Department of Pharmaceutics, Rajgad Dnyanpeeth’s College of Pharmacy Bhor, Pune
Neurodegenerative disorders such as Parkinson’s disease, Alzheimer’s disease, and related dementias remain difficult to treat because many therapeutic agents show poor penetration across the blood–brain barrier (BBB) and require long-term administration. Intranasal (IN) administration offers a non-invasive route for direct drug transport from the nasal cavity to the central nervous system (CNS) through olfactory and trigeminal pathways, partially bypassing systemic circulation and the BBB. However, mucociliary clearance, limited dosing volume, enzymatic degradation, and poor solubility of many neuroprotective molecules reduce delivery efficiency. Cubosomes—nanostructured particles derived from bicontinuous cubic liquid crystalline phases—have emerged as a versatile lipid-based platform capable of encapsulating hydrophilic, lipophilic, and amphiphilic payloads, enabling sustained release and improved mucosal permeation. This review summarizes the fundamentals of cubosome structure and composition (monoolein or phytantriol with stabilizers such as poloxamer 407), preparation approaches (top-down, bottom-up), critical quality attributes, and performance considerations for intranasal nose-to-brain delivery. Evidence from preclinical studies of cubosomal intranasal systems—often incorporated into in situ mucoadhesive gels—demonstrates improved brain targeting, enhanced pharmacodynamic outcomes, and acceptable nasal safety for multiple CNS-active drugs. Key design considerations, evaluation models, translational challenges, and future directions (surface functionalization, scalable manufacturing, regulatory quality-by-design) are discussed to guide development of clinically relevant cubosomal nose-to-brain neuroprotective therapies.
The burden of neurodegenerative diseases is rising globally, driven by aging populations and limited availability of disease-modifying interventions. A core obstacle in CNS drug development is achieving adequate drug concentration at target brain regions without systemic toxicity. The BBB, formed by tight junctions between endothelial cells along with efflux transporters and metabolic enzymes, restricts passage of most small molecules and nearly all biologics. Consequently, many neuroprotective candidates fail in translation despite promising in vitro activity. Alternative administration routes and carrier systems are being developed to enhance brain exposure, including intrathecal delivery, focused ultrasound BBB opening, and intranasal nose-to-brain transport.
Intranasal administration has gained attention as a patient-friendly route capable of delivering drugs directly to the CNS along olfactory and trigeminal neural pathways. Nevertheless, only a fraction of a dose typically reaches the brain because of mucociliary clearance, limited residence time, and constraints on formulation volume and viscosity. Nanocarriers can mitigate these limitations by improving solubility, protecting labile molecules, enhancing mucosal interaction, and enabling controlled release. Among lipid nanocarriers, cubosomes offer a unique internal architecture with high surface area and tortuous aqueous channels that can host diverse therapeutics. When tailored for intranasal use—commonly by embedding cubosomes within mucoadhesive in situ gels—these systems can prolong nasal retention and support nose-to-brain transport of neuroprotective agents.
2. Nose-to-Brain Delivery: Anatomy, Pathways, and Barriers
2.1 Nasal cavity regions relevant to CNS transport
The nasal cavity contains respiratory and olfactory regions. The respiratory epithelium provides a large vascularized surface for systemic absorption, while the olfactory epithelium (upper posterior nasal cavity) is directly connected to the olfactory bulb via olfactory neurons. The trigeminal nerve innervates both regions and projects to brainstem structures. Formulation deposition location (anterior vs posterior; respiratory vs olfactory) strongly influences whether a payload primarily enters systemic circulation or achieves direct nose-to-brain transport.
2.2 Mechanisms of N2B transport
N2B delivery occurs via multiple, partially overlapping mechanisms: (i) extracellular transport along perineural channels surrounding olfactory or trigeminal nerves; (ii) intracellular axonal transport following uptake into neurons; (iii) transport through epithelial tight junctions (paracellular) or via transcytosis (transcellular); and (iv) entry into cerebrospinal fluid (CSF) and subsequent distribution. The extracellular perineural route is often considered faster (minutes to hours) than axonal transport (hours to days). Nanocarriers may enhance epithelial uptake and protect drugs from enzymatic degradation, but size, surface charge, and mucoadhesion must be balanced to avoid excessive clearance or irritation.
2.3 Key formulation limitations for intranasal delivery
Limited administration volume (typically ~100–200 µL per nostril in adults) requiring potent drugs or concentrated formulations.
Mucociliary clearance reducing residence time (often 15–30 minutes) for conventional solutions/suspensions.
Enzymatic activity in nasal mucus and epithelium (peptidases, esterases) impacting labile molecules.
Variability due to nasal physiology (rhinitis, infections), dosing technique, and anatomical differences.
Local safety constraints: pH, osmolarity, preservatives, and excipient irritation must be controlled.
3. Cubosomes: Fundamentals and Rationale for Neuroprotection
3.1 Definition and structural characteristics
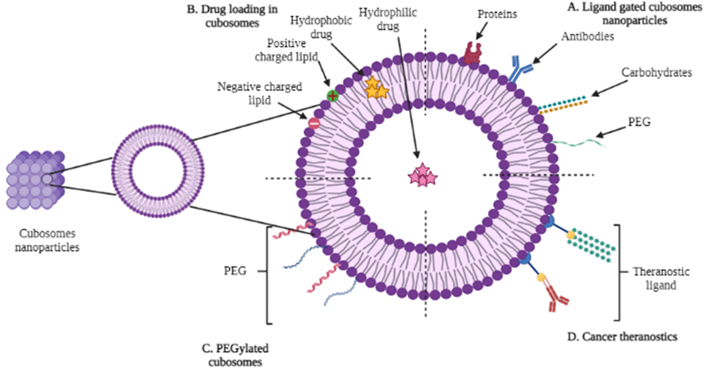
Cubosomes are colloidal nanoparticles formed by dispersing a bicontinuous cubic liquid crystalline phase in an aqueous medium. Their internal structure consists of a lipid bilayer separating two interpenetrating aqueous networks organized in a periodic cubic geometry (commonly Pn3m or Im3m). This architecture provides (i) high internal surface area, (ii) the ability to co-load hydrophilic (within aqueous channels) and lipophilic (within lipid bilayer) molecules, and (iii) diffusion-controlled, sustained release due to tortuous pathways. Cubosomes are often composed of monoolein (glyceryl monooleate, GMO) or phytantriol, stabilized with non-ionic polymers such as poloxamer 407 (Pluronic F127).
3.2 Why cubosomes are attractive for intranasal brain targeting
High drug-loading versatility for molecules with diverse physicochemical properties.
Sustained/controlled release that can reduce dosing frequency and smooth brain exposure profiles. Bioadhesive and membrane-interacting lipid composition that can improve mucosal permeation. Protection of labile drugs from degradation and potential improvement of apparent solubility. Compatibility with in situ gelling/mucoadhesive systems to extend nasal residence time.
3.3 Cubosomes versus other lipid nanocarriers
Compared with liposomes, cubosomes generally offer higher structural stability and sustained release due to their non-lamellar internal phase. Compared with solid lipid nanoparticles, cubosomes provide an internal bicontinuous network suitable for higher loading of hydrophilic agents and can avoid drug expulsion during lipid crystallization. Selection among carriers should consider payload solubility, desired release rate, scalability, and safety profile.
4. Materials for Cubosome Formulation
4.1 Lipid matrix formers
The most widely used cubosome-forming lipids are monoolein (GMO) and phytantriol. GMO is biodegradable and forms stable cubic phases upon hydration, while phytantriol can yield robust cubic phases with distinct phase behavior and sometimes improved chemical stability. Lipid purity and water content influence phase formation and reproducibility.
4.2 Stabilizers and surfactants
Stabilizers prevent aggregation and maintain colloidal stability. Poloxamer 407 (Pluronic F127) is commonly used because it adsorbs at the particle surface and provides steric stabilization. Other stabilizers include poloxamer 188, Tween surfactants, PEGylated lipids, and novel amphiphiles (including gemini surfactants) designed to enhance stability under physiological conditions.
4.3 Functional excipients for intranasal systems
Table 1. Typical composition of intranasal cubosomal formulations (illustrative ranges)
|
Component |
Examples |
Typical range |
Role in formulation |
|
Cubic-phase lipid |
Monoolein (GMO), phytantriol |
2–15% w/v (dispersion) |
Forms bicontinuous cubic phase; controls encapsulation and release |
|
Stabilizer |
Poloxamer 407 (F127), Poloxamer 188, Tween 80 |
0.2–2% w/v |
Steric stabilization; prevents aggregation; influences size |
|
Mucoadhesive polymer |
Chitosan, Carbopol, HPMC, sodium alginate |
0.1–1% w/v |
Increases nasal residence; may enhance permeation |
|
In situ gelling agent |
Poloxamer blends, gellan gum, pectin |
0.2–20% w/v (agent-dependent) |
Sol-to-gel transition for easy dosing and prolonged retention |
|
Buffer/tonicity agents |
Phosphate buffer, NaCl |
q.s. |
Controls pH and osmolarity for nasal comfort and stability |
Mucoadhesive polymers: chitosan, Carbopol, HPMC, sodium alginate to prolong residence time.
In situ gelling agents: poloxamers, gellan gum, pectin for temperature- or ion-triggered gelation.
Tonicity and pH modifiers: sodium chloride, phosphate buffers to match nasal physiology.
Preservatives/antioxidants: only when necessary; must be screened for nasal safety.
5. Preparation Methods for Cubosomes
5.1 Top-down approach
In the top-down method, a bulk cubic gel (formed by hydrating lipid with aqueous phase) is fragmented into nanoparticles using high-energy input such as probe sonication or high-pressure homogenization, in the presence of stabilizer. This method is widely used in laboratories and can produce nanosized dispersions, but it may be energy-intensive and may induce temperature rise, potentially affecting heat-sensitive drugs.
5.2 Bottom-up approach
In bottom-up methods, cubosomes form spontaneously from molecular precursors by controlled dilution or solvent displacement. Lipid is dissolved in a hydrotrope or solvent system and then added to aqueous stabilizer, allowing self-assembly into cubic nanoparticles. Bottom-up strategies can reduce energy requirements and may be more scalable, but careful control of solvent removal, residuals, and phase behavior is needed.
5.3 Process variables impacting quality
Lipid-to-stabilizer ratio (affects size, stability, and internal structure).
Energy input (sonication time/amplitude, homogenization pressure/cycles).
Temperature during processing (phase transitions; drug degradation risk). Order of addition and hydration conditions (reproducibility of cubic phase). Post-processing (filtration, sterilization approach, storage conditions).
6. Characterization and Critical Quality Attributes (CQAs)
6.1 Particle size, PDI, and colloidal stability
Particle size influences nasal deposition, uptake, and clearance. For many intranasal applications, sizes in the ~100–300 nm range are commonly targeted. A low PDI indicates uniformity, supporting reproducible performance and stability. Zeta potential provides insight into electrostatic stability and potential mucosal interaction; however, many sterically stabilized cubosomes exhibit modest zeta potential while remaining stable.
6.2 Internal nanostructure and phase confirmation
Because cubosome performance depends on its bicontinuous cubic phase, structural confirmation is critical. SAXS is the gold standard for identifying cubic space groups (Pn3m, Im3m) and lattice parameters. Cryo-TEM and freeze-fracture TEM provide complementary visualization of internal periodicity. Differential scanning calorimetry (DSC) can assess thermal behavior and drug-lipid interactions.
6.3 Encapsulation metrics and release/permeation testing
Encapsulation efficiency (EE%) and drug loading should be quantified using validated analytical methods (HPLC/UV). In vitro release should be designed to avoid sink limitations and to capture diffusion-controlled kinetics (e.g., dialysis methods with appropriate controls). Ex vivo permeation across excised nasal mucosa (e.g., sheep/goat) provides mechanistic insight, but must be interpreted with species differences and tissue viability considerations. Mucoadhesion testing (texture analyzer/mucin interaction) is important for gels or mucoadhesive coatings.
Table 2. Practical CQAs for intranasal cubosomal systems and their significance
|
CQA |
Typical methods |
Why it matters for N2B delivery |
|
Particle size & PDI |
DLS, nanoparticle tracking analysis |
Influences deposition, cellular uptake, and clearance; affects reproducibility |
|
Zeta potential |
Electrophoretic mobility |
Affects stability and interaction with mucus/epithelium |
|
Cubic phase confirmation |
SAXS, cryo-TEM |
Ensures intended internal structure and release behavior |
|
Drug loading/EE% |
Centrifugation/filtration + HPLC/UV |
Determines dose deliverable within nasal volume limits |
|
Rheology/gelation (if gel) |
Viscometry, gelation temperature/ion response |
Controls retention, sprayability, and patient acceptability |
|
In vitro release |
Dialysis, Franz diffusion |
Predicts sustained delivery and informs kinetic modeling |
|
Ex vivo permeation |
Nasal mucosa diffusion studies |
Approximates mucosal transport potential and formulation effects |
|
Nasal safety |
Histopathology, ciliary beat frequency, irritation tests |
Critical for chronic use; limits excipient choices |
7. In Situ Gels and Mucoadhesive Strategies for Cubosomal N2B Delivery
To overcome rapid mucociliary clearance, cubosomal dispersions are frequently incorporated into in situ gels that undergo sol-to-gel transition upon exposure to nasal conditions (temperature, pH, or ions). This approach enables easy administration as a low-viscosity liquid followed by formation of a more viscous gel that resists clearance. Mucoadhesive polymers further strengthen interaction with nasal mucus through ionic interactions, hydrogen bonding, or chain entanglement.
7.1 Thermoresponsive gels
Poloxamer-based systems gel at nasal temperature, enabling convenient dosing. Blends of poloxamer 407 with poloxamer 188 are used to tune gelation temperature and viscosity. However, high poloxamer content may cause irritation or drainage in some cases, and formulation must balance gelation with comfort and sprayability.
7.2 Ion-activated and pH-responsive gels
Gellan gum and pectin can gel in the presence of cations in nasal fluid, while carbopol-based systems can exhibit pH-dependent viscosity changes. These systems may achieve strong retention at relatively low polymer concentration. Compatibility with cubosomes must be validated to avoid destabilization or phase transition.
8. Evidence for Cubosomal Nose-to-Brain Delivery in Neurotherapeutics
A growing body of preclinical research supports the feasibility of cubosomal intranasal delivery for CNS targeting. Studies commonly report nanoscale particle size, high entrapment efficiency, sustained release, enhanced ex vivo permeation, and improved brain pharmacokinetics or pharmacodynamics compared with drug solution. Many studies embed cubosomes in mucoadhesive in situ gels and evaluate brain targeting metrics such as brain-to-plasma ratios, drug targeting efficiency (DTE), and direct transport percentage (DTP).
Table 3. Representative intranasal cubosomal systems evaluated for brain targeting
|
Drug/payload |
Cubosome lipid & stabilizer |
Dosage form |
Key findings (summary) |
Model(s) |
|
Resveratrol |
GMO + Poloxamer F127 |
Cubosomal in situ nasal gel |
Optimized nanosized cubosomes; improved brain targeting in vivo vs control; sustained release |
Rat (in vivo); ex vivo nasal |
|
Granisetron |
GMO-based cubosomes (optimized) + polymer |
In situ mucoadhesive gel |
Enhanced brain delivery through N2B route; optimized formulation via design; improved permeation |
Ex vivo; in vivo biodistribution |
|
Verapamil HCl |
GMO + Poloxamer 407 |
Cubosomal gel for intranasal |
High brain targeting efficiency and direct transport %; sustained release; nasal safety |
Ex vivo; in vivo brain biodistribution |
|
Tizanidine HCl |
GMO-based cubosomes |
Intranasal cubosomal spray/gel |
Improved CNS delivery compared to solution; optimized cubosomes with favorable size/EE |
In vivo (pharmacokinetic/PD) |
9. Neuroprotection Applications: Design Considerations
9.1 Oxidative stress and inflammation as common targets
Oxidative stress, mitochondrial dysfunction, excitotoxicity, and neuroinflammation are central features of many neurodegenerative diseases. Neuroprotective agents (polyphenols, antioxidants, anti-inflammatory drugs, neurotrophic factors, peptides, nucleic acids) frequently face delivery limitations due to poor solubility or instability. Cubosomes can improve apparent solubility for lipophilic antioxidants and protect labile payloads within aqueous channels or the lipid bilayer.
9.2 Selecting cubosome architecture for payload class
Lipophilic small molecules (e.g., polyphenols): favor lipid bilayer partitioning; consider antioxidant protection and release modulation.
Hydrophilic small molecules/peptides: may reside in aqueous channels; evaluate leakage and stability in nasal fluids.
Biologics (proteins/siRNA): require protection from enzymes and often benefit from mucoadhesive/permeation-enhancing coatings (e.g., chitosan).
Combination therapy: cubosomes may co-encapsulate synergistic agents, but compatibility and release synchronization must be tested.
10. Safety, Tolerability, and Regulatory Considerations
For chronic neurodegenerative therapy, local nasal safety is essential. Formulations should be isotonic or near-isotonic, with pH compatible with nasal mucosa (commonly ~5.0–6.5) and minimal irritants. Lipid excipients such as GMO and stabilizers like poloxamer 407 have a history of pharmaceutical use, but intranasal-specific safety must still be established, including effects on ciliary function, epithelial integrity, and inflammatory markers. Histopathology of nasal mucosa after repeated dosing is commonly used in preclinical safety evaluation. From a regulatory perspective, cubosomes are complex drug–product systems that require robust characterization and control. A QbD framework is well-suited: identify critical material attributes (lipid purity, polymer grade), critical process parameters (energy input, temperature), and CQAs (size, structure, EE, release). Scalable manufacturing (high-pressure homogenization; solvent-free bottom-up approaches) and sterilization strategies (aseptic processing, filtration where feasible) should be considered early.
11. Translational Challenges and Future Directions
Targeted deposition to the olfactory region remains challenging; device engineering and patient technique influence outcomes.
Species differences in nasal anatomy complicate extrapolation from rodents to humans; larger-animal models and imaging-based biodistribution can help. Long-term safety and immunogenicity data are limited for repeated intranasal nanoparticle administration. Scale-up requires control of cubic phase structure and particle size distribution under industrial processing conditions.
Future work: ligand-functionalized cubosomes for receptor-mediated uptake, mucus-penetrating coatings, and integration with in vivo imaging for mechanistic validation.
CONCLUSION
Cubosomes represent a promising lipid-based nanoplatform for intranasal nose-to-brain delivery of neuroprotective agents. Their bicontinuous cubic architecture supports versatile drug loading and sustained release, while formulation into mucoadhesive in situ gels can enhance nasal residence time and improve the likelihood of direct brain transport. Preclinical studies demonstrate improved brain targeting and therapeutic outcomes for multiple CNS drugs, suggesting that cubosomal systems may help bridge the gap between potent neuroprotective molecules and effective CNS exposure. Continued progress will depend on rigorous structural characterization, standardized in vivo evaluation, scalable manufacturing, and comprehensive nasal safety assessment.
REFERENCES


Anurag Gaikwad, K. Kore, Dhanashree Jarande, Cubosomal Drug Delivery Systems for Neuroprotection via Nose-to-Brain Delivery: A Detailed Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 4576--4586. https://doi.org/10.5281/zenodo.18811933
 10.5281/zenodo.18811933
10.5281/zenodo.18811933
