Bharat Institute of Technology, Mangalpally, Hyderabad.
Peritoneal tuberculosis is a type of abdominal extraperitoneal tuberculosis that happens when Mycobacterium tuberculosis infects the peritoneum. It is the sixth most common place where tuberculosis affects parts of the body, excluding the lungs, around the world. The main way to treat it is through anti-tubercular therapy. Even though ATT is proven to be effective and safe, it is known to cause harmful side effects, with liver damage being the most serious. Liver problems caused by ATT are among the most common and severe side effects of the main treatment for tuberculosis. A 61-year-old woman was admitted to the hospital because she had yellowing of both eyes and stomach discomfort. After looking at her symptoms and test results, doctors found that her liver was damaged because of the medication ATT. They also thought she might have either cholangiocarcinoma or gallbladder carcinoma. Her condition was managed through the appropriate therapy.
Tuberculosis is a long-term infectious disease that can affect almost any part of the body, including the abdomen, bones, kidneys, and digestive system. The main treatments for TB, called first-line anti-tubercular therapy, include drugs like isoniazid, rifampicin, pyrazinamide, and ethambutol. These medications are still the standard for treating TB. However, they can cause different levels of harm to the body, depending on how the liver processes them and how sensitive each individual is. One of the biggest problems with these drugs is liver damage. This can lead to stopping the treatment early, making it less effective, and even causing the disease to come back or become harder to treat. Liver injury caused by TB drugs is known as anti-tubercular therapy-induced liver injury. It affects up to 28% of patients mildly and 1 to 5% severely. The risk is higher for older people, those with hepatitis B or C, or those who use alcohol. Recognising this problem early is very important because stopping or changing the medication quickly can help the liver heal and prevent serious damage. The study looked at a case where a person had a history of TB in the abdomen and focused on the signs, symptoms, and challenges of dealing with liver issues caused by TB treatment.
Case Report
A 61-year-old woman came in with yellowing of her eyes for one week, a swollen abdomen for four days, low appetite, tiredness, body aches, and yellow-colored urine. She had a history of diabetes and peritoneal tuberculosis, and she was on medicines for diabetes and anti-tuberculosis treatment for four months. Her liver function tests were normal in the second month, but started increasing in the third month (ALP 204U/L, SGPT 38U/L, SGOT 132U/L) and even more in the fourth month (ALP 366U/L, SGPT 45U/L, SGOT 139U/L). Because of this, she stopped the anti-tuberculosis treatment 10 days before she was admitted. She had no history of drinking alcohol, smoking, or any drug allergies. Her vital signs were stable during the exam. Lab results showed a high white blood cell count (17,800), normal platelets (4.85 lakhs), urea (51), creatinine (1.07), low sodium (120), and low potassium (2.8). The fluid around her abdomen had low glucose (59 mg\dl), low ADA (2.83 g/dl), some white blood cells (420, mostly lymphocytes), and some red blood cells (910). The fluid didn’t show any cancer cells under the microscope. A CT scan of her abdomen found a slightly enlarged liver with some fat, gallstones, and fluid in the abdomen. A contrast CT scan suggested possible cancer in the bile ducts or gallbladder with spread to the liver and abdomen. Blood tests showed normal AFP and CEA levels, but a very high CA19-9 level (7208 U/mL). The final diagnosis considered liver injury from the anti-tuberculosis drugs, along with possible cholangiocarcinoma or gallbladder cancer, and also peritoneal tuberculosis and electrolyte imbalance. She was treated with intravenous N-acetylcysteine, pantoprazole, ondansetron, ursodeoxycholic acid, liver-protecting medicines (Maxiliv, Heptral), lactulose syrup, potassium and magnesium sulfate, and other supportive treatments.
Table 1: Drug Regimen Table
|
Drug Prescribed |
Generic Name |
Dose |
Frequency |
Route of Administration |
|
Inj. Pantop |
Pantoprazole |
40mg |
OD |
IV |
|
Inj. Zofer |
Ondansetron |
4mg |
BD |
IV |
|
Tab. Udiliv |
Ursodeoxycholic acid |
300mg |
TID |
P\O |
|
Tab. Heptral |
Ademetionine |
400mg |
BD |
P\O |
|
Inj. Maxiliv |
Glutathione |
600mg |
BD |
IV |
|
Syrup. Duphlac |
Lactulose |
5ml |
BD |
P\O |
|
Syrup. Sucralfate |
Sucralfate |
3ml |
TID |
P\O |
|
Inj. Nacfil |
Acetylcysteine |
2ml |
OD |
IV |
|
Kcl+mgso4 |
Kcl+mgso4 |
40ml |
QID |
IV |
DISCUSSION
Drug-induced liver injury (DILI) is a major problem in clinical practice and a common reason why patients stop their anti-tuberculosis treatment (ATT). Drugs like isoniazid, rifampicin, and pyrazinamide are known to cause liver damage, and the rate of this happening ranges from 5% to 28%. In countries where tuberculosis is prevalent, like India, the effects of DILI from ATT are even more serious because of the high number of people with tuberculosis and other health issues, such as diabetes, poor nutrition, and viral hepatitis. This shows the importance of closely watching patients to prevent complications and keep their treatment going.
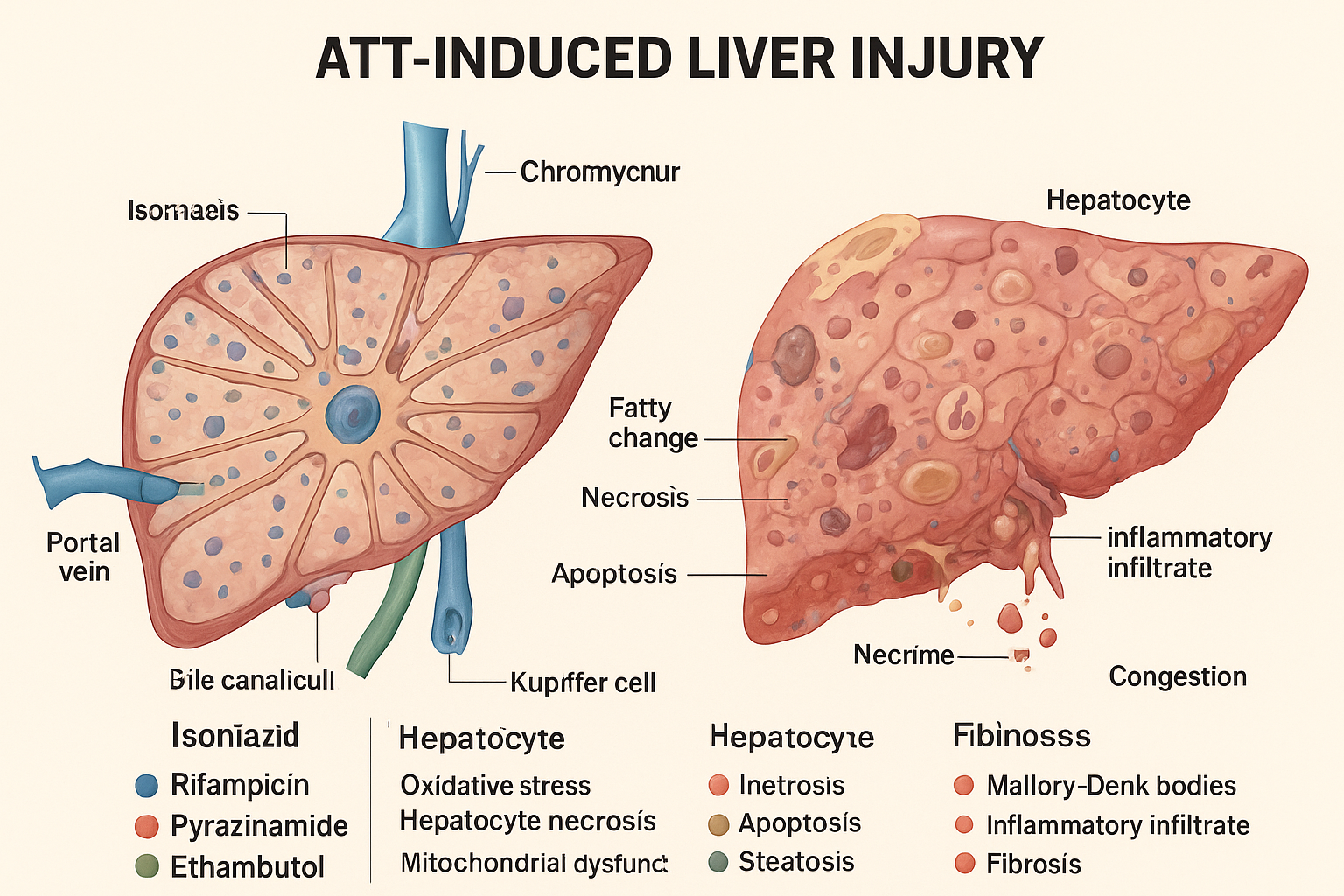
Figure 1: ATT-Induced Liver Injury and Related Pathological Changes.
A recent case of a 61-year-old woman with diabetes and peritoneal tuberculosis highlights how complicated ATT-related liver damage can be. Her liver function tests were normal at first, but after two months of treatment, they showed a big increase. The presence of high levels of CA 19-9 and imaging results that suggested possible cholangiocarcinoma or gallbladder cancer made it hard to know the exact cause. But by carefully looking at her medical history, lab results, and imaging, we were able to rule out other possibilities and confirm that the liver damage was due to the drugs. This case shows how important it is to do a thorough and organised assessment and to use evidence-based approaches. Quickly stopping the harmful drugs, giving N-acetylcysteine and other liver-protecting medicines, and providing support helped her liver function improve and avoided the need for more invasive tests. However, without a liver biopsy to confirm the cause and without proper guidelines to safely test which drug is responsible, it was hard to link the liver damage to each ATT drug definitively. As a single case, the results are useful but not enough to apply broadly. This case also shows the need for regular liver function tests, especially for patients who are at higher risk. Tumour markers should be considered in conjunction with other clinical and imaging information to avoid a misdiagnosis. When DILI occurs, stopping the harmful drugs, providing support, and carefully reintroducing necessary medications under close watch is key. Using a team of specialists can help get an accurate diagnosis and improve patient outcomes in these difficult cases.
CONCLUSION
Drug-induced liver injury can seriously affect the success of treatment for tuberculosis, especially in patients who are at higher risk. It is important to identify this early, regularly check the liver function, and act quickly with proven treatments to stop permanent damage and keep the treatment going. Using a team of different specialists helps in better diagnosis, reduces health problems, and ensures that effective treatments work properly.
REFERENCE


Sumaiya Fatima*, Azka Fathima, Case Report: ATT-Induced Hepatotoxicity in Peritoneal Tuberculosis, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 2849-2853 https://doi.org/10.5281/zenodo.17193322
 10.5281/zenodo.17193322
10.5281/zenodo.17193322
