New Montfort Institute of Pharmacy Ashti Wardha.
Sustained-release matrix tablet formulations have become a key strategy for optimizing therapeutic efficiency, minimizing dosing frequency, and enhancing patient compliance. This study focuses on the formulation and evaluation of sustained-release matrix tablets of captopril, an angiotensin-converting enzyme (ACE) inhibitor with a short half-life, to achieve prolonged and controlled release. The tablets were developed using hydrophilic and hydrophobic polymers such as Hydroxypropyl Methylcellulose (HPMC K-100), Xanthan Gum, and Ethyl Cellulose, through direct compression. Various pre- and post-compression parameters were evaluated, including flowability, hardness, friability, drug content uniformity, and in vitro dissolution. Spectroscopic analyses (FTIR and UV) confirmed compatibility of the drug with excipients. In vitro release studies revealed that the optimized formulation sustained drug release for up to 12 hours, following Higuchi and Korsmeyer–Peppas diffusion-controlled kinetics. The results demonstrate that polymeric matrix tablets can provide predictable and consistent drug release, improve bioavailability, and reduce dosing frequency for effective management of hypertension and cardiac failure.
Oral drug delivery remains the most preferred route of administration owing to patient convenience, safety, and flexibility in dosage design. However, traditional dosage forms often fail to maintain consistent plasma drug concentrations, resulting in sub-therapeutic or toxic levels. Sustained-release (SR) formulations are designed to overcome these limitations by controlling drug release over an extended period, thereby maintaining therapeutic levels within the target range (Chien, 2007; Aulton, 2007).
In sustained-release systems, the rate and extent of drug release are governed by the nature and concentration of polymers used in the matrix. The fundamental objective of such formulations is to achieve a steady-state concentration that ensures optimal therapeutic response and reduces dosing frequency (Mandal et al., 2007). Matrix tablets, among SR systems, are particularly popular due to their simplicity, stability, and cost-effectiveness.
Historically, the concept of solid dosage forms dates back to around 1500 BC when early Egyptians first documented the use of medicinal tablets. Over time, coating techniques and polymer sciences revolutionized dosage design, allowing modification of release profiles and enhancement of stability (Jain, 2001).
The novel drug delivery systems (NDDS) integrate principles of polymer chemistry and biopharmaceutics to provide spatial and temporal control over drug release, enhancing therapeutic efficacy and minimizing side effects. Sustained-release tablets are therefore advantageous for chronic conditions requiring long-term therapy, such as hypertension, diabetes, and arthritis.
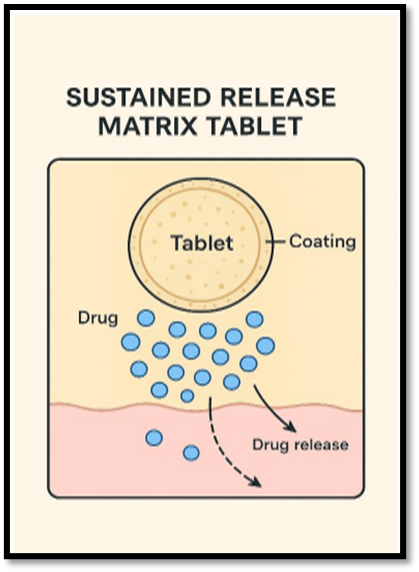
Figure No.1: Mechanism of Drug Release from Sustained Release Matrix Tablet.
1.1 Concept and Terminology
Various terms such as sustained release, prolonged release, extended release, and controlled release are often used interchangeably.
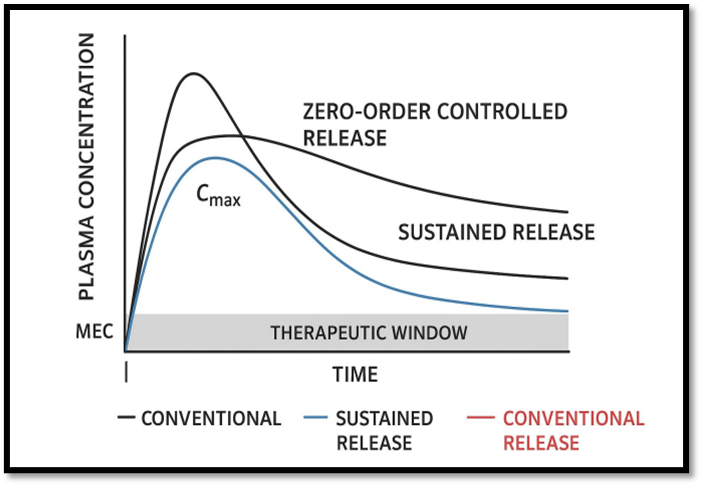
Fig No: 2 Plasma drug concentration vs. time profile for oral conventional dosing and single oral dose of sustained and controlled release formulation.
1.2 Biopharmaceutical Considerations
Designing an SR dosage form requires careful analysis of the drug’s physicochemical and pharmacokinetic properties (Brahmankar & Jaiswal, 2019). Important factors include:
Captopril, a short half-life drug (t½ ≈ 2 hours), is an ideal candidate for sustained release, offering the potential to minimize dosing frequency and maintain therapeutic plasma levels.
1.3 Role of Polymers in Sustained Release Systems
Polymers are central to the design of SRDDS, influencing drug diffusion, dissolution, and erosion rates:
Figure No. 3: Classification of Sustained Release Matrix Tablet
1.4 Mechanism of Drug Release
Drug release from matrix systems occurs primarily through diffusion, erosion, and swelling mechanisms.
ig no. 4: A. Diffusion Type Reservoir System, B. Diffusion Matrix Type System, c. Soluble Reservoir System, D. Soluble Matrix System.
2. Literature Review
Extensive research has been conducted on sustained release systems, particularly on matrix tablet design and optimization.
3. MATERIALS AND METHODS
3.1 MATERIALS
3.2 Method of Preparation
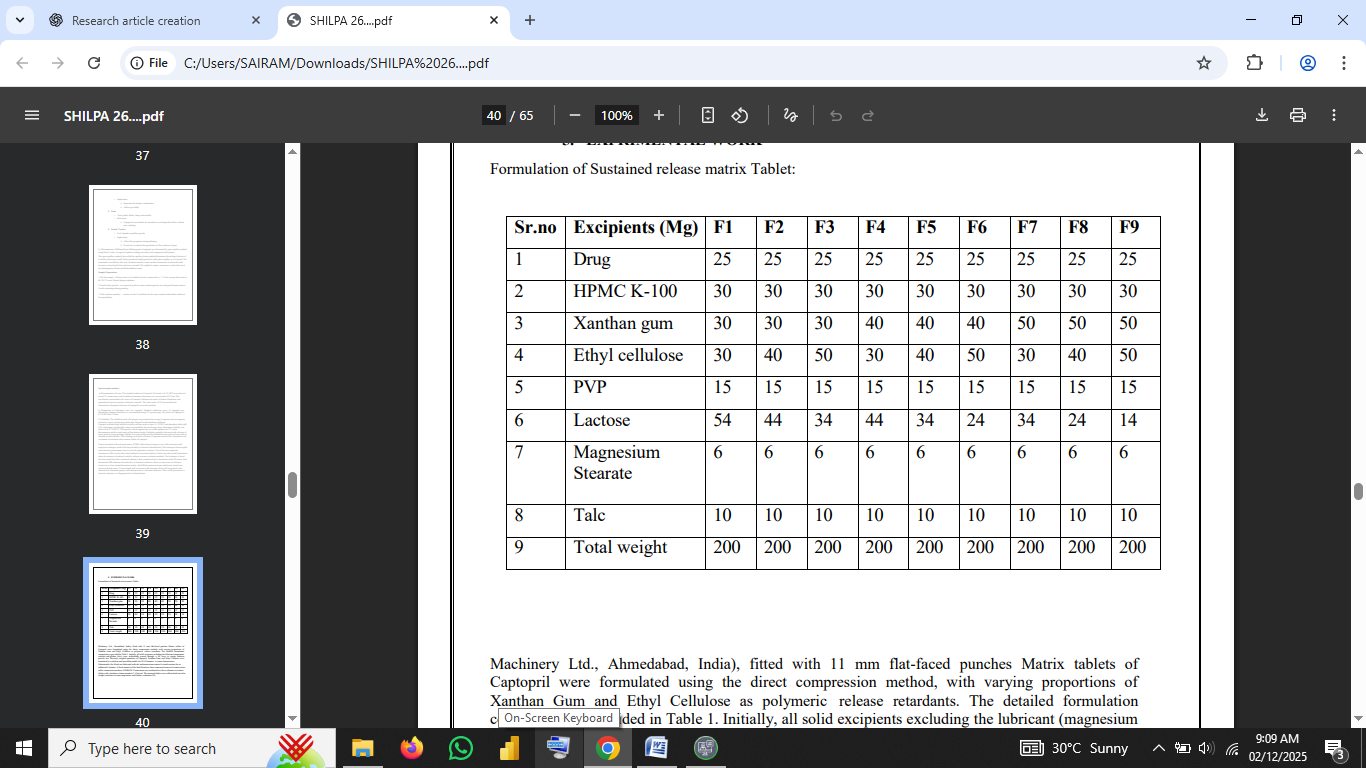
Matrix tablets of Captopril were prepared by the direct compression method using varying ratios of hydrophilic (Xanthan gum, HPMC K-100) and hydrophobic (Ethyl cellulose) polymers as release retardants.
Each tablet weighed 200 mg and was stored in airtight containers at room temperature until evaluation.
Table no 1: Formulation Composition of Matrix Tablets (F1–F9)
3.3 Characterization of Drug
Organoleptic Properties: Captopril appears as a white to off-white crystalline powder with a characteristic sulfur-like odor and bitter taste.
Melting Point: 105–108 °C (open capillary method).
Solubility: Freely soluble in water and 0.1 N HCl; sparingly soluble in ethanol and chloroform.
λmax Determination: 212 nm in 0.1 N HCl (Chien, 2007).
FTIR Compatibility: Characteristic peaks at ~1718 cm?¹ (C=O stretch), 2550 cm?¹ (SH group), and 1610 cm?¹ (N–H bend) were retained in the physical mixture, confirming no drug–polymer interaction.
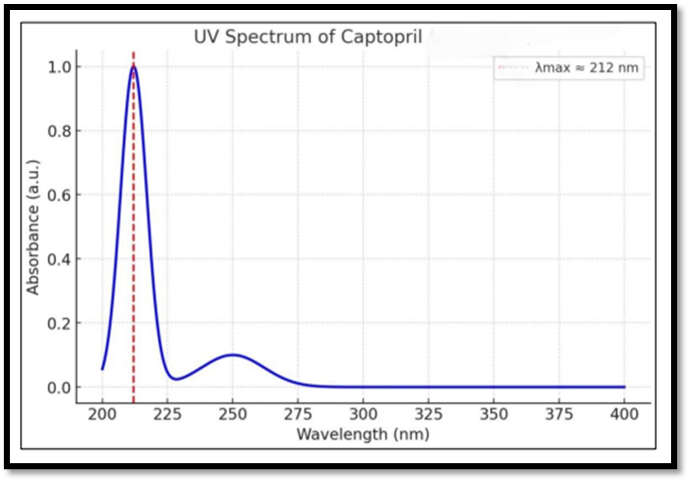
Fig No.5: UV spectrum of Captopril in phosphate buffer (pH 7.4).
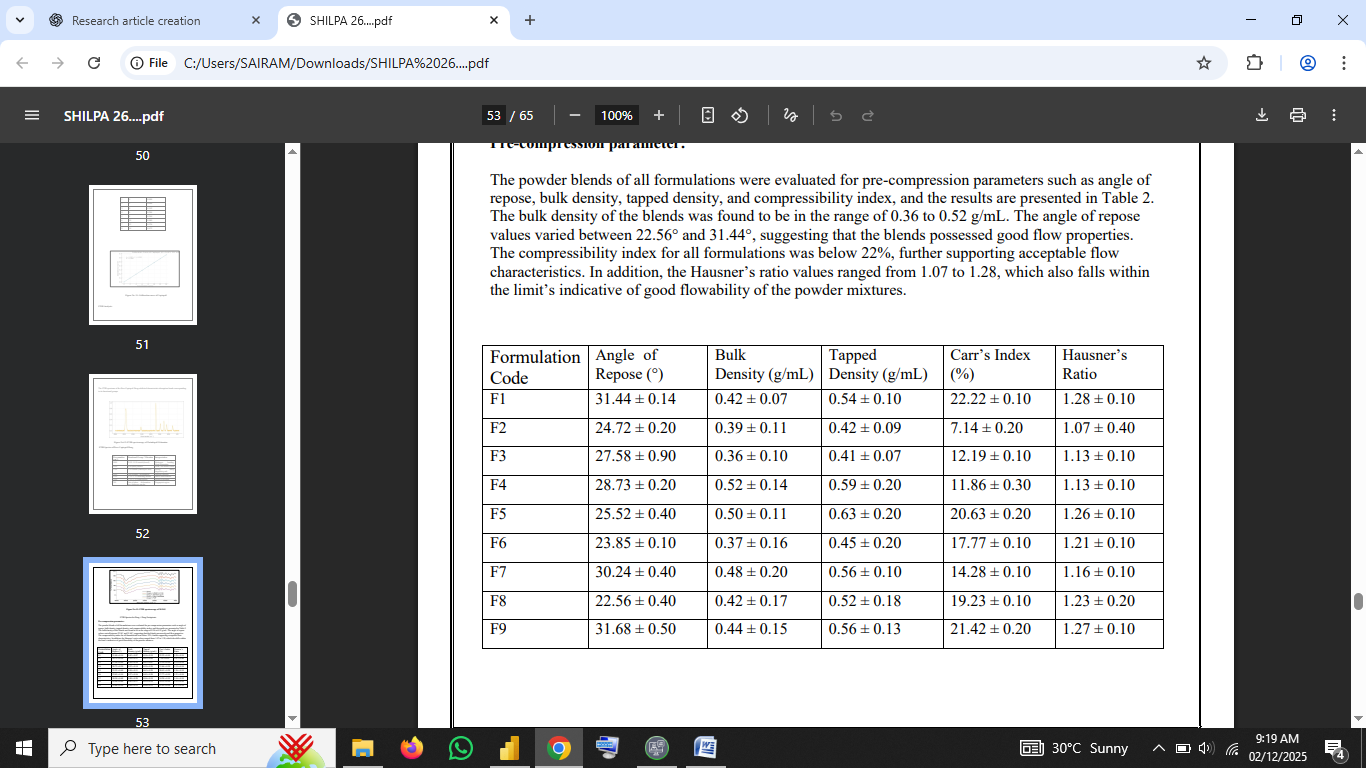
3.4 Pre-Compression Evaluation
The powder blend was evaluated for:
|
Parameter |
Formula |
Significance |
|
Bulk Density |
Mass / Bulk Volume |
Indicates packing behavior |
|
Tapped Density |
Mass / Tapped Volume |
Predicts compressibility |
|
Carr’s Index (%) |
((TD − BD)/TD) × 100 |
Flow property indicator |
|
Hausner’s Ratio |
TD / BD |
Flow index |
|
Angle of Repose |
tan θ = h/r |
Measures flowability |
All formulations showed Carr’s Index < 15% and Hausner’s Ratio < 1.25, indicating excellent flow and compressibility.
Table no 2: Pre-Compression Parameters for Formulations F1–F9
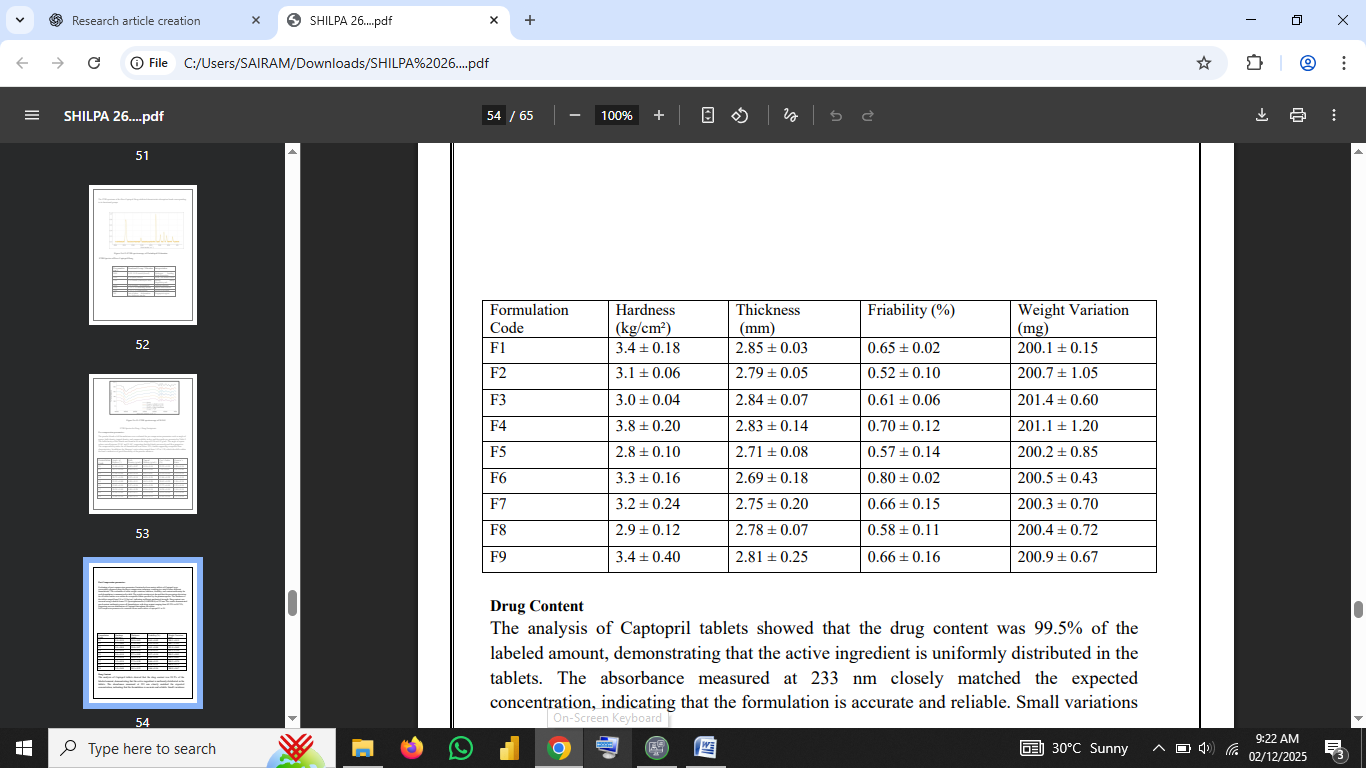
3.5 Post-Compression Evaluation
The tablets were evaluated for:
Table no.3: Post-Compression Evaluation Results
3.6 Swelling and Disintegration Studies
Swelling index was determined by weighing tablets before and after hydration in distilled water at 37 ± 0.5 °C. Formulations containing HPMC and Xanthan gum showed gradual swelling, forming a gel barrier that controlled release. Disintegration times ranged from > 4 h to > 12 h depending on polymer concentration.
3.7 In Vitro Dissolution Study
The drug release from each formulation was evaluated using USP Apparatus II (paddle method) in 900 mL of 0.1 N HCl (pH 1.2) at 37 ± 0.5 °C and 50 rpm. Samples were withdrawn at regular intervals (0.5–12 h), filtered, and analyzed at 212 nm.
The optimized formulation (F7) demonstrated a controlled release profile with ≈ 95 % drug released within 12 hours. Formulations F1–F3 showed faster release due to lower polymer content, while F8 and F9 retarded release beyond 12 h due to excess hydrophobic matrix.
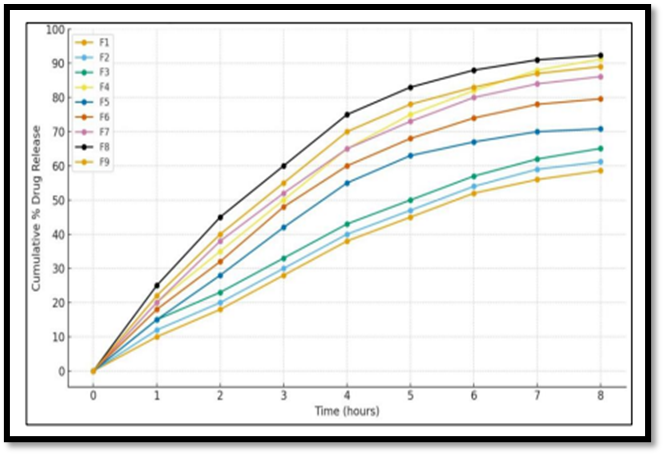
Fig no. 6: Dissolution profile of Captopril Sustained release matrix tablet for F1-F9 batches
3.8 Kinetic Modeling
Drug release data were fitted to various mathematical models to determine mechanism of release:
|
Model |
Equation |
Interpretation |
|
Zero Order |
Q? = Q? + K?t |
Constant release rate |
|
First Order |
log Q? = log Q? + Kt/2.303 |
Concentration-dependent |
|
Higuchi Model |
Q = K_H t¹?² |
Diffusion through matrix |
|
Korsmeyer-Peppas |
Mt/M∞ = K t? |
Mechanism based on n-value |
The correlation coefficients (R²) indicated that the optimized batch followed Higuchi diffusion kinetics (R² ≈ 0.987) and the Peppas model with n < 0.5, implying Fickian diffusion (Venkatraman et al., 2000).
3.9 Stability Studies
Stability testing was performed as per ICH guidelines (Q1A R2) on the optimized formulation (F7) at 40 ± 2 °C / 75 ± 5 % RH for three months. Samples were evaluated at 0, 30, 60, and 90 days for appearance, hardness, drug content, and dissolution. No significant changes were observed (p > 0.05), indicating excellent stability under accelerated conditions.
Table no 5: Stability Study Data for Optimized Batch (F7)
|
Parameter |
Initial |
After 30 days |
After 60 days |
After 90 days |
|
Appearance |
No change |
No change |
No change |
No change |
|
Hardness (kg/cm²) |
3.8 ± 0.2 |
3.7 ± 0.3 |
3.8 ± 0.2 |
3.7 ± 0.3 |
|
Drug content (%) |
100.2 ± 0.6 |
99.8 ± 0.7 |
99.4 ± 0.8 |
99.0 ± 0.7 |
|
% Cumulative Drug Release (12 h) |
95.2 |
94.6 |
94.0 |
93.7 |
Storage conditions: 40 ± 2 °C / 75 ± 5 % RH (Accelerated Stability, ICH Q1A Guidelines)
4. Results and Observations
4.1 Pre-Compression Findings
All powder blends exhibited good flow properties: bulk density (0.47–0.55 g/cm³), tapped density (0.55–0.63 g/cm³), Carr’s Index (8.3–12.5 %), and Hausner’s Ratio (1.09–1.14). This ensured uniform die filling and consistent tablet weight (Agarwal et al., 2017).
4.2 Post-Compression Results
Tablets were mechanically strong with friability < 1 % and uniform weight (± 2.5 %). Drug content ranged from 98.7 to 101.5 %. The uniform thickness and hardness values indicated satisfactory compression force and die filling during manufacture.
4.3 In Vitro Drug Release
Release rate was found to be polymer concentration-dependent. Formulations with higher Xanthan gum and Ethyl cellulose content retarded release significantly compared to lower ratios. Formulation F7 (HPMC K-100 + Xanthan gum 50 mg + Ethyl cellulose 40 mg) achieved controlled release for 12 hours with a smooth diffusion profile (Chauhan et al., 2012).
4.4 Kinetic Evaluation
The in-vitro release data for each formulation were fitted to zero-order, first-order, Higuchi, and Korsmeyer–Peppas models.
Thus, the system can be described as a diffusion-controlled matrix, where drug molecules migrate through hydrated polymer gel layers formed by HPMC K-100 and Xanthan gum, while Ethyl cellulose provides an additional hydrophobic barrier.
4.5 Effect of Polymer Ratio on Drug Release
As observed from dissolution profiles, increasing the concentration of HPMC K-100 or Xanthan gum extended the release period because of thicker gel-layer formation. Conversely, formulations with higher Ethyl cellulose content exhibited slower hydration and diffusion rates.
4.6 Morphological and Swelling Behavior
Swelling studies demonstrated that matrix hydration occurred within 30 min, forming a viscous gel barrier. The swelling index increased up to 6 h, then gradually decreased because of erosion of the outer gel layer. The dynamic balance between swelling and erosion controlled drug diffusion.
4.7 Stability Study Results
The optimized batch (F7) was subjected to accelerated stability testing (40 ± 2 °C / 75 ± 5 % RH, 90 days). Results are summarized below:
|
Parameter |
Initial |
30 days |
60 days |
90 days |
|
Appearance |
No change |
No change |
No change |
No change |
|
Hardness (kg/cm²) |
3.8 ± 0.2 |
3.7 ± 0.3 |
3.8 ± 0.2 |
3.7 ± 0.3 |
|
Drug Content (%) |
100.2 ± 0.6 |
99.8 ± 0.7 |
99.4 ± 0.8 |
99.0 ± 0.7 |
|
% Release at 12 h |
95.2 |
94.6 |
94.0 |
93.7 |
No statistically significant change was observed (p > 0.05). The optimized formulation remained physically and chemically stable.
5. DISCUSSION
The objective of developing a sustained-release matrix tablet of Captopril was successfully achieved. The combination of HPMC K-100 (hydrophilic) and Ethyl cellulose (hydrophobic) provided controlled hydration and diffusion. The results support previous studies (Mandal et al., 2007; Kumar et al., 2013) showing that drug release from HPMC matrices is primarily governed by gel-layer diffusion.
The kinetic analysis confirmed Higuchi diffusion mechanism and Fickian transport. This mechanistic behavior occurs when polymer hydration forms a barrier that gradually thickens with time, allowing drug release proportionally to the square root of time (Venkatraman et al., 2000).
The selected polymer combination also reduced initial burst release, which is a common problem in highly soluble drugs like Captopril. The release curve was smooth without irregularities, indicating uniform drug distribution within the matrix.
The stability results demonstrate that the optimized batch retained drug content and release behavior over three months, satisfying ICH guidelines and ensuring reproducibility and shelf life of the product.
From a clinical perspective, the formulation offers improved patient compliance by reducing dosing frequency (from three times to once daily) while maintaining steady plasma levels. Such systems also reduce fluctuations that can lead to side effects like hypotension or renal impairment.
5.1 Comparison with Previous Studies
|
Study |
Polymer Used |
Release Duration |
Mechanism |
Remarks |
|
Mandal et al. (2007) |
HPMC + EC |
12 h |
Diffusion |
Similar trend observed in current study |
|
Agarwal et al. (2017) |
Carbopol + HPMC |
10 h |
Diffusion/Erosion |
Comparable release profile |
|
Kumar et al. (2013) |
Guar gum |
8 h |
Swelling |
Lower retardation |
|
Present work |
HPMC K-100 + Xanthan + EC |
12 h |
Fickian Diffusion |
Stable and optimized profile |
The results confirm that combining hydrophilic and hydrophobic polymers is effective in achieving a balanced release mechanism and mechanical stability.
6. CONCLUSION:
The present study successfully demonstrated the formulation and evaluation of sustained release matrix tablets of captopril to overcome the limitations associated with its short biological halflife and frequent dosing requirements. The use of various release-retarding polymers such as Hydroxypropyl methylcellulose (HPMC), Carbopol, and Ethyl cellulose effectively controlled the drug release rate. Among the different formulations, the optimized batch exhibited desirable physicochemical properties, including uniform weight, adequate hardness, low friability, and uniform drug content, ensuring consistent quality and mechanical stability. The in vitro dissolution studies revealed that the drug release was sustained for up to 10–12 hours, following a diffusion-controlled mechanism as explained by kinetic model fitting (Higuchi or Korsmeyer– Peppas model). The polymer concentration was found to play a crucial role in controlling the release rate higher polymer levels retarded drug diffusion by forming a thicker gel barrier that slowed water penetration and drug dissolution. Stability studies conducted under accelerated conditions confirmed that the optimized formulation remained stable without significant changes in physical appearance, drug content, or dissolution profile, ensuring its suitability for long-term storage. Overall, the study concluded that sustained release matrix tablets of captopril can maintain prolonged therapeutic plasma concentrations, improve patient compliance by reducing dosing frequency, and minimize potential side effects related to fluctuating drug levels. Thus, the developed sustained release formulation provides a promising and effective oral drug delivery system for the long-term management of hypertension and related cardiovascular disorders.
REFERENCES

Shilpa Samarth*, Yasmin Shaik, Irashad Ahmad, Development, Formulation, and Evaluation of Sustained-Release Matrix Tablets Containing Captopril, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 390-403 https://doi.org/10.5281/zenodo.17797437
 10.5281/zenodo.17797437
10.5281/zenodo.17797437
