
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Shivlingeshwar College of Pharmacy Almala Tq. Ausa Dist. Latur.
Background: Snake bites are the common cause of morbidity and mortality in tropical countries. Snake bite is a serious problem in many sectors, especially in south Asian countries. Snake-bite has become an occupational disease. The main objective is to study the demographics and ASV use, assess whether ASV has been given or not for patients who had been treated in hospitals in the management of poisonous snake bites in the scenario of global ASV scarcity. Methods: Patients of snake bites with signs of envenomation were included in this observational, prospective study. Non- envenomation and died patient were excluded. Immediately, low dose (30 to 50 ml) of ASV was started and patients were kept under intensive observation with supportive care & titrated up to 500 ml. Results: Among the 156 patients, there were 74 males and 82 females. 91 patients had vasculotoxic, 43 patients had neurotoxic and 20 patients had mixed type of envenomation. In study, Average dose of ASV given was 48.11 ml. Conclusions: The epidemiological study shows the epidemics of the ASV use, those who came earlier to hospital required a low dose of ASV to save lives of victims of poisonous snake bites with good supportive management.
Snake bite is a serious problem in many sectors of the world, especially in south Asian countries. Snake-bite has become an occupational disease among peoples like farmers, plantation workers, herdsmen, fishermen, snake restaurant workers and many food producers (Warrell, 2010). There are about 236 species of snakes in India, most of which are nonpoisonous. Their bites, lead to cause panic reaction and local injury, but do not harm the patient. There are 13 known species that are poisonous and of which four species naming common cobra (Najanaja), Russell’s viper (Dabiolarusselii), saw-scaled viper (Echiscarinatus) and common krait (Bungaruscaeruleus) are highly venomous and are responsible for most of the poisonous bites in India (Surjit Singh).
Classification of snakes
There are three main families of venomous snakes Elapidae, Viperidae and Colubridae (Kathe, 1996).
These snakes have fixed front fangs and deliver venom through a bite. Their venom is typically neurotoxic, affecting the nervous system.
Examples: Cobras, Kraits, Coral snakes, Sea snakes, Mambas Characteristics:
Vipers have long, hinged fangs that allow deep penetration and efficient venom delivery. Their venom is usually hemotoxic, affecting blood and tissues.
Examples: Russell’s viper, Saw-scaled viper, Pit vipers (like rattlesnakes) Characteristics:
Colubridae is the largest snake family, and while most are non-venomous, a few species possess venom. Their fangs are usually rear-positioned, making venom delivery less effective in humans.
Examples: Boomslang, Twig snake Characteristics:
Signs and symptoms of snake bite
The signs and symptoms of snake bite categorized in mainly two phases.
Chronic phase (months to years after the bite): Weakness, loss of secondary sexual hair, amenorrhea, testicular atrophy, hypothyroidism (Guidelines Reprint Of The, 1999).
Acute Phase: Nausea, vomiting, malaise, abdominal pain, weakness, drowsiness, dizziness, faintness, collapse, shock, hypotension, cardiac arrhythmias, pulmonary and conjunctival oedema, Bleeding from recent wounds, gums, epistaxis, eyes, haemoptysis, haematemesis, rectal bleeding or melaena, haematuria, vaginal bleeding, Drowsiness, paraesthesiae, abnormal taste and smell, “heavy” eyelids, ptosis, external ophthalmoplegia, facial palsy, aphonia, difficulty in swallowing, respiratory and flaccid paralysis, pain, stiffness and tenderness of muscles, trismus, myoglobinuria, hyperkalaemia, cardiac arrest, haematuria, haemoglobinuria, myoglobinuria, oliguria/anuria, Symptoms and signs of uraemia, acute renal failure, shock, hypoglycemia.
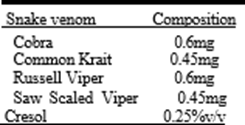
ASV Composition:
Table 1. Showing ASV composition
MATERIALS AND METHODS
500 patients consecutively admitted with history of snakebite were included in the study after obtaining ethical committee clearance as well as informed consent from all patients. All patients were evaluated with a detailed history and clinical examination. The present descriptive, case series, case control, observational study was carried out in between June2015 to November 2015 in the department of Medicine, a tertiary care center in Aurangabad. 156 Patients with history of venous snake bite with signs of envenomation were included in the study. Patients with non-poisonous snake bite were excluded. Data were collected on pre- designed, pre-tested, and structured questionnaire form and master chart by interviewing the study subjects who were hospitalized during the study period. Statistical tests were applied to calculate the frequencies and means of different variables studied. The average dose of ASV given was calculated.
Table 2. Showing seasonal influence of snake bite cases
|
Months |
No. Of Patients |
|
Jun |
10 |
|
Jul |
38 |
|
Aug |
32 |
|
Sep |
36 |
|
Oct |
30 |
|
Nov |
10 |

Graph 1. Showing seasonal influence of snake bite cases
In our study, Total average dose of ASV required was 48.11 ml and 9 patients of them required ventilation support for the surveillance. The patient having more complications like renal failure, cardiac problems and some having respiratory failure requires ventilation support are due to the venom exposure.
Table 3. Showing no. of male female cases
|
Type of bite |
No. Of patients |
|
Vasculotoxic |
91 |
|
Neurotoxic |
43 |
|
Mixed |
20 |
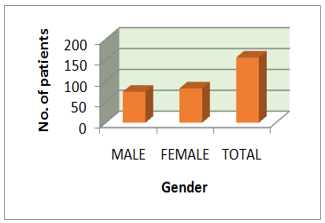
Graph 2. Showing no. of male female
Table 4. Showing no. of patient with types of bite
|
No. Of patients |
Numbers |
|
Male |
74 |
|
Female |
82 |
|
Total |
156 |
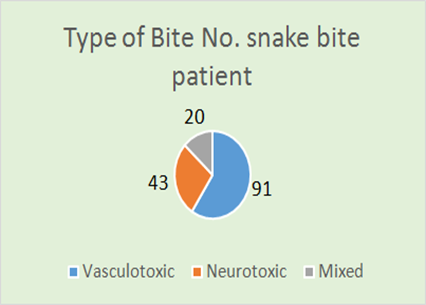
Graph 3. Showing no. of patient with types of bite
In this patient some complication such as Respiratory Depression (RD), Respiratory Failure (RF), Dropped Eyelids, Acute Renal Failure (ARF), Cellulities, Opthalmoplegia, Hematuria, Necrotic skin patch (Bhuvaneswar, 2014). By applying the statistics rules the average mean of the ASV use is been calculated by putting in following formula and the average ASV dose is 48.116. Furthermore, the frequency of the ASV dosing is calculated and results are in Table no. 5.
Table 5. Showing rate of the percentage complication of the snake bite patients
|
Complications |
Rate |
|
RD |
5 |
|
RF |
7 |
|
Dropped eyelids |
1 |
|
ARF |
10 |
|
Cellulities |
1 |
|
Opthalmoplegia |
1 |
|
Hematuria |
1 |
|
Necrotic skin patch |
1 |

Graph 4. Showing rate of the percentage complication of the snake bite patients
In the dosing frequency more commonly 30 cc of the ASV is given in 56 patients followed by 50 cc in 35 patients and as mentioned in table. The case series study of 500 patient’s records during 6 months according to proforma was carried out. Among that 156 patients were given ASV. Out of 156, 74 males with snake bite and 82 females respectively received ASV. Immediately, those patients with poisonous snake bite started dose of (10 to500 ml) ASV given IV, after carefully monitoring of patient. The patient were kept under observation with supportive care like drugs such as neostigmine, atropine, blood & fresh frozen plasma, artificial ventilation, MgSO4 bandage as needed.6 Vital parameters, two hourly urine output, clotting time, signs of respiratory failure, bleeding tendencies were closely monitored (David, 2010).
Mean:
????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????????
???????????????? (????) = ∑ ????????. ????????????????????????????????????????
???????????????? = 7410
156
Frequency
Total no. of patients are 156
Table 7. Showing annual no. of snake bite patient
|
Year |
No. Of snake bite |
ASV given |
|
2013 |
500 |
268 |
|
2014 |
450 |
277 |
|
2015 |
500 |
156 |

Graph 6. showing annual no. of snake bite patient
DISCUSSIONS
Snake bites are the common cause of morbidity and mortality in tropical countries. In India, there are 216 species of snakes, of which only four are venomous snakes (Cobra, Kraits, Russell’s viper & saw scaled viper). Maximum number of snake bite occurred in the monsoon season between July to November there is flooding habitats of the snakes. In present study, maximum incidence of snake bite was found in the age group between 1-60 years, attributed mainly for their outdoor activities in this age group. Similar findings were observed by Dr. Borkar MS et al. (Mangala, 2015). Snake bite can be said as an occupational disease since it is more common in farmers, lab ours & gardeners, Farmers constituted for 54%, lab ours accounted for 18% and housewives in 16% and 12% other of the snake bite cases. They are more prone for accidental snake bites while working. One more reason for higher incidence among famers & lab ours is bare foot walking while working (Halesha, 2013). This study showed increased incidence of snake bite areas where agricultural activities are more common. The main limiting aspects of treatment is expensive nature of ASV and many patients are purely depends on the Govt. Medical College & Hospital and sometimes losing their life while traveling a long distance (Barry, 2002). We noticed ???????????????? = 48.11688 in our epidemiological study that 12% of the cases were received within 2 hours of the snake bite, 45% between 2 to 4 hours, 30% between 4 to 12 hours, and 13 % between 12 to 24 hours. The delay in reaching our hospital can be attributed to distance from the village, traffic problem, poor transportation, facilities, lack of knowledge about the complication of snake bite, time may be wasted for application of tourniquet and herbal medicines Similar results were observed by Kulkarni ML, Anees S et al & Lahori UC, Sharma DB et al (Yogendra Kumar Gupta, 2014). In developing country like India, where the supply of ASV is far less than the demand. We have to use this precious life- saving drug very conservatively and judiciously. Snake Venom Antiserum (Polyvalent), in India is a refined preparation of serum globulins obtained by fractionating blood from healthy hyper immunized horses where each ml of which neutralizes the following quantities of standard venoms tested in mice by intravenous route. Cobra 0.6 mg, Common Krait 0.45 mg, Russell's Viper 0.6 mg and Saw-scaled Viper 0.45 mg (Bawaskar, 2004). This study is epidemiological type (an observational prospective study), which is the result of a -no choice situation. Around 2007, we started facing a shortage of ASV. Earlier, we used to give 100 to 200 ml of ASV in patients of poisonous snake bite, though in a steady, single infusion. Many of the other physicians in this department used to prescribe 10 - 100 cc as 6 hourly doses. We believe that whatever dose is to be given should preferably be given as a single dose. In the vast majority of cases in this region of Marathwada in Maharashtra state of India, very low dose of ASV (about 50 ml or less) given as a single infusion over 2 hours is adequate to save cases of poisonous snake bites, Anti-venom treatment can be expected to neutralize free circulating venom, Prevent progression of envenoming and allow recovery. However, these processes take time and the severely envenomed patient may require life support systems such as treatment of shock, assisted ventilation and renal dialysis until the severely damaged organs and tissues have had time to recover. If an adequate dose of appropriate anti-venom has been administered, the following responses may be observed.
Therefore, appropriate to give anti-venom for as long as evidence of the Coagulopathy persists. Whether anti-venom can prevent local necrosis remains controversial, but there is some clinical evidence that, to be effective in this situation, it must be administered within the first few hours after the bite. Majority of the victims 98 had bites on lower limb followed by bites on upper limb 57 and remaining 28 with sites among the 156 cases. A similar observation was made in the study conducted by Dr. M. S. Borkar et.al. Showing in Table no.6 & Graph no. 5
CONCLUSION
The epidemiological study shows the epidemics of the ASV use, those who came earlier to hospital required a low dose of ASV to save lives of victims of poisonous snake bites with good supportive management (Paul, 2004). The percentage of venomous snake bite is decreased as compared to 2013 and 2014 with an average dose of 48.11 ASV required. In past, we use ASV at once only but modern anti-venoms cause very few side effects for most people, even when they get them a second time. In the past, most anti- venoms were of the old-fashioned allergy-provoking type, and back then some doctors and many snake experts avoided risking a second use of anti-venom. The reason was that a person’s immune system might recognize the animal serum in the anti-venom, and there might be either a serious allergic reaction or a severe case of “serum sickness.” But even back then, many people got anti- venom a second (or third, or fourth…) time, often by using allergy medications at the same time (Debnath, 2007).
REFERENCES

Pratima Tighade*, Dr. Sachin Hangargekar, Dr. Vishweshwar Dharashive, Epidemiological Study of Anti-Snake Venom Use in Snake Bite Patients, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 1135-1143 https://doi.org/10.5281/zenodo.17090189
 10.5281/zenodo.17090189
10.5281/zenodo.17090189