1M Pharmacy in pharmaceutics, KGRDCP, Karjat, Maharashtra, India
2M.S.(Pharma)Pharmacology and Toxicology NIPER SAS NAGAR, Mohali, Punjab, India
3M Pharmacy in pharmaceutics, KGRDCP, Karjat, Maharashtra, India
Gastro-effervescent tablets have emerged as an innovative pharmaceutical dosage form designed to provide rapid and efficient drug delivery, particularly for medications requiring enhanced absorption in the stomach. This study focuses on the formulation, development, and evaluation of gastro-effervescent tablets, with the aim of improving patient compliance and therapeutic efficacy. The tablet formulation includes a combination of an active pharmaceutical ingredient (API), citric acid, and sodium bicarbonate, creating an effervescent reaction upon contact with water. This review paper aims to provide valuable insights into the development of gastro-effervescent tablets as a viable drug delivery system, offering potential advantages in terms of patient convenience, rapid onset of action, and improved absorption. Gastro-effervescent tablets have the potential to revolutionize the field by providing a convenient, fast-acting, and effective means of administering medications.
Historically, oral drug administration has been the predominant route for drug delivery. During the past two decades, numerous oral delivery systems have been developed to act as drug reservoirs from which the active substance can be released over a defined period of time at a predetermined and controlled rate. Although some important applications, including oral administration of peptide and protein drugs, can be used to prepare colonic drug delivery systems, targeting drugs to the colon by the oral route. More often, drug absorption is unsatisfactory and highly variable among and between individuals, despite excellent in vitro release patterns1,2. The gastrointestinal (GI) tract has advanced consistently in terms of technology and diversity, encompassing a variety of systems and devices such as floating systems, raft systems, expanding systems, swelling systems, bioadhesive systems and low-density systems. Gastric retention will provide advantages such as the delivery of drugs with narrow absorption windows in the small intestinal region. Also, longer residence time in the stomach could be advantageous for local action in the upper part of the small intestine, for example treatment of peptic ulcer diseas.3,4. Furthermore, improved bioavailability is expected for drugs that are absorbed readily upon release in the GI tract. These drugs can be delivered ideally by slow release from the stomach. Many drugs categorized as once-a-day delivery have been demonstrated to have suboptimal absorption due to dependence on the transit time of the dosage form, making traditional extended-release development challenging. Therefore, a system designed for longer gastric retention will extend the time within which drug absorption can occur in the small intestine5,6.
1.1. Modified Release Oral Drug Delivery Systems
The oral route represents nowadays the predominant and most preferable route for drug delivery. Unlike the majority of parenteral dosage forms, it allows ease of administration by the patient and it’s the natural, and therefore a highly convenient way for substances to be introduced into the human body.
Oral drug delivery systems (DDS) are divided into immediate release and modified release systems. Immediate release DDS are intended to disintegrate rapidly, and exhibit instant drug release. They are associated with a fast increase and decrease, and hence fluctuations in drug plasma levels, which leads to reduction or loss in drug effectiveness or increased incidence of side effects. Oral modified release delivery systems are most commonly used for
1) delayed release (e.g., by using an enteric coating);
2) extended release (e.g., zero-order, first-order, biphasic release, etc.);
3) programmed release (e.g., pulsatile, triggered, etc.) and
4) site-specific or timed release (e.g., for colonic delivery or gastric retention).
Extended, sustained or prolonged release drug delivery systems are terms used synonymously to describe this group of controlled drug delivery devices, with predictability and reproducibility in the drug release kinetics. Delayed release dosage forms are distinguished from the ones mentioned above as they exhibit a pronounced lag time before the drug is released. Oral extended-release dosage forms offer the opportunity to provide constant or nearly constant drug plasma levels over an extended period of time following administration. Extended-release DDS include single-unit, such as tablets or capsules, and multiple-unit dosage forms, such as minitablets, pellets, beads or granules, either as coated (reservoir) or matrix devices.
The maximum achievable sustained drug release is subject to inter individual variations, with an average gastrointestinal (GI) transit time of around 24 h in humans. The transit time is affected by age, gender, body mass index and the state of health of the individual as well as his emotional state and composition of meals. In addition, drugs affecting gastric motility, such as opioid analgesics or metoclopramide, have to be taken into account. The gastric emptying process can vary from a few minutes to 12 h, depending upon the physiological state of the subject and the design of pharmaceutical formulation. This variation, may lead to unpredictable bioavailability and times to achieve peak plasma levels, since the majority of drugs are preferentially absorbed in the upper part of the small intestine.7,8
1.2 Gastroretentive Drug Delivery Systems
The retention of oral dosage forms in the upper GIT causes prolonged contact time of drug with the GI mucosa, leading to higher bioavailability, and hence therapeutic efficacy, reduced time intervals for drug administration, potentially reduced dose size and thus improved patient compliance. Therefore, extended-release DDS possessing gastric retention properties may be potentially useful.
Gastro Effervescent Tablets beyond the bubbles provided spectrum of benefits like
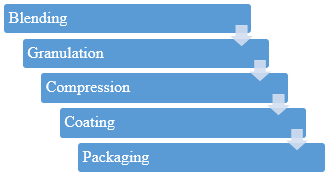
Formulation:
Preparation of Effervescence tablets by using various concentrations of Polymers
Thoroughly mix the active ingredient, citric acid, sodium bicarbonate, binder and disintegrating agent.12,13
If needed for the binding process, add a granulating agent and granulate the mixture in a Rapid Mixer Granulator or High shear Homogenizer.13,14
Compress the mixture into tablets using a tablet press.
It is an optional stage if required apply a coating to improve stability, taste, or appearance.
Package the effervescent tablets in moisture-resistant and airtight packaging to prevent premature activation.15,16
Characterization
I. Preformulation studies
II. Evaluation of blends
III. Evaluation of floating tablets
CONCLUSION
To conclude it will not be wrong to say that Effervescent Solutions for Gastric Relief are an Unveiling the Fizz of Innovation. As research continues to explore their potential, the future of gut health seems to be brimming with effervescent possibilities. Imagining a future where personalized bubbly concoctions tackle heartburn, constipation, and everything in between, all with a delightful fizz. To summarize, the development and evaluation of gastro effervescent tablets present a promising avenue for enhancing medication delivery and improving patient compliance. Thus one can say that these floating tablets can bring a abeyant leap in the treatment designing and tailoring of Gastrointestinal disease and further play a role in exploration of Precision Medicine.
REFERENCE


Sudarshan Mirghal, Payaam Vohra, Priya Patil, Enhancing Drug Delivery: Formulation and Evaluation of Novel Effervescent Tablets for Optimal Bioavailability, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 6, 971-976. https://doi.org/10.5281/zenodo.11970531
 10.5281/zenodo.11970531
10.5281/zenodo.11970531
