonly used in dietary supplements due to their nutritional benefits and distinct health properties.[40]
Emulsifiers – For emulsification to proceed smoothly during the manufacturing process, emulsifying agents are necessary. Additionally, they support emulsion stability throughout time. Commercial formulations can stay stable for months or even years, whereas formulated emulsions can endure for days. Stearic acid, sodium stearate, polyethylene glycol (PEG), 4031 stearate, sorbitan monooleate (Span 80), and polyoxyethylene sorbitan monooleate (Tween 80) are a few examples.[41]
Gelling Agent – These compounds serve as thickening agents and increase the viscosity of different dosage forms, improving the formulations' stability and uniformity. They contribute significantly to the preparation of emulgels by giving the formulation its viscosity, stability, and rheological characteristics. They serve to turn the emulsion into a semi-solid gel matrix, boosting its spreadability, adherence and retention on the skin, thereby optimizing drug administration and therapeutic efficacy.[42]
Types of Gelling Agent
Natural polymer – Proteins (gelatin, collagen, egg whites, and casein) and polysaccharides (guargum, acacia gum, tragacanth gum, pectin, starch, xanthan gum, dextran, succinogluconate, etc.) are examples of natural polymers.
Semi Synthetic Polymers – These polymers, which include carboxymethylcellulose, hydroxylpropylcellulose, ethylcellulose, hydroxyethylcellulose, silicate (Veegum®), methylcellulose, sodium alginate, and carbopol-940, contain both natural and manufactured polymers.
Synthetic Polymers – These are entirely synthetic and produced on a bigger scale in a lab, such as polyvinyl alcohol, poloxamers (Pluronics®), and carbopols® (now known as carbomers).[43]
Permeation enhancer
By allowing medications to pass through biological barriers like the skin or mucous membranes, penetration enhancers increase drug delivery systems. These enhancers improve the therapeutic results of topical and transdermal medications by increasing drug bioavailability and efficacy.
Features of Permeation enhancer:
Co-surfactants: Surfactants with single chains alone cannot sufficiently reduce the oil-to-water interfacial tension. Therefore, to enable emulsification, various co-surfactants are used such as propylene glycol (PG) and cetostearyl alcohol.[43]
Preservatives – Preservatives are necessary to stop microorganisms from growing. Parabens such as methyl, propyl, benzyl, butyl, and p-hydroxy benzoate are commonly used for this.[43]
Methods for preparation of Emulgel
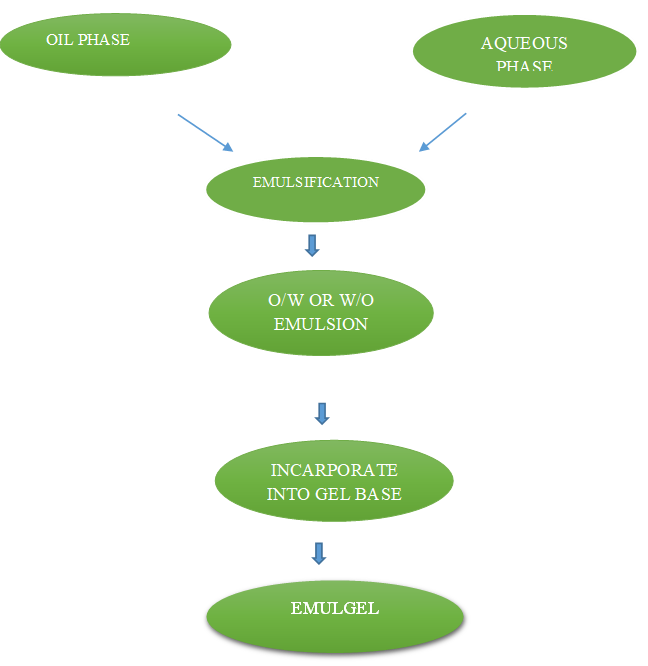
Fig 2. Methods for preparation of emulgel
Methods for preparing emulgel involve three main steps:
There are three primary steps in the straightforward process used to prepare emulgel. To create emulgel, the first two processes are to formulate the emulsion and gel base independently, then incorporate the emulsion into the gel base. The aqueous phase of the emulsion formulation is first made by dissolving emulsifying agents such as Tween 20 or hydrophilic surfactants in distilled water. Likewise, emulsifying agents such as Span 20 or lipophilic surfactants are dissolved in oil (liquid paraffin) to create the oil phase. After being heated independently to a temperature between 70° and 80°, the oil and aqueous phases are combined while being constantly stirred to create an emulsion. Dispersing gelling chemicals, such as Carbopol or HPMC, into distilled water creates the gel phase. In order to create emulgel, the emulsion and gel phase are finally combined in a 1:1 ratio while being gently stirred.[44]
EVALUATION OF EMULGEL[43]
Visual examination
The prepared formulation is visually examined to assess its color, texture, and uniformity in order to evaluate its physical characteristics.
Homogeneity
Assessing homogeneity involves looking at the gel's appearance and looking for any aggregates in formulation.
pH
To ascertain the emulgel's pH, dissolve it in water to create a 1% solution first. Next, use a digital pH meter to measure this solution's pH in order to get an accurate reading.
Spreadability
Spreadability was assessed by applying an excess of sample on each of the two glass slides, which was then compacted to a consistent thickness using a 1 kg weight for five minutes.
A precise 50 g weight was added to the lower plate. The measure of spreadability was the amount of time needed to spread the two slides, or the amount of time it took for the upper glass slide to pass over the lower plate.
Spreadability (S) = M × L / T
where L is the length traveled on the glass slide, T is the time required, and M is the weight tide to the top slide.
Drug content determination
Dissolve 1 gram in 100 milliliters of solvent to find the amount of drug present in the emulgel. Filtering the solution and then appropriately diluting it for spectrophotometric measurement will produce clarity.
Centrifugation Analysis
By mimicking high-speed circumstances, the centrifugation technique is used to evaluate the stability of emulgel formulations. This method, which is usually carried out a week following the emulgel's creation, aids in determining whether the formulation stays stable or if any phase separation or changes take place over time. Centrifuging the emulgel for 30 minutes at 3000 rpm is required for the stability evaluation. Centrifugation 71 can be used to detect any phase separation, sedimentation, or instability inside the emulgel.
Viscosity determination
The digital viscometer (Brookfield), which has a cone and plate arrangement, was used to measure the viscosity of several emulgel formulations at room temperature. This tool provides crucial information on the consistency of the emulsion by precisely measuring how thick and flow-resistant it is. The spindle was allowed to rotate freely in the emulgel when the viscosity reading was taken. Spindle 6 is used to measure the viscosity of emulgel at 100 rpm.
Skin irritation test: For topical dose forms, a skin irritation test is required. to assess irritability following a single topical emulgel treatment. After applying the optimal formulation to the skin (3 cm2), reactions like erythema and edema are measured and graded 24 hours later. After a day, the emulgel is taken off, and the treatment areas are cleaned.
Extrudability study
Extrudability is measured by the force needed to push emulgel out of a tube. The method determines the applied shear in that region and states that plug flow happens when the shear rate exceeds the yield value. In this experiment, the emulgel is extruded using a collapsible metal tube. The weight in grams needed to extrude an emulgel ribbon in ten seconds is measured in order to determine extrudability. Better extrudability is indicated by a higher weight. To guarantee measurement accuracy, this procedure is carried out three times, and the average value is computed. The following formula is used to determine extrudability. The formula for calculating extrudability is area (cm2) divided by weight (g) used to extrude emulgel from the tube.
Globule Size and Distribution in Emulgel
The globule size and distribution within the sample are ascertained using the Zetasizer instrument. A one-gram sample is dissolved in filtered water and then thoroughly mixed by spinning to produce a uniform dispersion. Using the zetasizer, this procedure guarantees precise assessment of the globule properties. This sample is then put into the zetasizer's photocell, and the distribution and mean globule diameter are determined.
In vitro cumulative drug release studies by percentage
To prepare the egg's outer shell membrane, the calcified layer is dissolved by submerging the egg in a 50% aqueous solution of HCl. To remove the contents of the egg, the membrane is carefully cut, and the contents are then washed with regular saline solution. The inner membrane is kept in distilled water after being frequently cleaned with water. After cutting the necessary length of egg membrane and tying it with thread to the diffusion cell's bottom (grounded) layer, it is put in a beaker with 100 milliliters of 5.5 pH phosphate buffer. To stir the contents during the studies, a magnetic bead is added to the outer compartment. The complete system is placed in a magnetic stirrer and temperature
Swelling index
The formulation with the highest swelling index is capable of absorbing exudates from wounds. To determine the swelling index, 1g of emulgel is placed in a petridish with 10 ml of 0.1 N NaOH and covered with permeable aluminum foil. The samples are taken at different times, given a little time to dry, and then weighed. Next, the swelling index is computed using a formula. The index (????????) % is equal to [(????????−????????)/????????] ×100. where Wo is the initial weight of the emulgel at zero time, (SW) % is the equilibrium swelling percentage, and Wt is the weight of the swollen emulgel after a predetermined amount of time.
Analysis of stability
Stability is the capacity of a drug formulation to maintain its unique chemical, physical, toxicological, and therapeutic characteristics inside a certain container. All stability investigations are conducted in accordance with ICH guidelines.
INFLAMMATION[45,46]
Inflammation is a protective reaction involving immune cells, blood vessels, and chemical mediators that occurs when bodily tissues react to hazardous stimuli like pathogens, damaged cells, or irritants. Inflammation serves to remove the initial source of cell damage, remove necrotic cells and tissue that has been harmed by the first insult and the inflammatory process, and promote initial tissue restoration.Inducers, mediators, effectors, and sensors make up the inflammatory pathway. Both infectious and non-infectious stimuli, including poisons, foreign objects, necrotic cell signals, and damaged tissue, can act as inducers. The inducer activates sensors, which are specialized molecules that cause mediators to be produced. Endogenous substances known as mediators have the ability to activate effector tissue and cells, cause pain, and either stimulate or inhibit inflammation and tissue repair. Numerous other pathways in the inflammatory pathway are created by the conjugation of these multiple participants, and the stimuli that are included determine which path is chosen. One of the objectives of a sterile stimulation is to keep the wounded tissue from becoming infected. Pathogen associated molecular patterns (PAMPs), which are molecules from pathogenic organisms, and damaged associated molecular patterns (DAMPs), which are molecules generated from host cells that have been damaged, are two categories of inducers. Different receptors in dendritic and macrophage cells recognize these patterns, and pain receptors also detect injured tissue. When such receptors are stimulated, inflammatory cytokines are produced. These include, among others, TNF-alpha, IL-10, and IL-6, which alter the endothelium and let immune cells to pass through the junction between the junctions.The immune cells that rely on the tissue's level of inflammation While full-blown inflammation also causes neutrophils to migrate to the tissue, para-inflammation results in the recruitment of monocytes. Enzymes that combat infectious organisms and eliminate dead cells will subsequently be released by these cells. Reactive oxygen species (ROS) will build up in tissue as a result of this enzyme release. They are referred to as "damaged healthy cells." Additionally, pro-inflammatory cytokines released by endothelial cells draw in more inflammatory cells. Additionally, plasma moves to nearby tissues, causing tissue edema. Anticoagulant protein production is decreased, and circulating platelets are also activated and aggregate. This may result in intravascular thrombosis, which may cause organ failure if it occurs in excess.
Causes of inflammation[47]
Signs of inflammation[48]
Acute inflammation might manifest as any one of five symptoms.
Types of inflammation[48]
1. Acute inflammation
The healing process begins when the body reacts by releasing cytokines, which are proteins that increase inflammation. Acute inflammation is frequently brought on by trauma, dangerous substances, or microbial invasion (i.e., bacteria and viruses). Acute inflammation happens quickly, can be severe, and lasts for a brief amount of time. While signs and symptoms may last a few days, more serious causes may cause them to last longer.
Five distinct symptoms are often caused by acute inflammation. These consist of:
2. Chronic inflammation
Long-term inflammation that lasts for months to years is called chronic inflammation. An autoimmune condition, in which the immune system targets its own healthy tissues because it believes they are ill, is typically the source of chronic inflammation. Additionally, low-level exposure to irritants such industrial chemicals might result in chronic inflammation. whether it resulted in an acute inflammation, as is the case with disease or infection, or over extended periodsof time or failure to cure.
Compared to acute cases, chronic inflammation symptoms typically manifest differently. Acute inflammation may be followed by chronic inflammation, or it may start slowly. It lasts longer and is linked to tissue damage, fibrosis, blood vessel proliferation, and the presence of macrophages and lymphocytes.
Symptoms are
Treatment of inflammation depend on[49]
1. Types of Inflammation
2. Underlying Causes
3. Affected Body Systems
NSAIDs (Nonsteroidal Anti-inflammatory Drug)[48]
NSAIDs (nonsteroidal anti-inflammatory medications) have antipyretic and analgesic effects. Oral NSAIDs are useful for treating a range of acute and chronic pain conditions, but using them can have major side effects, especially gastrointestinal disorders. For a number of clinical indications, transdermal distribution of NSAIDs has proven to be a practical method of administration. Furthermore, applying gel as a method of delivery. can give a quicker release of the drug's ingredient and lengthen the time it stays on the skin. In most cases, extensive preformulation experiments are required to maximize both skin penetration and medication release from the topical carrier.
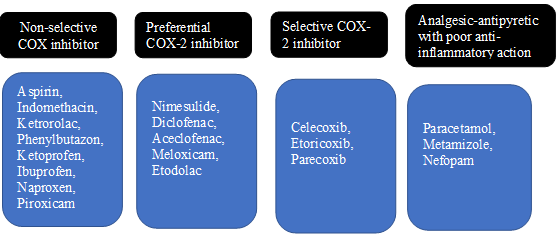
Classification of NSAIDs
Mechanism action of NSAID’S48
NSAIDs reversibly block the cyclooxygenase (also known as prostaglandin endoperoxide synthase, or COX) enzyme, which is now known to have two isoforms, COX-1 and COX-2, that mediate prostaglandin synthesis.
Advantages of topical NSAID’S formulation[48]
ANTI-INFLAMMATORY EMULGELS[50]
The characteristics of an emulsion (oil-in-water or water-in-oil) and a gel base are combined in an anti-inflammatory emulgel, a topical medication delivery device. It is intended to alleviate inflammation, discomfort, and swelling locally by delivering anti-inflammatory medications through the skin.
RATIONALE BEHIND USE OF EMULGELS FOR INFLAMMATION
Emulgels enable direct delivery of anti-inflammatory drugs to the affected area, such as the skin, muscles, or joints. This localized approach limits systemic drug absorption, thereby reducing the side effects often associated with oral anti-inflammatory medications.
The combination of emulsion and gel phases in emulgels allows for the efficient delivery of both water-soluble and fat-soluble drugs. The presence of oils and permeation enhancers further facilitates drug penetration through the skin, boosting therapeutic effectiveness.
Thanks to their non-greasy, smooth texture, emulgels spread easily and absorb quickly into the skin. This makes them more comfortable and user-friendly compared to greasy ointments or creams, leading to better patient compliance.
Emulgels provide controlled and sustained release of drugs, which extends their duration of action and reduces the frequency of application.
Emulgels can incorporate various anti-inflammatory agents, ranging from synthetic NSAIDs like diclofenac to natural compounds such as curcumin, allowing for tailored treatment options.
Marketed formulations of emulgel for inflammation[53]
|
Brand Name |
Active Ingredient |
Manufacturer |
|
Voltarol 1.16% Emulgel |
Diclofenac Diethyl Ammonium Salt |
Novartis Pharma
|
|
Diclon Emulgel |
Diclofenac Diethylamine |
Med Pharma |
|
Acent Gel |
Aceclofenac |
Intra Labs India Pvt. Lt |
|
Topinate Gel |
Clobetasol Propionate |
Clobetasol Propionate |
|
Isofen Emulgel |
Ibuprofen |
Beit Jala Pharmaceutical Company |
|
Voveran Emulgel |
Diclofenac Diethylamine |
Dr Reddy’s Laboratories Ltd |
|
Miconaz-H-Emulgel |
Miconazole Nitrate, Hydrocortisone |
Medical Union Pharma Ceuticals |
|
Dosanac Emulgel |
Diclofenac Diethyl Ammonium |
Siam Bheasach |
|
Volini Gel |
Diclofenac Diethylamine |
Ranbaxy Laboratories |
Reported herbal drug emulgels and their efficacy53
|
Herbal Drug |
Category |
Route of Administration |
|
Ginger |
Anti-inflammatory |
Topical(Emulgel) |
|
Clove-Cinnamon |
Anti-fungal & Anti-inflammatory |
Oral(Emulgel) |
NOVEL FORMULATION OF ANTI-INFLAMATORY EMULGEL ARE
Concept: Embed nanoemulsion droplets into a gel base to enhance drug delivery by improving penetration, stability, and providing controlled release.
Novelty: The presence of nano-sized oil droplets boosts skin absorption and increases the drug’s bioavailability.
This formulation integrates multiple plant-derived anti-inflammatory compounds such as:
Novelty: Offers a broad-spectrum, natural anti-inflammatory effect through synergistic action of multiple botanicals, resulting in enhanced efficacy with minimal side effects.
Incorporate thermoresponsive polymers such as Poloxamer 407, which stay in a liquid state at room temperature but transition into a gel when exposed to skin temperature (around 32°C). This improves ease of application and creates a protective gel layer once applied.
Incorporate the anti-inflammatory drug within liposomes or niosomes to achieve:
CURRENT THERAPEUTIC APPROACHES FOR INFLAMATION
1. Pharmacological Management of Inflammation
A. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)[56]
B. Corticosteroids[57]
C. Disease-Modifying Anti-Rheumatic Drugs (DMARDs)[58]
D. Analgesics with anti-inflammatory adjunct properties[59]
2. Topical anti-inflammatory therapeutics[60]
3. Biologic therapies and immunomodulators[61]
4. Natural and phytopharmaceutical approaches[61]
5. Lifestyle & non-pharmacological interventions
A. Dietary interventions[62]
B. Physical activity[63]
C. Stress management[64]
6. Emerging & targeted therapies
A. Nanomedicine & Advanced Drug Delivery Systems[65]
B. Gene-based therapies[66]
C. Microbiome modulation[67]
RECENT ADVANCES IN EMULGEL FORMULATIONS FOR ANTI-INFLAMMATORY APPLICATIONS
Recent investigations have shown that emulgel systems significantly enhance the percutaneous absorption and provide sustained release of active pharmaceutical ingredients (APIs). For example, research on posaconazole-loaded emulgels demonstrated superior dermal delivery compared to traditional topical formulations, addressing common limitations in skin penetration.
The incorporation of nanocarriers, such as nanoemulsions, into emulgel formulations has been extensively studied to improve the solubility, stability, and bioavailability of lipophilic drugs. These nanoemulsion-based gels enable dual release mechanisms—combining both emulsion and gel phases—offering an advanced platform for efficient topical drug delivery.
The therapeutic efficacy of emulgels is highly dependent on the careful selection of formulation components, including gelling agents, surfactants, and permeation enhancers. Optimizing these excipients is essential to achieve desirable rheological characteristics, formulation stability, and enhanced skin permeation.
Emulgels are increasingly favored in dermatological therapy due to their favorable physicochemical properties, such as non-greasiness, transparency, and ease of application, which collectively improve patient adherence. Their efficacy in managing inflammatory dermatoses further emphasizes their growing clinical relevance.
PHARMACEUTICAL CHALLENGES IN FORMULATING AND COMMERCIALIZING EMULGELS FOR MANAGEMENT OF INFLAMMATION[72]
Physical and chemical stability
Emulgel formulations frequently encounter stability problems such as phase separation, creaming, and sedimentation during storage, which can compromise their uniformity. Additionally, degradation processes like oxidation and hydrolysis of both active ingredients and excipients may diminish the product’s efficacy and shelf life. Maintaining stable viscosity and rheological properties over extended periods is also challenging, especially when exposed to fluctuations in temperature and humidity.
Drug loading and controlled release
Formulating emulgels with sufficient drug loading, particularly for poorly water-soluble or hydrophobic anti-inflammatory compounds, remains difficult due to solubility limitations. Achieving controlled and sustained drug release without an initial burst effect requires careful optimization of the formulation components. Furthermore, the use of permeation enhancers must be balanced to improve skin absorption without inducing irritation or toxicity.
Manufacturing and scale-up
Translating lab-scale emulgel production techniques, such as homogenization and sonication, to industrial manufacturing poses reproducibility and scalability challenges. Ensuring consistent batch-to-batch quality, including parameters like particle size distribution and viscosity, during large-scale production is a critical hurdle.
Regulatory and quality control issues
The absence of well-defined regulatory guidelines tailored specifically for emulgels complicates the approval process. Characterization protocols for formulations containing nanocarriers or novel excipients are still under development. Additionally, the safety and efficacy evaluation of emerging bioactive phytoconstituents necessitates thorough toxicological and clinical studies.
Patient-centred challenges
There is a risk of skin irritation or allergic reactions stemming from excipients or penetration enhancers used in emulgels. Unfavorable sensory properties such as greasiness, odor, and poor spreadability can negatively impact patient compliance. Moreover, there is limited long-term safety data available for chronic use of emulgel formulations in inflammatory conditions.
FUTURE PROSPECTS OF ANTI-INFLAMMATORY EMULGELS
The future of anti-inflammatory emulgel development is expected to be shaped by technological innovations and the evolving needs of patient-centric therapeutics. As pharmaceutical sciences advance, emulgels are poised to offer more efficient, targeted, and user-friendly treatment modalities for a wide spectrum of inflammatory disorders. The following key areas highlight potential directions for future research and development:
Emulgel formulations incorporating nanocarriers—such as nanoemulsions, liposomes, niosomes, solid lipid nanoparticles (SLNs), and nanostructured lipid carriers (NLCs)—are likely to gain further traction. These systems enhance the solubility of lipophilic anti-inflammatory drugs, improve dermal penetration, and allow for sustained and site-specific drug release. Future studies may focus on optimizing formulation parameters to improve drug entrapment, minimize systemic absorption, and ensure precise delivery at the site of inflammation.
An emerging trend in emulgel design involves the use of stimuli-responsive materials that react to physiological triggers such as temperature, pH, enzymatic activity, or oxidative stress. Thermoresponsive gels, for instance, undergo phase transitions at skin temperature, promoting prolonged retention and controlled drug release. These intelligent delivery systems are expected to enhance therapeutic efficiency and reduce dosing frequency.
The future of emulgel therapy may align with personalized medicine approaches, wherein formulations are adapted based on individual patient factors including skin physiology, genetic predisposition, and disease severity. Such customization would optimize therapeutic outcomes and reduce the risk of adverse effects, particularly in patients with hypersensitive or compromised skin barriers.
There is increasing emphasis on incorporating natural, biodegradable, and biocompatible excipients in emulgel formulations. Plant-derived polymers (e.g., xanthan gum, alginate), phospholipids (e.g., lecithin), and essential oils may serve as functional gelling agents, emulsifiers, or penetration enhancers. These components not only improve safety profiles but also align with regulatory trends toward sustainable and “green” pharmaceutical products.
Next-generation emulgels may be designed to co-deliver multiple active pharmaceutical ingredients (APIs), offering anti-inflammatory, antimicrobial, and antioxidant properties in a single formulation. This synergistic approach is particularly beneficial for complex skin conditions involving both inflammation and infection, thereby minimizing the need for multiple medications and improving adherence.
Combining emulgels with advanced transdermal systems—such as microneedles, iontophoresis, or ultrasound-mediated delivery—could enhance drug absorption beyond the epidermal layer and facilitate systemic effects. This innovation may broaden the applicability of emulgels from purely topical treatments to systemic management of inflammatory conditions.
For successful commercial translation, there is a need to refine large-scale manufacturing processes that ensure consistency, cost-effectiveness, and quality assurance. Techniques such as continuous processing, high-pressure homogenization, and real-time monitoring (PAT tools) will be vital for overcoming scalability and reproducibility challenges.
As emulgel-based drug products gain popularity, regulatory bodies are anticipated to establish dedicated guidelines concerning their evaluation. These would include standardized protocols for assessing physicochemical properties, drug release kinetics, microbiological stability, and dermal safety. Regulatory harmonization will facilitate smoother product approval and market penetration.
Robust clinical trials will be essential to establish the safety, efficacy, and acceptability of novel anti-inflammatory emulgels in human populations. Additionally, real-world evidence and pharmacovigilance data will contribute to post-marketing surveillance, enabling early detection of rare adverse events and supporting long-term therapeutic use.
CONCLUSION
Anti-inflammatory emulgels represent a valuable advancement in topical drug delivery, combining the structural advantages of both emulsions and gels. This biphasic system enhances percutaneous absorption, extends drug retention at the site of application, and promotes user acceptability due to their non-oily texture and ease of application. Recent progress—particularly the incorporation of nanotechnology, stimuli-responsive systems, and plant-derived actives—has broadened their applicability in treating both acute and chronic inflammatory disorders. However, critical challenges remain, including issues of physicochemical stability, precise drug release modulation, scalability in manufacturing, and the lack of standardized regulatory guidelines. Future directions are likely to focus on the development of patient-tailored, multifunctional emulgels with improved safety, efficacy, and compliance. The integration of advanced formulation strategies and clinical validation will be essential to support their transition from experimental preparations to widely accepted therapeutic options in dermatology and inflammatory disease management. Anti-inflammatory emulgels offer an innovative and efficient approach for topical drug delivery by combining the benefits of both emulsions and gels. This formulation enhances drug stability, improves skin absorption, and increases patient acceptability. By enabling targeted and sustained release of anti-inflammatory agents, emulgels provide effective treatment with reduced systemic exposure and side effects. Advances in nanoemulgel technology further refine drug delivery and therapeutic outcomes, making these formulations highly suitable for treating various inflammatory disorders. Ongoing research is likely to expand their use and improve treatment options in dermatology and related fields.
REFERENCES

Tanaya Vairagade, Dr. R. H. Kasliwal, Dr. Yogesh Gholse, Dr. D. R. Chaple, Pranali Dhule, Trupti Nimburkar, Prachi Karadbhajane, Vidhi Sonbirse, Anti-Inflammatory Emulgels: Emerging Trends and Future Perspectives in Topical Drug Delivery System, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 1003-1025. https://doi.org/10.5281/zenodo.17551041
 10.5281/zenodo.17551041
10.5281/zenodo.17551041