
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Dr. Utamaro Mahajan College of B Pharmacy, Chalisgaon, Dist. Jalgaon,424101.
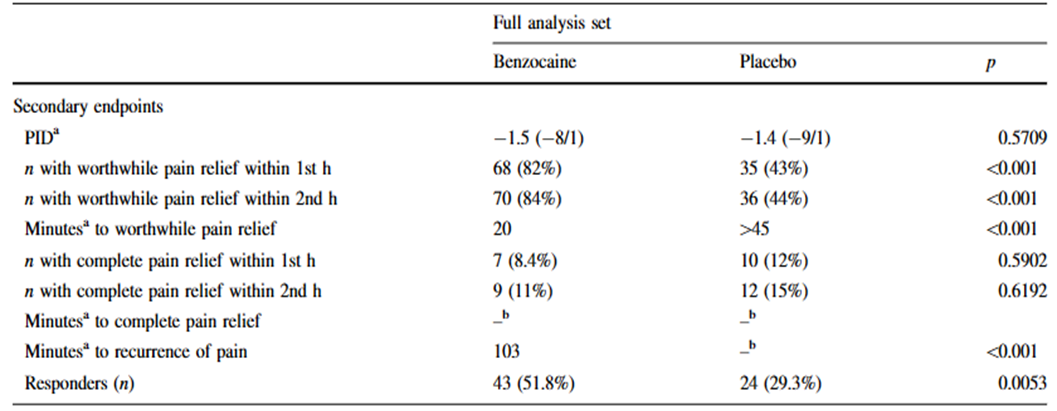
Lozenges with benzocaine are often used to relieve the symptoms of an acute sore throat. The reason for this take a look at changed into to determine whether or not giving patients who skilled discomfort after swallowing a benzocaine lozenge was better than giving them a placebo. Volunteers with acute, easy sore throats were double-blindly assigned to receive either a placebo lozenge or an eight mg dose of benzocaine. A numerical visual score scale was used to degree pain. The sum of the ache depth differences (SPID) throughout two hours served as the primary final results degree. The range of patients who reported 50% or more in their baseline pain rating (responders), folks that had beneficial and whole pain reduction, the time it took to obtain profitable and whole pain relief, and the prevention of pain recurrence and side effects have been all examples of secondary outcome measures. After 50 patients had been protected, a predetermined interim evaluation showed that benzocaine had become advanced to a placebo within the SPID (p = 0.0086). By means of this factor, 165 patients in all have been enrolled (complete evaluation set, or FAS), and statistical analysis was finished. Patients receiving benzocaine confirmed a appreciable decrease in median SPID in the FAS than those getting a placebo (-12vs. - five, p = 0.001). In the benzocaine group, there have been enormously more responders and patients who experienced meaningful pain relief. There have been only a few folks who had a general ache remedy. The median period for sizable pain alleviation became 20 minutes for benzocaine and forty-five minutes for placebo. There have been no unfavorable occurrences noted. Benzocaine lozenges are a useful, well-tolerated therapy to reduce excruciating pharyngeal pain, and they're more effective than placebo lozenges.
A typical sign of bacterial or viral infections of the oropharyngeal tract is a sore throat. The goal of symptomatic treatment is to lessen the excruciating pain. The benefit of topical local anesthetics is that they work locally, and in the case of benzocaine (ethyl 4-aminobenzoate), esterases quickly convert it into an inert substance after absorption. Systemic adverse effects are therefore extremely uncommon. By reducing the permeability of the neuronal membrane to sodium ions, benzocaine prevents both the initiation and conduction of nerve impulses. An rise in sensitivity thresholds, such as the pain threshold, is linked to this. Peripheral blood monocytes and neutrophils produce more oxygen free radicals in individuals with acute pharyngitis. When using topical benzocaine to treat the symptoms of a simple sore throat, its strong antibacterial action and noticeable benzocaine radical scavenging activity are advantageous Six kinds of microorganisms that are often present in the oral cavity—Streptococcus mutans, S. sanguis, S. mitis, S. salivarius, Actinomyces viscosus, and Candida albicans—significantly decreased cell proliferation. Upon exposure to 20% liquid benzocaine for one minute (bacteriostatic and fungistatic effects) and two hours (bactericidal and fungicidal effects). Benzocaine is available globally in a variety of formulations and active compound strengths for this broad-spectrum action in treating symptomatic sore throat pain. It is marketed by multiple companies as mono- or combination preparations, as well as partially as over-the-counter products. The effectiveness of various benzocaine lozenges in treating acute pharyngitis was assessed in two investigations. In a single-blind trial, Kagan and colleagues contrasted two dosages of benzocaine combined with an antimicrobial. The 10 mg dosage of benzocaine worked better than half the amount. Bush and colleagues demonstrated that a newly created 8 mg lozenge was not inferior to a commercial pastille with the same dosage. There hasn't been a comparison with a placebo yet, though. Thus, the purpose of this study was to determine if an 8 mg benzocaine lozenge was more effective than a placebo in treating acute, simple sore throats.
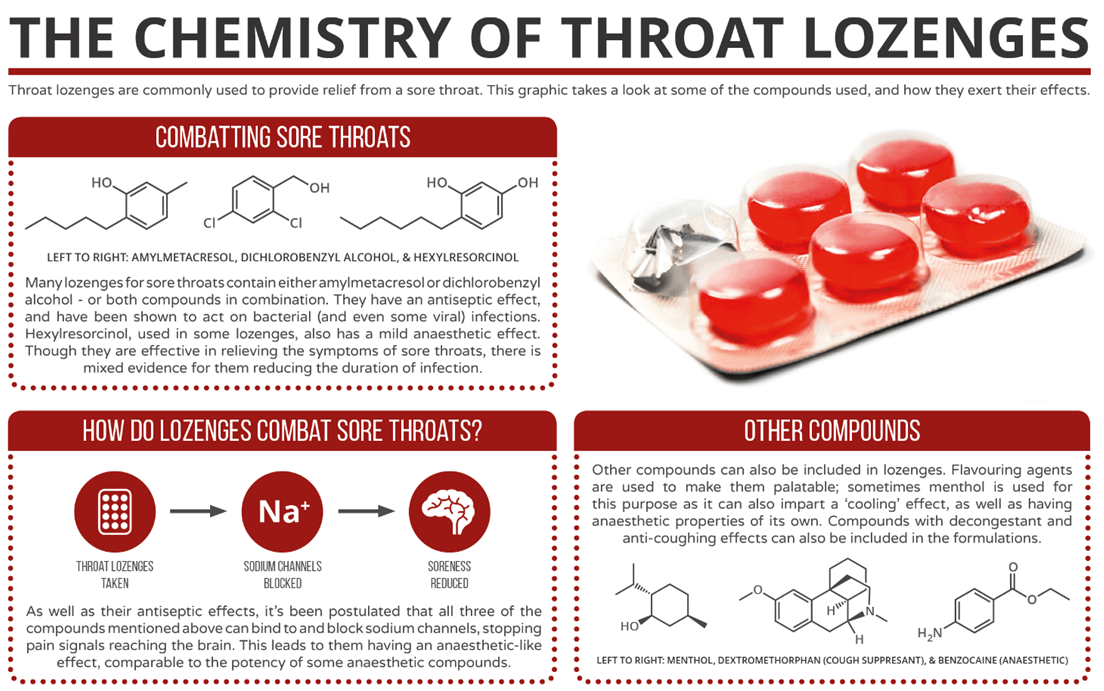
Figure: -1
METHODS: -
Participants had to be at least 18 years old, have experienced mild to severe discomfort (rated at least five out of ten) on a visual rating scale (VRS) for at least 24 hours, and have consulted their family doctor due to a sore throat to be eligible to participate. The International Conference on Harmonization Good Clinical Practice Guidelines and the Declaration of Helsinki were both adhered to by the research protocol. The independent regional Ethics Committees gave their approval to each of the 17 participating outpatient clinics. The following strict exclusion rules were in place:
The patients' age, gender, medical and surgical histories, and the outcomes of a general physical examination, which included their height, weight, seated blood pressure, and heart rate, were documented after they provided written informed consent. A visual rating scale with numbers ranging from 0 to 10 was used to gauge the baseline level of discomfort. Before being given the study drug, patients were given two stopwatches. This was distributed using a double-blind, randomized process that was run in blocks of four patients. A lozenge containing either 8 mg of benzocaine, which would dissolve gradually in the mouth, or a placebo lozenge that was identical in size, color, and flavor served as the research drug. To ensure that it would only be accessible in an emergency, the blinding code list was sealed and kept in storage. The research drug was administered concurrently with the commencement of the stopwatches, and patients were told to stop one watch as soon as they believed that the pain was worth it and the other if and when the agony leveled out. Additional measurements of pain were taken at 15 (±3), 30 (±3), 45 (±3), 60 (±3), and 90 (±3) minutes. The patients were asked if they were feeling any systemic or local side effects (such as burning, itching, or redness) whenever they reported discomfort. At the end of the trial, which was set to end in 120 (±6) minutes, patients were evaluated for their vital signs, acceptance of the study drug, and any side effects. The sum of pain intensity differences (SPID) across a 2-hour period served as the main outcome measure. The secondary outcome measures included the number of patients who reported a halving or more of their baseline pain (referred to as responders), the number of patients who experienced worthwhile and complete pain relief within 60 and 120 minutes, the time to worthwhile/complete pain relief and the time to recurrence of pain (with an increase in the pain intensity to baseline level), and the change in pain intensity after 2 hours in comparison to baseline (PID, pain 120min - pain 0min). Before analysis, every case report form was examined for quality assurance.
Figure: -2
Statistical Analysis:-
For statistics, SAS V8.3 was utilized. Analysis of safety and effectiveness was done by intention to treat, which included all randomly assigned individuals. The total number, mean, median, standard deviation, minimum and maximum, and frequency and percentage of categorical data were used to summarize the metric variables for tabulation and graphical presentation. The hypothesis that needed to be evaluated was that there was no difference in the primary endpoint between the 8 mg benzocaine active treatment group and the placebo group (null hypothesis H0). The accompanying alternative hypothesis (H1) stated that patients receiving benzocaine had a higher "Sum of PID over 2 h" than those getting a placebo. The Mann–Whitney U test was used to evaluate the main effectiveness factors. For a two-sided test, the error or likelihood of finding a significant difference in the primary effectiveness endpoint was fixed at a = 0.05. We assumed that the SPIDs for patients receiving a placebo and benzocaine treatments were 15 and 22, respectively (standard deviation 14), in order to calculate the sample size. A power of 80% was linked to a number of 174 (taking into account 20% of dropouts) if the significance level was chosen at p = 0.05. Due to estimating uncertainty, an interim analysis was conducted utilizing Bauer and Kohne's methodology. which sets the nominal, predetermined amount of a = 0.05 as the upper limit on the total type one error probability (a). Two limits for the p value for the interim analysis were to be defined as part of this process (a1 = 0.0233 for superiority of the test product and a2 = 0.5 for "no difference"). Following the completion of the trial (sample) by 50 patients (groups placebo 24 and benzocaine 26), an interim analysis was conducted using the predetermined limitations. The trial would have been terminated and the null hypothesis would have been rejected with 95% confidence if either benzocaine or a placebo had been preferred, according to p(1)\-a1. All of the trial's participants (full analysis set, FAS) were examined for efficacy; nevertheless, because patient recruitment continued during the interim analysis. Chi-square tests were used to compare the number of patients who experienced "worthwhile/complete" pain reduction and the number of patients who experienced "response" across the treatment groups. A log-rank test was employed to compare treatment groups, and Kaplan-Meier estimates were utilized to analyze time to event data (time to worthwhile/complete pain alleviation and recurrence of pain).
Findings:-
There were no patient dropouts among the 165 patients recruited across 17 centers (Fig. 3), and 43 patients (21 group placebo, 22 group benzocaine) had overall protocol deviations, including one major protocol violation (group placebo, baseline pain intensity of four ignored the inclusion criterion). No significant differences were observed between the sample's treatment groups and the FAS in terms of demographics, patient history, vital signs, and baseline pain intensity (Table 1).The corrected error probability for the FAS was determined to be a = 0.00078/0.0086 (p value of the sample) following the SPID analysis, which produced a p value of 0.0086 indicating the superiority of the benzocaine over the placebo therapy. Both samples had 100% treatment compliance. During the 2-hour period, the sample and the FAS had mean sums of pain intensity differences (±SD) of -14.2 ± 8.1 and -13.6 ± 10.6 (group benzocaine) and -8.3 ± 11.5 and 9.3 ± 11.7 (group placebo), respectively (Table 1). Figs. 2a and b show the mean pain intensities at the different time periods, and Table 2 provides a summary of the additional findings. One potential confounding factor that was ruled out was the center-specific impact. Additional information is provided on. The original article may be found at http://www.uniklinik-freiburg.de/rechtsmedizin/live/forschung/phytomedicine.html.One patient in the placebo group experienced an adverse event during the whole research. incident, a vertigo attack that went away before the study's conclusion and didn't need medical attention. The trial had no discernible impact on vital signs.
Medicine or revealed any clinically significant changes during the physical examination (see website). No signs of local intolerability were noted by any of the patients.
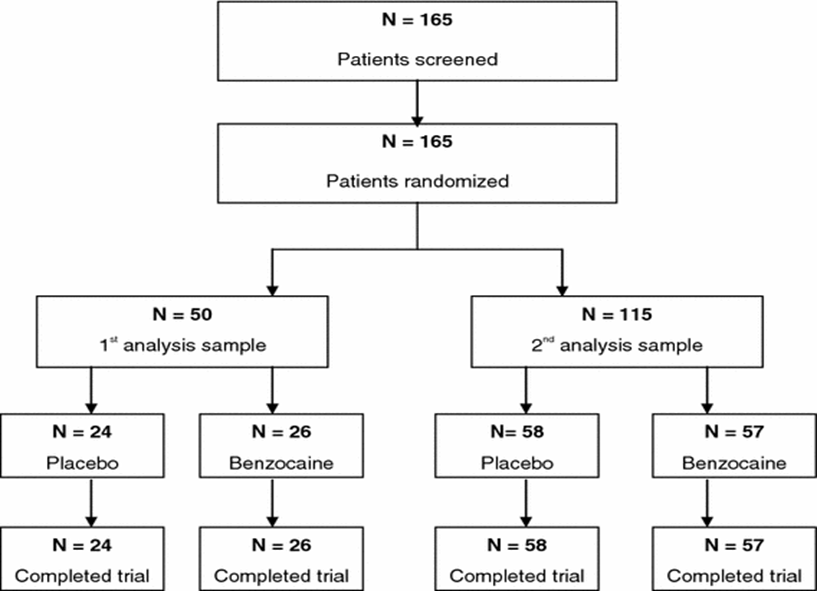
Figure: - 3
Table:-1 Vital signs, demographic data, and primary endpoint findings from the entire analysis set and the intermediate analysis sample SPID sum of pain intensity difference over two hours
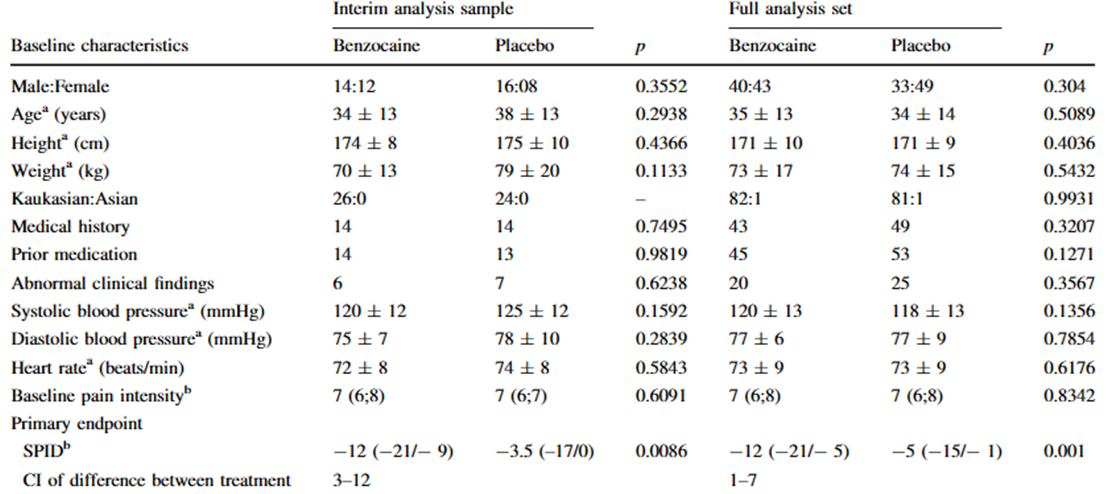
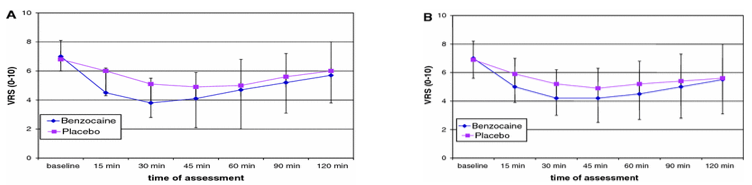
Figure:-4
Conversation:-
Sucking lozenges containing 8 mg of benzocaine significantly reduced discomfort in individuals with mild to severe uncomplicated sore throats that had just started, compared to sucking a placebo lozenge. With benzocaine lozenges, the onset of noticeable pain alleviation was around 20 minutes, and it was noticeably quicker than with placebo lozenges. Prior research evaluating several topical benzocaine formulations for the same disease had similarly noted a rapid start of pain alleviation. The 8 mg benzocaine lozenge's effects persisted for almost an hour. This also explains why there was no change in pain intensity between the placebo and benzocaine lozenges at the beginning and conclusion of the research. The amide lidocaine, which has also been shown to have positive therapeutic implications in the treatment of sore throats, is more readily absorbed by the mucosal membranes than the ester benzocaine. Ambroxol, a derivative of local anesthetic, has also been demonstrated to reduce complaints related to a severe, simple sore throat. However, because of its strong mucolytic and anti-inflammatory properties, ambroxol could be better conserved for suppurative pharyngitis. Other lozenges that have a modest local anesthetic effect, including dichloro-benzyl alcohol, amylmetacresol, and hexylresorcinol, have a strong local antiseptic domain and are now used to address sore throat issues. Although they have not yet been conducted, studies comparing the various strategies—such as lozenges containing NSAIDs, such as flurbiprofen, or lozenges containing combinations of antiseptics and enzymes—are necessary to determine the best course of action for treating acute, simple sore throats. Lozenges have an advantage over sprays or gargles in that the medicine releases continuously while being sucked. Sucking encourages the production of saliva, which in and of itself helps to relieve sore throat discomfort. Lozenges containing local anesthetics are probably less likely to cause adverse outcomes than those containing NSAIDs, however the development of methemoglobinemia after topical benzocaine usage has lately sparked alarm.This potentially fatal adverse effect is uncommon. However, because it is impossible to predict which people will be at risk of developing methaemoglobinemia following exposure to benzocaine, and because the dose needed to produce toxicity and a therapeutic effect overlap, Guay recommended that clinical use of benzocaine be discontinued entirely.
Table:- 2 Results of The Whole Study Set's Secondary Endpoints
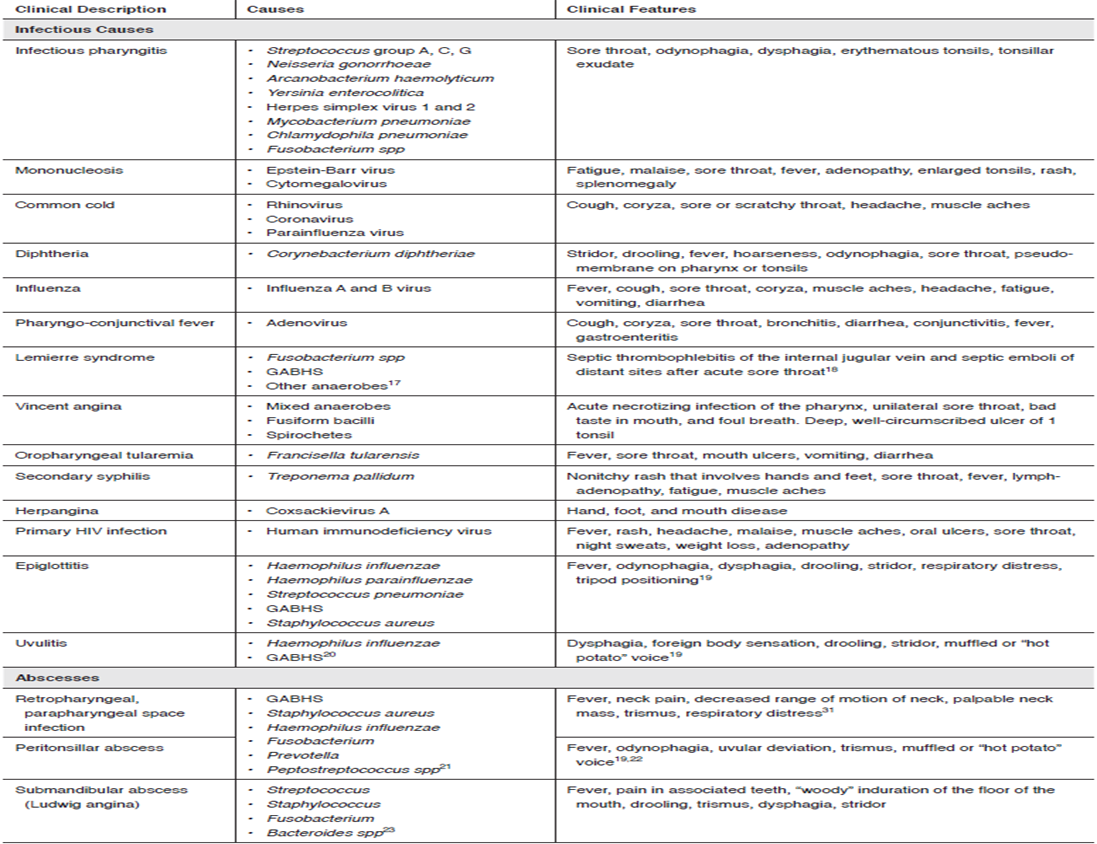
Institutions have previously taken this proposal into consideration, and government regulatory bodies in the US and Canada have issued warnings, but not globally. Between 2007 and 2010, 714600 packages were sold in Germany. Early detection and prompt intravenous delivery of 1-2 mg/kg of methylene blue may avert fatal outcomes in the case of methaemoglobinemia. Ongoing education might make it easier to handle this infrequent negative occurrence. Viral infections are the primary cause of sore throats, which are prevalent. Bacterial infections, allergies, mouth breathing dryness, inhaling irritants (like smoke), trauma (such endotracheal intubation), and malignancy are among more causes. Pain, swelling, and redness are all signs of an irritated oropharyngeal tract mucosa, particularly after swallowing. There are a number of widely accepted, varyingly evidence-based therapy recommendations for sore throats.At one extreme, early antibiotic therapy is advised to avoid the significant hazards that Fusobacterium necriforme and Group A Streptococci provide. On the other hand, as sore throat is typically a self-limiting condition, only symptomatic treatment is recommended. Other recommendations fall somewhere in the middle, suggesting that antibiotic therapy be preceded by a range of diagnostic tests;
These have draw backs:-
Delaying antibiotic prescriptions decreased antibiotic use, but there was no difference in outcomes between delayed, immediate, and no medications for respiratory tract infections, including sore throats, according to a Cochrane analysis. There was no difference in the resolution of sore throat symptoms or patient satisfaction from antibiotic delay in two of the studies that included a "no antibiotics" group. The most effective strategies for lowering the prescription of antibiotics for inappropriate reasons have been multifaceted initiatives that include public, patient, and physician education in a range of settings and formats. Because of its triple action—pain-relieving, anti-oxidative, and anti-microbial—benzocaine lozenges may be a suitable place to start when treating acute, simple sore throat symptoms. They also help reduce the overall number of antibiotic prescriptions and their associated hazards.
Table: -3 Basic Information about Infection Causes Of Sore Throat
REFERENCES





Yash Chaudhari*, Rushikesh Bhoi, Yash Joshi, Harshal Mandole, Karan Patil, Nazeer Ahmed, Efficacy of A Benzocaine Lozenge in The Treatment of Uncomplicated Sore Throat, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 2348-2358 https://doi.org/10.5281/zenodo.15244901
 10.5281/zenodo.15244901
10.5281/zenodo.15244901