
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Shraddha Institute of Pharmacy, Kondala Zambre Washim, Maharashtra India- 444505
Wastes are the unwanted or unusable materials that people will no longer use for, which are either intended to get rid of or have already been discarded. Moreover, wastes can be hazardous to human or the environment as such, which has to be discarded immediately, else may cause serious health related problems in human. Biomedical waste means any solid or liquid waste which is generated during the diagnosis, treatment or immunization of human beings or animals. Thus pharmaceutical waste are manage by the various treatment processes and also aware to manage the pharmaceutical waste by the drugs Reclamation Program. Survey on Drugs Reclamation Program to waste Segregation, collection, storage, survey on Drugs Reclamation Program areness about the manage the pharmaceutical waste in rural areas hospitals medicals.
Wastes are the unwanted or unusable materials that people will no longer use for, which are either intended to get rid of or have already been discarded. Moreover, wastes can be hazardous to human or the environment as such, which has to be discarded immediately, else may cause serious health related problems in human. Wastes should else be recycled to another useful products. Wastes may be of different forms like household rubbish, sewage, sludge, wastes from manufacturing activities, packaging items, discarded cars, old televisions, garden waste, old paint containers etc. Thus, daily activities may give rise to a large variety of different wastes arising from different sources. This might be developed from households, commercial activities (e.g., shops, restaurants, hospitals etc.), industry (e.g., pharmaceutical companies, clothes manufacturers etc.), agriculture (e.g., slurry), construction and demolition projects, mining and quarrying activities and from the generation of energy. With such vast quantities of waste production, it is of vital importance that these should be managed in such a way that they does not cause any harm to either human health or to the environment. There are a number of different options available for the treatment and management of wastes including prevention, minimization, re-use, recycling, energy recovery and disposal. Pharmaceutical wastes are of different types mainly hazardous wastes and non hazardous wastes[1]. Biomedical waste means any solid or liquid waste which is generated during the diagnosis, treatment or immunization of human beings or animals. Biomedical waste poses hazards due to two principle reasons: first is infectivity and other toxicity. There are two sources of biomedical waste. Major sources: Govt. Hospitals, Nursing homes, Medical Colleges, PHC (Primary Health Centers), Research Centers, Veterinary Colleges, Animal Research Centers, Blood Bank, Biotechnology Institutions, Isolation Wards, ICU etc. Minor sources: - Dentist clinic, Animal houses, slaughter houses, vaccination centers, funeral services, etc. Classification: - Waste is of three types: solid, liquid and gaseous waste. They are further classified as hazardous & non- hazardous waste. Most of the biomedical waste, nearly 80-85% is non hazardous only 15 to 20% of waste is hazardous, which needs proper segregation collection, transportation, treatment & disposal of Hazardous waste.[2]
Pharmaceutical waste is further classified in 2 categories:-
Wastes that are dangerous or potentially harmful to human health or the environment is called as hazardous waste. These can be liquids, solids, contained gases, or sludges. Hazardous wastes are divided into two categories:
(1) Listed wastes
(2) Characteristic wastes.
Pharmaceutical wastes come under listed wastes since they contain commercial chemical products. Characteristic wastes are regulated because they exhibit certain hazardous properties – ignitability, corrosivity, reactivity and toxicity. Wastes that are not listed and do not exhibit a characteristic are considered solid waste. Solid wastes should be discarded according to state and/or local regulations, including regulated medical waste requirements[3].
Ignitability: The objective of the ignitability characteristic is to identify wastes that either present a fire hazard under routine storage, disposal, and transportation or are capable of exacerbating a fire once it has started. There are several ways that a drug formulation can exhibit the ignitability characteristic. Many of the hazardous wastes that pharmacies handle are hazardous because they are ignitable. These wastes often pose the greatest management problems for pharmacies. Ignitable wastes are easily combustible or flammable.
Corrosivity: Corrosive wastes corrode metals or other materials or burn the skin. These liquids have a pH of 2 or lower or 12.5 or higher. Examples of acids that exhibit a pH of 2 or lower include glacial acetic acid. Examples of bases that exhibit a pH of 12.5 or higher include Potassium Hydroxide and Sodium Hydroxide. Generation of corrosive pharmaceutical wastes is generally limited to compounding chemicals in the pharmacy. Reactivity Reactive wastes are unstable under “normal” conditions. They can cause explosions, toxic fumes, gases, or vapors when heated, compressed, or mixed with water.
Toxicity: Wastes are toxic if they contain toxic organic chemicals or certain heavy metals, such as chromium, lead, mercury, or cadmium. Approximately 40 chemicals meet specific leaching 12 concentrations which classify them as toxic. Wastes that exceed these concentrations must be managed as hazardous waste.[4]
Pharmaceutically inert: Certain medicinal products have no pharmaceutical properties but are still controlled and administered by medical stuffs (examples include sodium chloride or dextrose solutions). Through use, however, these products may become contaminated, or mixed with other compounds and therefore require assessment for hazardous properties prior to disposal. Biomedical Wastes Biomedical wastes can be briefly defined as any solid or liquid waste that is generated in the diagnosis, treatment of immunization of human beings or animals in research pertaining thereto, or in the production or testing of biological material.[5]
Non-hazardous waste refers to materials that do not pose a significant risk to human health or the environment. Unlike hazardous waste, it lacks dangerous properties such as toxicity, flammability, or reactivity. Common examples include household waste like paper, plastic, food scraps, and packaging materials, as well as industrial by-products such as non-toxic metals, glass, and construction debris like bricks and drywall. These wastes are typically generated by homes, offices, manufacturing facilities, and construction sites. Non-hazardous waste is usually managed through landfilling, recycling, composting, or in some cases, incineration. Recycling and composting help reduce the volume of waste sent to landfills and support environmental sustainability by conserving resources and lowering emissions. Governments and environmental agencies regulate the handling and disposal of non-hazardous waste to ensure it does not become a nuisance or harm local ecosystems. Proper segregation, reduction at the source, and public awareness are key strategies in effective non-hazardous waste management. By promoting responsible disposal and recovery methods, communities can significantly minimize their environmental impact while maintaining public health and safety[6].
2. LITERATURE REVIEW
Biomedical waste poses significant risks due to its hazardous components, which constitute approximately 10–25% of the total BMW. These hazardous wastes include physical, chemical, and microbiological elements that can endanger healthcare workers and the environment if not properly managed.
Focus on the critical issues surrounding waste generation and management within the pharmaceutical industry. The review highlights different types of pharmaceutical wastes, including solid, liquid, and hazardous materials, and discusses various methods of disposal and treatment to ensure environmental safety and regulatory compliance. It emphasizes the growing need for sustainable waste management practices to minimize the environmental impact of pharmaceutical production and consumption. Strategies like recycling, reuse, incineration, and advanced waste treatment technologies are explored. The authors advocate for stringent waste management protocols, training programs, and continuous monitoring to promote both public health and environmental protection.
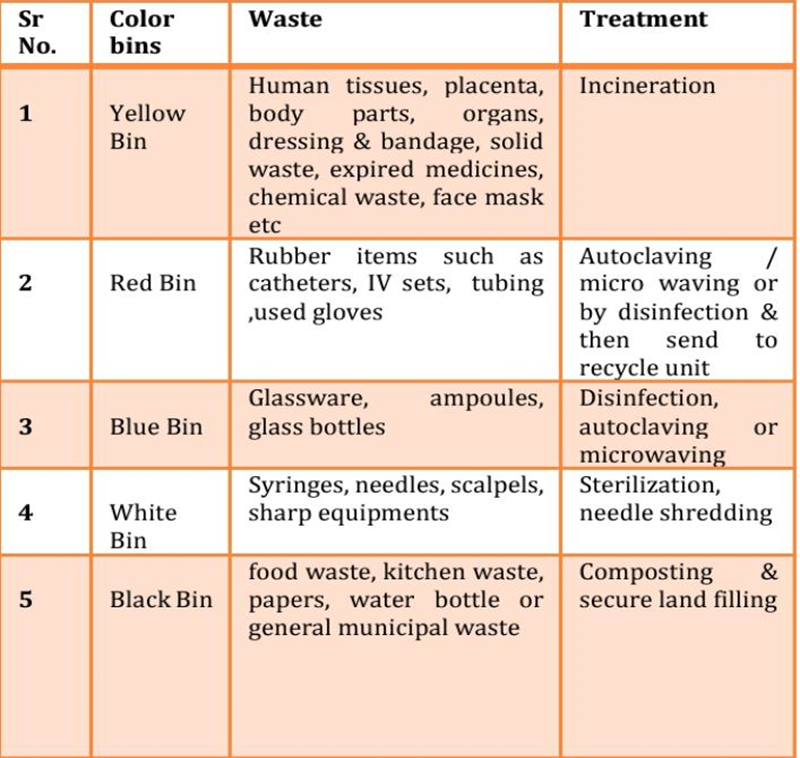
B. Waste segregation and collection
Table No. 1: waste segregation and collection
C. Storage and handling
N Akola, there are near about 720 hospitals which emit Bio medical waste about 23.5 tons per month. This study of Bio medical waste is conducted by visiting hospitals like GMC Hospital (Akola), ICON Hospital Akola, OZON Hospital (Akola), District Women’s Hospital Akola and treatment plant of Bio medical waste which of Global Eco Save Systems Privet limited, first showed up in 2003.[7]
Collection
The containers or bins should be placed in such a way that 100% collection is achieved. Sharps must always be kept in solid containers to avoid accidents to the workers. After collection the bio medical waste is stored in proper storage rooms. Separated wastes of different types need to be collected in different color-coded containers.[8]
Storage
All biomedical waste will be safely bundled in biohazard compartments which will be marked with the images. All BMWs bundled in compartments stamped biohazard No individual will store biomedical waste above 0º C for over seven days without the composed endorsement of the important lead office, given that untreated obsessive waste will be discarded inside 48 hours.[9,10,]
D.Transportation
Waste from the Hospitals is transported to the treatment facility in Badnera by means of wheeled trolleys, containers, or carts and trucks that are not used for any other purpose and meet the following rules: easy to load and unload; no sharp edges that could damage waste bags or containers during loading and unloading; easy to clean. The waste bags seals should be in position and fixed at the end of transportation.[11,12]
E. Treatment
1. Hazardous waste
As per color coding, yellow dust bin waste must be incinerated at 800º C – 1100º C in incinerators. Red Dustbin waste such as rubber, gloves, catheters, IV sets, tubing should be either autoclaved or disinfected property before being sent to recycling unit. Blue bins waste such as glassware, ampoules, glass bottles should be disinfected or auto claved before burying. White bins waste such as syringes, needles scalpers, sharp equipment should be well sterilized, needles shredded & handed over to proper recycling personal. Black bins.[13,14]
Incineration: This process reduces the volumes of solid waste to 20 to 30 percent of the original volume. Incineration and other high temperature waste treatment systems are sometimes described as “thermal treatment”. Incinerators convert waste materials into heat, gas, steam and ash.
Autoclaving: In autoclaving, saturated steam in direct contact with the BMW in a pressure vessel at time lengths and temperatures sufficient to kill the pathogens are used for sterilization. Minimum temperature, pressure, and residence time for autoclaves for safe disinfection are specified in the Biomedical Waste Rules.[15,16,17]
Microwaving: Microwaving is not suitable for human anatomical, animal, chemical, or pharmaceutical wastes, or for large metal parts. Microwaving produces a waste that can be land filled with municipal waste. The advantages of this treatment technology are its small electrical energy needs and no steam requirement. The disadvantages include the need for qualified technicians and frequent breakdown of shredders.
Chemical treatment: Chemical disinfection is most suitable for treating liquid wastes such as blood, urine, stools, or health care facility sewage. Addition of strong oxidants-like chlorine compounds, ammonium salts, aldehydes, or phenol compounds-kills or inactivates pathogens in the BMW. However, microbiological cultures, mutilated sharps, or shredded solids can also be treated by chemical disinfection.[18,19]
2. Non hazardous waste
1.Waste minimization: Methods of avoidance include reuse of secondhand products, repairing broken items instead of buying new, designing products to be refillable or reusable (such as cotton instead of plastic shopping bags), encouraging consumers to avoid using disposable products (such as disposable cutlery), removing any food/liquid remains from cans, packaging, and designing products that use less material to achieve the same purpose (for example, light-weighting of beverage cans).
2. Reuse: Re-use means the use of a product on more than one occasion, either for the same purpose or for a different purpose, without the need for reprocessing. Re-use avoids discarding a material to a waste stream when its initial use has concluded. It is preferable that a product be re-used in the same state.
3. Recycling: Recycling involves the treatment or reprocessing of a discarded waste material to make it suitable for subsequent reuse either for its original form or for other purposes. It includes recycling of organic wastes but excludes energy recovery. Recycling benefits the environment by reducing the use of virgin materials.[20]
F. Awareness and training
Survey on Drugs Reclamation Program
A drugs Reclamation Program focuses on the proper collection, disposal, and possible reuse (if applicable) of unused, expired, or unwanted medications. Training and awareness programs for such initiatives are essential to ensure public safety, environmental protection, and compliance with regulatory guidelines. The Drugs Take-Back Program was officially established by the U.S. Drug Enforcement Administration (DEA) in 2010. The first National Prescription Drug Take Back Day took place on September 25, 2010. This program was created in response to growing concerns about the misuse, abuse, and environmental impact of unused or expired medications. It provided a safe, anonymous way for individuals to dispose of prescription drugs and has since become a biannual event, significantly contributing to public health and safety. The most recent National Prescription Drug Take Back Day was held on October 26, 2024, across the United States. This biannual event, organized by the U.S. Drug Enforcement Administration (DEA), provides a safe, convenient, and responsible means of disposing of unused or expired prescription medications.[21]
Awareness Initiatives
In Social Media Campaigns taken the online survey
After the training, an online survey can gauge the effectiveness of the training and assess whether participants feel prepared to implement or promote the drug take-back program. It can include questions
11. What color dustbin is used for disposing infectious biomedical waste (e.g., gloves, cotton with blood)?
12. Which type of waste should be disposed of in the red dustbin?
13. Who can participate in the Drugs Reclamation Program?
14. What is one way the government can support pharmaceutical waste management?
15. is the key message of a pharmaceutical waste awareness campaign?
All the response I achieved by the online survey in that we calculate the percentage above questions answers in bar graph and pie chart we plot the response of survey of peoples. We have seen the how many people’s are aware of drugs reclamation program. Seen in fig no.1 and 2.
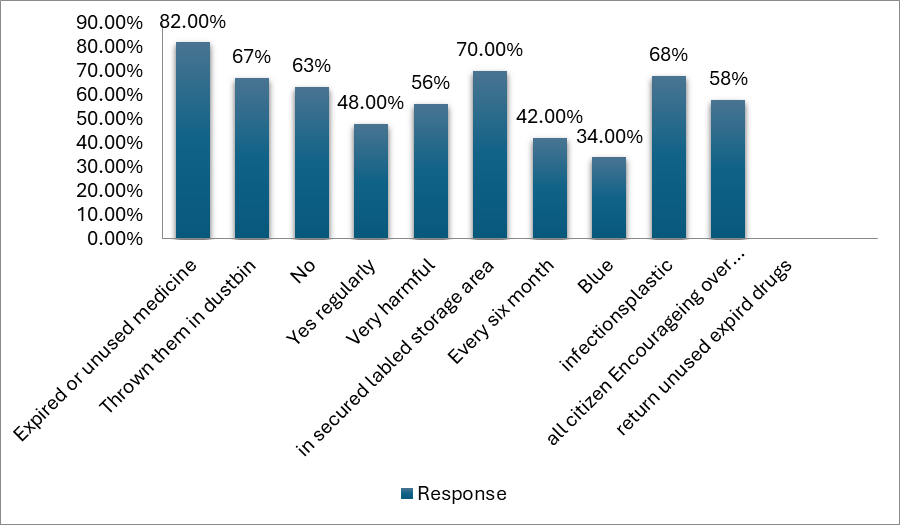
Fig. No. 1 : Survey on drug reclamation program
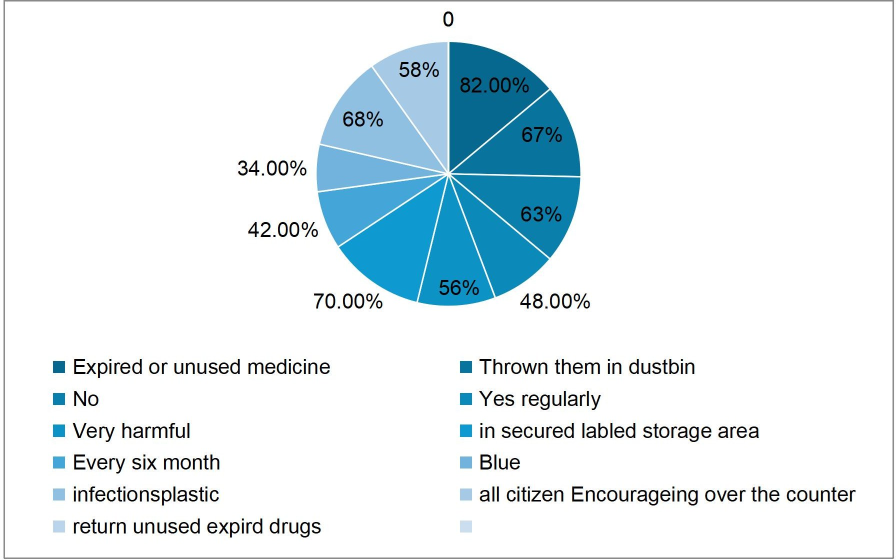
Fig. No. 2 : Survey on drug reclamation program
Prevents pharmaceutical residues (like antibiotics, hormones, and cytotoxic drugs) from entering water bodies, which can harm aquatic life.Reduces soil contamination, preserving biodiversity and agricultural productivity.Limits air pollution from improper incineration of hazardous substances.Minimizes the risk of accidental ingestion, especially by children or animals.Reduces the chance of pharmaceuticals entering drinking water sources.Helps control the spread of antimicrobial resistance by preventing helps hospitals, pharmacies, and manufacturers meet local and international environmental regulations (e.g., WHO, EPA, EU Waste Directives).Avoids legal penalties, lawsuits, and reputational damage. Some non-hazardous pharmaceutical waste can be safely incinerated for energy recovery.Certain packaging materials (like plastics and glass) can be recycled after proper decontamination. Enhances the reputation of pharmaceutical companies and healthcare providers as environmentally responsible organizations. Builds public trust and loyalty. Streamlined waste management processes improve internal hospital/pharmacy workflow. Reduces risks during audits and inspections.
2. Public Awareness 63% of participants became more aware of safe medication disposal methods. Increased community knowledge about the dangers of expired and unused drugs.
3. Volume of Drugs Collected 70% of pharmaceuticals safely collected and destroyed. Most collected drugs were painkillers, antibiotics, and antidepressants.
4. Public Health and Safety 68% of accidental poisoning, especially among children and pets, reported after the program started. Potential reduction in drug abuse due to fewer unused prescriptions available in homes.
5. Participation Rates 66% of targeted households participated in the collection drives. Pharmacies and healthcare facilities showed high levels of cooperation.
6. Challenges Identified Some areas reported low participation due to lack of awareness. Need for more frequent collection events and better advertising.
7. Recommendations Expand educational outreach campaigns. Offer more drop-off points (like pharmacies, police stations, clinics). Improve collaboration with healthcare providers.
Effective pharmaceutical waste management offers critical environmental, public health, and organizational benefits. Preventing pharmaceutical residues such as antibiotics, hormones, and cytotoxic drugs from entering water bodies protects aquatic life, reduces soil contamination, and preserves biodiversity and agricultural productivity. Proper disposal limits air pollution caused by hazardous substance incineration and minimizes the risk of accidental ingestion by children and animals. It also reduces the chance of pharmaceuticals contaminating drinking water sources and helps curb the spread of antimicrobial resistance. Hospitals, pharmacies, and manufacturers benefit by complying with local and international environmental regulations (such as WHO guidelines, EPA standards, and EU Waste Directives), avoiding legal penalties, and safeguarding their reputations. Additionally, non-hazardous pharmaceutical waste can be incinerated for energy recovery, and properly decontaminated packaging materials (plastics, glass) can be recycled. The program also enhances the Image of pharmaceutical companies and healthcare providers as environmentally responsible, boosting public trust and internal efficiency. It reduces risks during audits and improves overall waste management workflows.
Challenges and Recommendations
Low participation in some areas highlighted the need for better education and more frequent collection events. Recommended actions include expanding outreach campaigns, increasing the number of drop-off locations, and improving partnerships with healthcare providers
Wastes are the unwanted or unusable materials that people will no longer use for, which are either intended to get rid of or have already been discarded. Pharmaceutical waste management is a challenge to the medical personnel who works in the recycling industries, government administrations, policy planning’s, quality assurance, etc., for the effective waste management. New classification for medical wastes for their easy removal and effective technique have to be developed in a continuous manner and it has to be ensured that these can decrease the cost of the waste management. For the reduction of waste materials the authorities must implement different techniques and strategies. Improper management of waste at healthcare centers. Well documented instructions are not provided Proper separation of waste is not done. Mixing of Bio-medical waste with municipal waste and residential waste. As the improper segregation is done plastic waste is mixed with other waste which reaches to treatment site. Awareness about the biomedical waste in peoples is negligible. Very less knowledge about biomedical waste in peoples. Rules are not followed properly. Proper training and education about the biomedical waste is not given to healthcare facility staff.
REFERENCES

Pradnya Lahupanchang*, Shubham Tikait, Dr. Swati Deshmukh, Awareness Of Pharmaceutical Waste Management by Drug Reclamation Program, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 2633-2644. https://doi.org/10.5281/zenodo.15431403
 10.5281/zenodo.15431403
10.5281/zenodo.15431403