Shri Venkateshwara college of pharmacy. Ariyur, Puducherry, India.
Chronic obstructive pulmonary disease (COPD) plays a significant role in global morbidity and mortality rates, typified by progressive airflow restriction and lingering respiratory symptoms. Recent explorations in molecular biology have illuminated the complex mechanisms underpinning COPD pathogenesis, providing critical insights into disease progression, exacerbations, and potential therapeutic interventions. This review delivers a thorough examination of the latest progress in molecular research related to COPD, involving fundamental molecular pathways, biomarkers, therapeutic targets, and cutting-edge technologies. Key areas of focus include the roles of inflammation, oxidative stress, and protease–antiprotease imbalances, alongside genetic and epigenetic factors contributing to COPD susceptibility and heterogeneity. Comprehending the molecular foundation of COPD carries substantial potential for the creation of tailored treatment strategies and the enhancement of patient outcomes. By integrating molecular insights into clinical practice, there is a promising pathway towards personalized medicine approaches that can improve the diagnosis, treatment, and overall management of COPD, ultimately reducing its global burden.
COPD is defined as Chronic obstructive pulmonary disease it is the airflow restriction that does not change significantly over several months. The condition consists of chronic bronchitis, small airways disease (bronchiolitis), and emphysema in varying proportions across individuals. COPD is a leading cause of illness and mortality worldwide. Tobacco exports to developing countries like India, Mexico, Cuba, Egypt, South Africa, and China are expected to significantly boost the prevalence of smoking among Western women. Asthma is a significant health risk, but there are few treatment choices available, with most drugs specifically designed for this condition. To develop effective COPD medications, it's important to study the disease's epidemiology, natural history, genetic and environmental risk factors, and pathophysiology. This review paper comprise of Epidemiology, Pathophysiology, Etiology, Diagnosis, Risk Factors, Treatment.
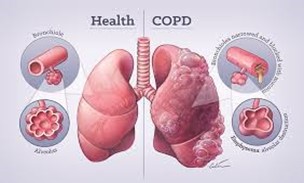
Fig: 1
Epidemiology:
COPD is the worldwide cause due to the expouse to the toxic substance. The world's population is aging, smoking rates are rising, and deaths from ischemic heart disease and infections are decreasing. Chronic obstructive pulmonary disease (COPD) is the world's fourth biggest cause of death, accounting for 3.5 million deaths in 2021, or almost 5% of total global deaths. Low- and middle-income countries (LMIC) account for about 90% of COPD fatalities among those under the age of 70.COPD is the eighth biggest cause of poor health worldwide, as defined by disability-adjusted life years. Tobacco use is responsible for nearly 70% of COPD cases in high-income nations. Tobacco use accounts for 30-40% of COPD cases in low- and middle-income countries, and household air pollution is a key contributor (1). Although marketed as a nicotine replacement medication, vaping has become a technique for attracting nonsmokers. Tobacco is a prominent ingredient in several vaping and e-cigarette products. Nicotine has been flavored with THC, CBD oils, Vitamin E, and other ingredients to appeal to non-smokers and young adults (2-5). COPD is a prevalent and curable illness affecting 5-22% of adults over 40. COPD is a prominent cause of hospitalization and has significant healthcare costs. 6-8 According to Gershon et al., the annual COPD incidence is 5.9 cases per 1000 people. The study found a lifetime COPD risk of 26.6%. The risk was higher for men, smokers, those over 40, and those living in rural regions. More people will be diagnosed with COPD than with heart failure, acute myocardial infarction, or some malignancies (9). There is insufficient evidence to accurately evaluate the morbidity, death, and overall burden of COPD. The majority of COPD estimations lack consistency and may be underestimated (6, 10, 11). The CDC reported that 9.0 million persons were diagnosed with chronic bronchitis in 2018. 3.6 percent of individuals were diagnosed with chronic bronchitis in the same years. Emphysema affects around 3.8 million individuals, or 1.5% of the population.
Pathophysiology:
Etiology:
Etiology of COPD are as follows:
The primary risk factor for COPD is tobacco use.15, 16 In high-income nations, tobacco use accounts for more than 70% of COPD cases, whereas in low- and middle-income countries, it accounts for 30% to 40% of cases. The effects of smoking include oxidative damage, cilia malfunction, and an inflammatory response.17 Additional etiologies include indoor biomass fuel combustion, air pollution, and occupational exposure to dust, chemicals, and fumes.18,19,20 Both high levels of particulate matter and large dosages of pesticides are associated with a higher risk of COPD(21,22,23,24)The pathophysiology of COPD also includes oxidative stress and an imbalance in proteases and antiproteases, particularly in those with alpha-1 antitrypsin deficiency25. Processes that impact proper lung development and, therefore, lung function can raise the chance of developing COPD.26 These processes may have their origins in childhood, adolescence, pregnancy, and delivery. Cigarette smoke contains dangerous compounds that cause lung tissue damage, oxidative stress, and chronic inflammation. The airways and alveoli undergo structural alterations as a result of this exposure, including:
2. Genetic Factors
The best-defined causal genetic illness is alpha-1 antitrypsin deficiency, which is a major cause of emphysema in nonsmokers and significantly increases disease vulnerability in smokers. More than 30 genetic variants have been linked to COPD or deterioration in lung function in specific populations, but none have been proved to be as significant as alpha-1 antitrypsin13
3. Environmental Exposures
Other inhalational exposures that can lead to COPD include:
• Indoor air pollution is prevalent in LMICs where biomass fuels (e.g., wood or animal dung) are used for cooking and heating.
• Long-term exposure to dust, chemicals, and odours in work places can raise the risk.
• Air pollution is a major contributor, especially in cities.
4. Early Life Factors:
Several early-life circumstances, such as poor fetal growth, premature birth, and severe respiratory infections during childhood, might impede optimum lung development and raise the risk of having COPD later in life.
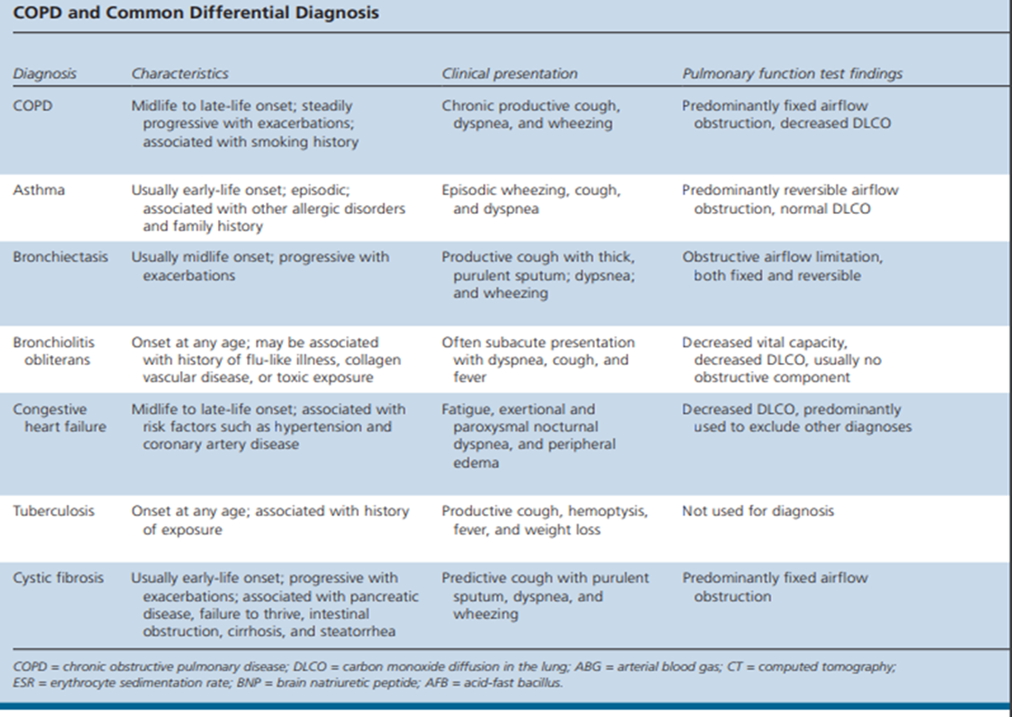
DIAGNOSIS:
Table: 1 COPD and Common Differential Diagnosis
Risk Factors
The most commonly reported risk factors for COPD include:
TREATMENT:
COPD is not treatable, however it can be improved by quitting smoking, reducing air pollution, and obtaining immunizations. It is treatable with medications, oxygen, and pulmonary rehabilitation. There are numerous therapies for COPD. The most common treatments are inhaled medications that open and relieve edema in the airways. Bronchodilator inhalers are the most significant medications for treating COPD. They relax the airways so that they remain open. Short-acting bronchodilators work quickly and can last up to 4-6 hours. These are commonly utilized during flare-ups. Long-acting bronchodilators take longer to work, but they last longer. These are given once day and can be supplemented with inhaled steroids.
Additional therapies may be used:
Living with COPD
RESULT
In summary, there is a considerable call among members of the scientific community to try to find an ideal way to identify COPD patients at the onset of their disease, given that early interventions can have a great impact on the future burden of the disease or its prognosis. The concepts reviewed here constitute an initial approximation of the different forms that COPD can have at its onset.
Compliance with ethical standards
We would express our sincere gratitude to all those who have given valuable guidance and support throughout the research process. Those supports help in shaping our research and helping us to overcome challenges.
REFERENCES

Indumathy. K., Priyadharshini S., Jayaramanan Rajangam, Thanushree V.S., Shivashakthi P., Exploring The Comprehensive Review of Diagnostic Method of Chronic Obstructive Pulmonary Disease: A Global Scenario, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 12, 2820-2827. https://doi.org/10.5281/zenodo.14542901
 10.5281/zenodo.14542901
10.5281/zenodo.14542901
