Department of Pharmacy practice, Srinivas College of Pharmacy, Mangaluru, Karnataka -574143.
Gestational diabetes mellitus (GDM) is a common metabolic disorder during pregnancy requiring careful pharmacological management to prevent maternal and fetal complications. Drug-related problems (DRPs) may compromise therapeutic outcomes and increase adverse events. This prospective interventional study aimed to identify DRPs and evaluate the impact of structured patient counselling using the Appraisal Diabetes Scale (ADS). The study was conducted over six months in a tertiary care teaching hospital involving 100 pregnant women diagnosed with GDM. DRPs were categorized as adverse drug reactions, dosing problems, drug interactions, and non-adherence. Patients were divided into intervention and control groups. Baseline ADS scores were assessed, followed by structured pharmacist-led counselling for the intervention group. Post-intervention assessment was performed. A total of 32 drug related problems (DRPs) were identified among the participants, with adverse drug reactions being the most frequently reported. Post-counselling assessment showed improvement in ADS scores and better disease perception in the intervention group compared to control group. The study concludes that structured clinical pharmacist counselling significantly reduces DRPs and improves medication adherence and disease perception among pregnant women with GDM
Pregnancy is a dynamic physiological state characterized by significant hormonal and metabolic adaptations required for fetal growth and development. However, these physiological changes may predispose women to metabolic complications, among which gestational diabetes mellitus (GDM) is one of the most common disorders encountered during pregnancy. GDM is defined as glucose intolerance with onset or first recognition during pregnancy and is associated with increased risks of maternal and neonatal morbidity.¹ The global prevalence of GDM has been rising steadily due to factors such as advanced maternal age, obesity, sedentary lifestyle, and genetic susceptibility. Inadequate glycemic control during pregnancy may lead to complications including preeclampsia, cesarean delivery, fetal macrosomia, neonatal hypoglycemia, and long-term risk of type 2 diabetes mellitus in both mother and child.² Therefore, early diagnosis and appropriate therapeutic management are essential to ensure optimal pregnancy outcomes. Management of GDM primarily involves medical nutrition therapy, lifestyle modification, regular physical activity, and self-monitoring of blood glucose levels. When lifestyle measures fail to achieve adequate glycemic control, pharmacological therapy such as insulin or selected oral hypoglycemic agents is initiated.³ However, pharmacotherapy during pregnancy requires careful monitoring because physiological alterations may influence drug absorption, distribution, metabolism, and excretion, thereby increasing the risk of therapeutic failure or adverse drug reactions. Drug-related problems (DRPs) are defined as any event or circumstance involving drug therapy that actually or potentially interferes with desired health outcomes.? DRPs may include adverse drug reactions, inappropriate drug selection, dosing errors, drug–drug interactions, and medication non-adherence. Previous studies have demonstrated that hospitalized pregnant women are at considerable risk of medication-related problems requiring clinical intervention.?
Women with GDM are particularly vulnerable to DRPs due to polypharmacy, coexisting conditions such as hypertension, concerns regarding fetal safety of medications, and inadequate knowledge about insulin administration and glucose monitoring. Poor adherence to antidiabetic therapy has also been reported among pregnant women, which may compromise glycemic control and increase the likelihood of adverse maternal and fetal outcomes.?
Clinical pharmacists play a pivotal role in identifying, preventing, and resolving DRPs through systematic medication review and structured patient counselling. Pharmaceutical care interventions have been shown to improve medication adherence, glycemic control, and overall quality of life among patients with diabetes.? In addition to pharmacological challenges, the psychological burden and emotional distress associated with diabetes during pregnancy may influence disease perception and treatment adherence. The Appraisal Diabetes Scale (ADS) is a validated instrument used to assess patients’ cognitive appraisal and emotional adjustment to diabetes.? Assessment using ADS provides measurable insight into patients’ coping ability and perception of disease control, thereby enabling evaluation of counselling outcomes.
Although pharmaceutical care services have demonstrated benefits in diabetes management, limited hospital-based interventional studies have specifically evaluated the identification of DRPs and the impact of structured pharmacist-led counselling among pregnant women with GDM in tertiary care settings. Therefore, the present study was undertaken to identify drug-related problems in pregnant women diagnosed with gestational diabetes mellitus and to evaluate the impact of structured patient counselling on DRPs and medication adherence using the Appraisal Diabetes Scale.
2.0 OBJECTIVES OF THE STUDY
To identify drug-related problems in pregnant women with gestational diabetes mellitus.
To measure the impact of structured patient counselling on medication adherence using Appraisal Diabetes Scale among pregnant women with gestational diabetes mellitus.
3.0 REVIEW OF LITERATURE
4.0 METHODOLOGY
MATERIALS AND METHODS
Study design: A hospital-based prospective intervention study conducted to identify drug-related problems and evaluate the impact of patient counselling using Appraisal Diabetes Scale(ADS) among pregnant women with gestational diabetes
Study site: Srinivas Institute of Medical Sciences and Research Centre (SIMS & RC), Mukka-574146.
Sample Size: 100
Study duration: 6 months
Ethical Clearance: The study protocol was approved by the Institutional Ethics Committee (IEC) of Srinivas Institute of Medical Science, Mukka, Mangaluru. In addition, written informed consent was obtained from all the participants in this study. (Ref. No.: SIEC/SIMS & RC/53/03/2024)
Inclusion Criteria:
•Pregnant women aged above 18 years diagnosed with gestational diabetes mellitus.
Exclusion Criteria:
•Pregnant women with psychiatric illness and who are not willing to give consent for the study.
•Pregnant women without gestational diabetes mellitus and those with previously diagnosed diabetes mellitus were excluded.
Source of data collection:
•Data source: Patient case files.
•Material used: Data collection form, Questionnaires and PIL.
•Study method: A hospital-based interventional study which will be conducted based on methodology.
THE STUDY PERIOD WAS DIVIDED INTO 3 PHASES
Data collection form: Included the patient’s demographic details, co-morbid diseases, laboratory details, treatment chart.
Assessment tools:
Appraisal diabetes scale (ADS)
Impact of pharmaceutical care plan on quality of life in diabetes mellitus patients can be identified from ADS scale. ADS can be incisive as a relatively quick (5mins) screening tool to examine a patient’s adjustment to diabetes or risk for noncompliance with a care regimen.
Institutional ethics committee approval
Patients were segregated based on inclusion and exclusion criteria
Informed consent form was obtained from the selected patient in English and Kannada.
Among 100 screened pregnant women with gestational diabetes mellitus, 50 patients who had satisfactory baseline adherence and adjustment to diabetes were excluded. The remaining 50 eligible patients were randomly assigned into a control group (n=25) and an intervention group (n=25) to evaluate the impact of patient counselling using the Appraisal Diabetes Scale.
DATA ANALYSIS
Statistical analysis involved collecting and scrutinizing every data sample in a set of items from which samples can be drawn and a suitable statistical test was applied to analyse the data. The collected data will be analyzed using Microsoft Excel.
5.0 RESULTS
DRUG RELATED PROBLEMS AMONG PREGNANT WOMEN WITH GESTATIONAL DIABETES
The table provides data on the drug related problems of pregnant women.
Table 1. Drug Related Problems
|
S.No |
Drug-Related Problems Identified |
Number of each type |
|
1 |
Adverse drug reactions |
12 |
|
2
a)
b) |
Dosing problems Drug dose too low Drug dose too high |
8
5 |
|
3 |
Drug Interactions |
7 |
|
TOTAL |
32 |
|
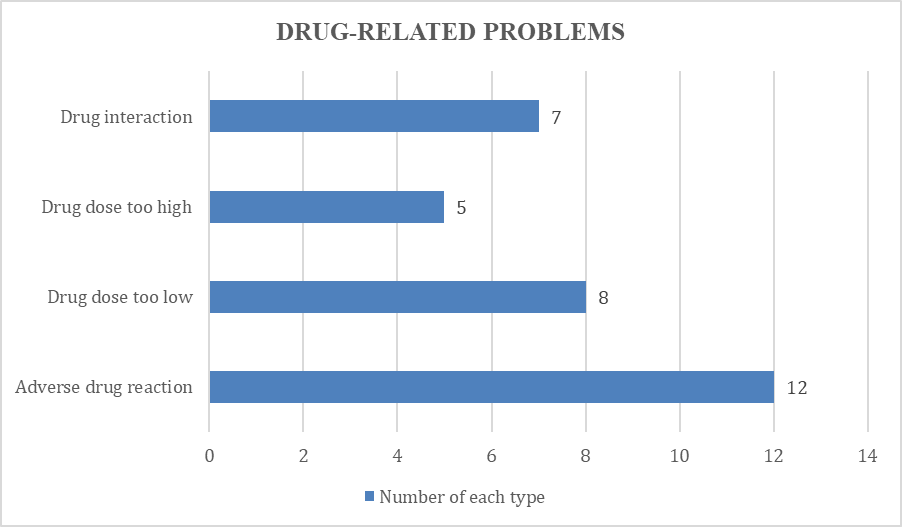
Figure 1: Identified Drug related problems
The table outlines the drug-related problems identified in pregnant women, with a total of 32 DRPs reported. Among these, 12 were adverse drug reactions, indicating unexpected or harmful responses to medications. Dosing problems were categorized into two types: 8 instances where drug doses were too low, and 5 cases where doses were too high, which can lead to ineffective treatment or increased risk of side effects, respectively. Additionally, there were 7 reported drug interactions, drug interactions mainly occurred between antidiabetic and antihypertensive medications. Addressing these problems is crucial for optimizing patient safety and treatment outcomes. The study underscores the effectiveness of counseling in reducing DRPs and improving medication management.
TO MEASURE THE IMPACT OF PATIENT COUNSELLING ON DRUG RELATED PROBLEMS OF PREGNANT WOMEN WITH GESTATIONAL DIABETES USING ADS SCALE.
Among 100 screened pregnant women with gestational diabetes mellitus, 50 patients who had satisfactory baseline adherence and adjustment to diabetes were excluded. The remaining 50 eligible patients were randomly assigned into a control group (n=25) and an intervention group (n=25) to evaluate the impact of patient counselling using the Appraisal Diabetes Scale.
APPRAISAL DIABETES SCALE (ADS)
Impact of pharmaceutical care plan on quality of life in diabetes mellitus patients can be identified from ADS Scale. ADS can be incisive as a relatively quick (5mins) screening tool to examine a patient’s adjustment to diabetes or risk for noncompliance with a care regimen.
Table 2.APPRAISAL DIABETES SCALE (ADS)
|
VARIABLE |
CONSTANT |
INTERVENTION GROUP n=25 |
CONTROL GROUP n=25 |
||
|
PRE |
POST |
PRE |
POST |
||
|
1. How upsetting is |
a. Not at all |
10% |
20% |
9% |
11% |
|
having diabetes for you |
b. Too slightly upsetting |
14% |
52% |
25% |
25% |
|
|
c. Moderately upsetting |
40% |
8% |
39% |
42% |
|
|
d. Very upsetting |
22% |
8% |
19% |
15% |
|
|
e. Extremely upsetting |
14% |
12% |
8% |
7% |
|
2. How much control |
a. Not at all |
14% |
4% |
15% |
10% |
|
over your diabetes do |
b. Slight amount |
46% |
6% |
40% |
41% |
|
you have |
c. Moderate amount |
26% |
32% |
30% |
32% |
|
|
d. large amount |
12% |
56% |
8% |
10% |
|
|
e. Total amount |
2% |
1% |
7% |
7% |
|
3. How much |
a. Not at all |
0% |
6% |
2% |
3% |
|
uncertainty do you |
b. Slight amount |
20% |
56% |
52% |
52% |
|
currently experience in |
c. Moderate amount |
56% |
14% |
17% |
17% |
|
your life as a result of |
d. large amount |
20% |
16% |
7% |
6% |
|
being diabetic |
e. Extremely large |
4% |
8% |
2% |
2% |
|
|
amount |
|
|
|
|
|
4. How likely is your |
a. Not likely at all |
15% |
22% |
13% |
13% |
|
diabetes to worsen over |
b. Slightly likely |
30% |
38% |
27% |
26% |
|
the several years |
c. Moderately likely |
23% |
28% |
24% |
24% |
|
|
d. Very likely |
20% |
12% |
22% |
23% |
|
|
e. Extremely likely |
12% |
0% |
14% |
14% |
|
5. Do you believe that |
a. Totally because of me |
2% |
2% |
5% |
2% |
|
achieving good diabetic |
b. Mostly because of me |
18% |
2% |
17% |
2% |
|
control is due to your |
c. Partially because of me |
76% |
94% |
77% |
93% |
|
effort as compared to |
and other factors |
4% |
2% |
1% |
2% |
|
factors which are your |
d. Mostly because of other |
0% |
0% |
0% |
0% |
|
control |
factors |
|
|
|
|
|
|
e. Totally because of other |
|
|
|
|
|
|
factors |
|
|
|
|
|
6. How effective are you in coping with your diabetes |
|
10% 46% 40% 4% 0% |
18% 18% 26% 36% 2% |
13% 50% 35% 2% 0% |
13% 52% 34% 1% 0% |
|
7. To what degree does your diabetes gets in the way of your developing life goals |
|
4% 42% 48% 4% 2% |
18% 30% 48% 4% 0% |
7% 46% 40% 5% 2% |
6% 43% 47% 3% 1% |
DISCUSSION
The present hospital-based interventional study was conducted to identify drug-related problems (DRPs) among pregnant women with gestational diabetes mellitus (GDM) and to evaluate the impact of structured pharmacist-led counselling using the Appraisal Diabetes Scale (ADS). The findings demonstrate that DRPs are prevalent in this vulnerable population and that clinical pharmacist intervention plays a significant role in improving medication safety and disease perception. In the present study, 32 drug-related problems were identified among 100 participants. Adverse drug reactions were the most frequently observed DRPs, followed by dosing errors and drug–drug interactions. These findings are consistent with the study reported by Bezerra et al., who reported therapeutic ineffectiveness and adverse drug reactions as the most common DRPs among pregnant women with hypertension and GDM.9 Their findings highlight the importance of careful insulin dose adjustment and monitoring during high-risk pregnancies. Similarly, Smedberg et al. observed that a considerable proportion of pregnant and lactating women experienced at least one DRP during hospitalization, emphasizing the need for systematic medication review and multidisciplinary collaboration to enhance patient safety.10 The occurrence of drug interactions between antidiabetic and antihypertensive medications in the present study further supports the evidence that polypharmacy increases medication-related risks during pregnancy. Medication adherence plays a crucial role in achieving optimal glycemic control in GDM. In the present study, structured counselling resulted in improved disease perception and coping ability as assessed by the ADS. These findings are in agreement with Borzouei et al., who reported that improved adherence was associated with better glycemic control among pregnant women with GDM.11 Furthermore, Elnour et al. demonstrated significant improvements in glycemic parameters and maternal outcomes following structured pharmaceutical care interventions in women with GDM.12 Similarly, Krishnakumar et al. reported significant enhancement in medication adherence and therapeutic outcomes after patient education among women receiving insulin or metformin therapy for GDM.13 These studies collectively support the beneficial impact of pharmacist-led counselling observed in the present study. The improvement noted in ADS parameters suggests that counselling not only enhances medication adherence but also positively influences psychological adjustment to diabetes. Emotional distress, uncertainty, and reduced perceived control are common among women newly diagnosed with GDM. Educational interventions focusing on insulin administration techniques, hypoglycemia management, lifestyle modification, and regular glucose monitoring can reduce anxiety and improve self-efficacy, thereby promoting better treatment adherence. Overall, the findings of this study emphasize the critical role of clinical pharmacists in identifying and resolving DRPs and in improving both pharmacological and psychological aspects of GDM management. Integrating pharmacist-led counselling into routine antenatal care may significantly enhance maternal safety and therapeutic outcomes.
7.0 LIMITATIONS OF THE STUDY
CONCLUSION
The present study demonstrated that drug-related problems (DRPs) are common among pregnant women with gestational diabetes mellitus and may compromise therapeutic outcomes if not identified and addressed promptly. The most commonly observed DRPs included adverse drug reactions, dosing errors, and drug–drug interactions.
Structured pharmacist-led counselling significantly improved medication adherence and disease perception, as evidenced by improvement in Appraisal Diabetes Scale (ADS) parameters in the intervention group. The findings highlight the importance of systematic medication review and patient education in minimizing medication-related risks during pregnancy.
Integration of clinical pharmacists into multidisciplinary antenatal care teams can play a vital role in optimizing pharmacotherapy, enhancing patient understanding, and improving overall maternal health outcomes in gestational diabetes mellitus.
ACKNOWLEDGEMENT
I sincerely thank Dr. Krishnananda Kamath K, my guide, and Dr. Blessy Fernandes, my co-guide, for their invaluable guidance, support, and encouragement throughout this research work. I express my deep gratitude to Dr. A. R. Shabaraya, Principal, for providing the necessary resources and constant motivation to carry out this study. I extend my heartfelt thanks to Srinivas College of Pharmacy and SIMS & RC for providing the opportunity and facilities essential for this research. I am also grateful to all the faculty members, staff, parents, friends, and study participants for their constant support and contribution, which made this work possible.
REFERENCES


Fathima Thabsheera, Krishnananda Kamath K, Blessy Fernandes, A.R. Shabaraya, Drug-Related Problems and Impact of Patient Counselling Using Appraisal Diabetes Scale in Pregnant Women with Gestational Diabetes: A Hospital-Based Intervention Study.., Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 1428-1436. https://doi.org/10.5281/zenodo.19001536
 10.5281/zenodo.19001536
10.5281/zenodo.19001536
