
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Bengal College of Pharmaceutical Sciences and Research, Durgapur, West Bengal
The allopathic healthcare system provides two conventional ways of treatment for rheumatoid arthritis, both of which have side effects. As a result, turning to Ayurvedic herbal treatment formulation that is safe, effective, and proven would be a better choice. Rheumatoid arthritis is an autoimmune disease that is chronic and progressive, distinguished by chronic inflammation affecting the peripheral joints. Transdermal films containing herbal medicinal plants such as Cardiospermum helicacabum and Aloe barbadensis were designed in this study to treat rheumatoid arthritis . The solvent casting method was used to develop transdermal patches using plant extracts. The patches were evaluated based on physicochemical parameters such as thickness, folding endurance, physical appearance, weight uniformity, moisture content, drug content, flatness, moisture uptake, pH, and invitro drug release and stability study. The plots for average absorbance release vs time through transdermal film shows that drug release occurred at a steady rate. The skin irritation study on human volunteer's skin revealed that the formulation does not cause skin irritation. Overall, the present research provides a novel approach to the implementation of transdermal drug delivery techniques in the design of herbal remedies. Currently, herbal drugs are the focus of numerous studies on novel drug delivery systems. The curcumin transdermal medication conveyance framework was developed and evaluated. Curcumin, the active component of curcuma longa (haldi), has a place in the family Zingiberaceae and is currently being used as an anti-inflammatory specialist against rheumatoid joint pain in this audit. Curcumin's transdermal patch makes use of a variety of polymer blends to improve therapeutic efficacy and reduce side effects. The depiction, dissolvability, and similarity studies completed the medication's detail concentrates. Three formulas were created by combining 20 milligrams of curcumin with a variety of polymer concentrations of hydroxy propyl methyl cellulose (HPMC), methyl cellulose (MC), and ethyl cellulose (EC), respectively. Solubility was tested in water, phosphate buffer pH 7.4, ethanol, DMSO, and tetrahydrofuran (THF), respectively.
The skin is the largest organ in the human body, covering about 1.5 to 2.0 square meters in adults. Throughout history, people have used the skin as a gateway for medicine, applying treatments to heal wounds, manage illnesses, and enhance beauty. Ancient civilizations, such as the Egyptians and Babylonians around 3000 BC, used salves, ointments, and even early versions of patches made from plant, animal, and mineral extracts.
However, transdermal drug delivery as we know it today— where medications are precisely and consistently absorbed through the skin into the bloodstream—only became common in the late 20th century. Advances in technology made it possible to control drug release, ensuring safe and effective treatment for various conditions.

Fig. 1
Transdermal patches have become a popular way to deliver medications and cosmetic treatments through the skin. These patches are the result of years of research, trial and error, and scientific advancements in skin science and drug delivery.
This review takes a journey through the history of topical treatments, from the earliest ointments to modern transdermal patches. It explores the early experiments, devices, and drug delivery methods that led to today's patch technology. We also look at the current transdermal products available, addressing concerns like product consistency, safety, and regulatory considerations. Finally, the review highlights exciting future developments, such as enhanced patch designs, microneedle technology, and new skin-based delivery systems like metered- dose sprays.[1]
Rheumatoid arthritis is a long-term autoimmune disease that causes chronic inflammation in the joints, leading to cartilage damage, bone erosion, and, over time, irreversible joint deformities and loss of function. Treatment mainly focuses on reducing inflammation by regulating inflammatory responses in the body.
Transdermal drug delivery is emerging as a promising approach for managing rheumatoid arthritis. By allowing medications to pass through the skin, this method can bypass the digestive system, reducing stomach-related side effects and avoiding the first-pass metabolism in the liver. This improves drug absorption and helps control inflammation more effectively.
This paper explores the latest advancements in transdermal drug delivery for rheumatoid arthritis. It discusses various innovative formulations, including gels (such as nano emulsion, nano micelle, and ethosomal gels), patches, drug-loaded microneedles, nanostructured lipid carriers, transfersomes, lyotropic liquid crystals, and electrospun nanofibers. These developments open up new possibilities for more effective and convenient treatments for rheumatoid arthritis.[2]
TRANSDERMAL PATCH
A transdermal patch is a simple and effective way to deliver medication through the skin directly into the bloodstream. The first transdermal patch was approved by the FDA in 1981, and since then, this method has been widely used for various treatments. Today, transdermal patches are available for motion sickness (scopolamine), cardiovascular conditions (clonidine and nitroglycerin), chronic pain (fentanyl), and smoking cessation (nicotine).

Fig. 2
One of the biggest advantages of transdermal drug delivery is that it provides a steady, controlled release of medication, avoiding the spikes and drops that can happen with oral or injectable drugs. This is particularly helpful for medications with short half-lives, as it ensures a continuous and consistent effect.
Compared to traditional oral or injectable medications, transdermal patches are gentler on the digestive system and liver, improving patient comfort and reducing side effects. They are also convenient—some patches only need to be applied once a week—making it easier for patients to stick to their treatment plan. This ease of use and improved drug absorption make transdermal patches a valuable option in modern medicine.[3]
Key Components of a Transdermal Patch
A transdermal patch consists of several essential components, each playing a crucial role in delivering medication effectively through the skin.
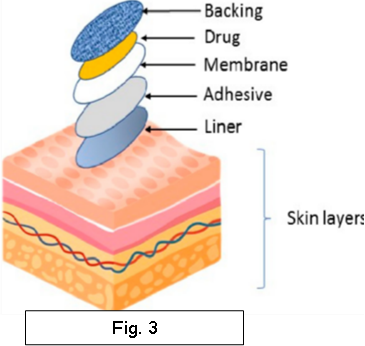
Each of these elements plays a role in making transdermal patches a reliable and convenient way to deliver medications.[4]
Biopharmaceutical Parameters for Drug Selection in Transdermal Patches
When selecting a drug for transdermal patch delivery, several biopharmaceutical factors must be considered to ensure effective absorption and therapeutic efficacy. These include:
Approaches Used in the Development of Transdermal Patches
In this system, the drug reservoir is completely enclosed within a shallow compartment made of a drug-impermeable metallic plastic laminate. The release of the drug is controlled by a polymeric rate-controlling membrane.
The rate-controlling membrane can be either microporous or non-porous, with ethylene vinyl acetate (EVA) copolymer being a common choice.
This is the simplest version of the membrane-moderated drug delivery system. In this approach, the drug reservoir is created by directly dispersing the drug into an adhesive polymer. The medicated adhesive is then spread onto a flat, drug-impermeable metallic plastic backing using a solvent-casting method, forming a thin drug reservoir layer.
In this system, the drug reservoir is created by evenly dispersing drug solids within a hydrophilic or lipophilic polymer matrix. The resulting medicated polymer is then molded into a disc with a defined area and thickness.
The micro-reservoir system is a hybrid approach, combining features of both reservoir and matrix dispersion systems.[6]
Challenges and Recent Advances in Plant-Based Drug Discovery
Scientists are constantly working to improve both the quality and quantity of natural compounds entering the drug development pipeline. However, discovering and developing plant-based drugs is often more time-consuming and complex compared to other drug discovery methods.
To advance research in this field, collaboration across multiple disciplines such as biology, chemistry, ecology, and nutrition is essential.
Recent Advances in Plant-Based Drug Discovery:
Advanced Analytical Techniques – Modern tools like Nuclear Magnetic Resonance (NMR) spectroscopy and Mass Spectrometry (MS) help isolate and identify plant-derived compounds.
High-Throughput X-ray Crystallography – This technique aids in understanding the structure of medicinal plant compounds, which is crucial for drug design.
Herbal Compound Libraries – Creating databases of herbal compounds and their derivatives can enhance drug discovery by combining traditional herbal knowledge with modern combinatorial chemistry.
Despite the challenges in plant-based drug discovery, natural compounds will continue to play a significant role in developing new medicines. Research in this field is ongoing, offering great potential for future breakthroughs.[7]
Different Carriers for Novel Drug Delivery Systems of Herbal Drugs
Novel drug delivery systems aim to maximize therapeutic efficacy with minimum dosage, ensuring targeted delivery of herbal compounds for better results. Various carriers are used in these advanced delivery methods, including:
The term ‘Phyto’ means plant, and ‘some’ means cell- like. Phytosomes are tiny, cell-like structures where biologically active herbal compounds are complexed with phospholipids, making them lipid-compatible. This patented technology improves the absorption of water-soluble plant extracts into the body.
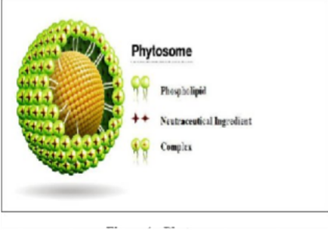
Fig. 4
Liposomes are microscopic vesicles made of one or more lipid bilayers, encapsulating hydrophilic substances in their aqueous compartments while integrating lipophilic drugs into the membrane. They are classified based on size, lamellae count, and surface charge (anionic, cationic, or neutral). Liposomal delivery improves the solubility, bioavailability, and stability of herbal compounds.
Nanoparticles range from 1-100 nm and consist of synthetic or semi-synthetic polymers. These tiny particles help target drugs more effectively, reducing degradation and interaction with other ingredients. Encapsulating herbal extracts in nanoparticles enhances solubility, absorption, and bioavailability, allowing for lower doses and improved therapeutic effects.
These are oil-in-water emulsions with particle sizes in the micron range, commonly used in veterinary applications due to their non-toxic and non-irritant nature. They allow prolonged drug release and help improve the concentration of herbal drugs in organs like the liver, kidney, and spleen.
Microspheres are spherical polymer-based carriers (1-300 µm) in which the drug is dispersed in a matrix. Drug release follows first-order kinetics, occurring either through matrix dissolution or surface erosion. The release rate depends on factors such as polymer type, size, and concentration.
Niosomes are vesicular drug carriers made of non-ionic surfactants (like alkyl polyglycerols) and cholesterol. They are similar to liposomes but are more stable, cost- effective, and capable of encapsulating a wide range of drugs. Various herbal drug formulations have been successfully developed using niosomes.
TDDS delivers medication through skin patches, allowing controlled drug absorption into the bloodstream. It is an effective alternative for drugs that are poorly absorbed orally. Examples include nicotine patches for smoking cessation and scopolamine patches for motion sickness, along with emerging herbal transdermal formulations.
These novel carriers enhance the efficacy and bioavailability of herbal drugs while reducing side effects and improving patient compliance.
Advantages of Transdermal Drug Delivery
Anti-rheumatic Herbal Patch
Rheumatic diseases have affected mankind since ages and are one of the commonest inflammatory conditions in developing countries. The main ingredients used in Anti-rheumatic herbal patches are Boswellic acid and Curcumin. Ethano botanically Boswellia serrata, Curcuma longa and Trichodesma indicum were used for antirheumatic, anti-inflammatory and in the treatment of different skin diseases. Waghulkar et al., (2011) developed the transdermal patches (films) for the antirheumatic activity by using chloroform extract of Trichodesma indicum and Boswellia serrata. Further research work also highlights on Curcuma longa that turmeric oil may be incorporated into the transdermal drug delivery system for their suitable and convenient use Vishwakarma et al., (2012). Studies have shown promising results; hence, there is a scope for further pharmacodynamic and pharmacokinetic evaluation.[9]
Fig. 5
ANTI-INFLAMMATION ACTIVITY
Discovering a single efficient bioactive compound from ginger which possesses anti- inflammatory property with better pharmacokinetics values, in turn will create a good impact on pursuing the suitable drug delivery mode with enhanced ratio of bioavailability. The inconveniences of the standard form of drug application and side effects due to the administration route are the reasons for studying the improvement strategies of bioavailability. Several active components are present in ginger among them major active ingredients are gingerol, shogaol, gingeberin and paradol. These components are used for treatment of inflammation, rheumatism, and bronchitis .Ginger extracts have been extensively studied for a broad range of biological activities including antibacterial, analgesic, anti-inflammatory, anti-tumor.[10]
DRUGS USED FOR TREATMENT OF RHEUMATOID ARTHRITIS AND INFLAMMATORY EFFECTS
Cinnamomum cassia Presl, a tree from the Lauraceae family, is known for its aromatic bark, commonly used as cinnamon. This spice is valued worldwide for its fragrance and spicy flavor, serving as both a kitchen staple and a key ingredient in traditional medicine.[11]
Native to China, India, Vietnam, and Indonesia, C. cassia is primarily cultivated in China’s Guangxi, Guangdong, Fujian, and Hainan provinces. Its bark, known as Cinnamomi cortex, is widely used in the West as a seasoning and food supplement, while in Asia, it plays a significant role in traditional medicine. Listed in the Chinese Pharmacopoeia since 1963, it is included in over 500 medicinal formulas to treat conditions such as cardiovascular and gastrointestinal diseases, gynecological disorders, and inflammation.

Fig. 6
Research has identified over 160 active compounds in C. cassia, confirming its diverse pharmacological benefits, including anti-inflammatory, antibacterial, antiviral, antitumor, and neuroprotective properties. The Chinese Pharmacopoeia continues to recognize Cinnamomi cortex as a valuable traditional medicine, using cinnamaldehyde content as a quality standard.[12]
Traditional Uses of Cinnamomum cassia
Cinnamomum cassia has a long history in traditional Chinese medicine, valued for its diverse therapeutic properties. Its medicinal use dates back to the Shennong Bencao Jing, an ancient Chinese medical encyclopedia from the Eastern Han Dynasty (25–220 AD), where it was prescribed for arthritis. Other classical texts also highlight its benefits—Mingyi Bielu describes its analgesic effects, while Yaoxing Lun records its use for bellyaches and menstrual pain.

Fig. 7
Throughout history, C. cassia has been mentioned in renowned medical texts such as Tangye Bencao, Bencao Gangmu, Bencao Jingshu, and Bencao Huiyan. Today, it remains a widely used traditional remedy for conditions like nephropathy, dysmenorrhea, irregular menstruation, and diabetes. To enhance its clinical applications, various modern formulations—including pills, capsules, granules, and oral liquids—have been developed for ease of use and effectiveness.[13]
Anti-Inflammatory and Pain-Relieving Effects of Cinnamomum cassia
Cinnamomum cassia has been widely studied for its ability to reduce inflammation and relieve pain. Its bioactive compounds, such as cinnamaldehyde and cinnamic acid, work by lowering inflammation-causing molecules and blocking pain pathways.
1. Anti-Inflammatory Properties
Studies have also shown that extracts from C. cassia can suppress inflammatory responses in immune cells (macrophages) by preventing the activation of important signaling pathways (JNK, p38, ERK1/2).[14]
2. Pain-Relief and Analgesic Effects
Overall, Cinnamomum cassia is a natural remedy with strong anti-inflammatory and pain- relieving properties, making it a promising alternative for treating arthritis, nerve pain, and other inflammatory conditions.[15]
Conclusions and Future Perspectives
In conclusion, the traditional usages, phytochemistry, pharmacological activity and toxicity of C. cassia have been summarized in the present review. Modern studies have confirmed that C. cassia has a wide range of pharmacological activities, including anti-tumor effects, anti- inflammatory and analgesic effects, anti-diabetic and anti-obesity effects, antibacterial and antiviral effects, for which it has been used in the clinic in many countries. Moreover, C. cassia has the same origin as a medicine and food which is often used as a condiment in our daily life. Nevertheless, there is still a lack of sufficient research about the alimento therapy, health products, toxicity and side effects of C. cassia. Therefore, more investigations need to be done in C. cassia in the future. Firstly, there is a lack of systematic toxicity and side effects studies of the extracts or compounds isolated from C. cassia. Essential oils are the main constituents of C. cassia, which has been reported to irritate the skin and possibly cause allergies, and the antibacterial effect of essential oil is applied in food and cosmetics. In addition, as a plant with the same origin as medicine and food, people will also eat C. cassia for a long time, therefore, in-depth investigations on its toxicity and side effects are a guarantee for the safe use of this plant.
Biological Name: Aloe barbadensis
Common Name: Curacao aloe, Lily of the desert
Family: Liliaceae
Aloe barbadensis is cultivated in Europe and in many parts of India, including the north-west Himalayan region. Aloe vera has been one of the most important plants used in folk medicine. Anthraquinone, anthracene, cinnamic acid and anthranilic acid are found in the Aloe vera plants that are responsible for its activity. Aloe vera is used in a variety of skin ailments such as mild cuts, insect stings, bruises, poison ivy and eczema. It also has antibacterial and antifungal properties, used as blood purifier, anti- inflammatory, diuretic, uterine tonic, spermatogenic, laxative, purgative and fever reliever. The anti arthritis property of aloe vera is due to the anthraquinone compound. Aloe vera stimulates the immune system and it is a powerful anti- inflammatory agent. Topical application of aloe vera extract result in the reduction of inflammation and arthritis in adjuvant induced arthritis in Sprague

Fig. 8
Therapeutic effects
Aloe vera is best known for its soothing and healing effects on burn and other wounds. Aloe vera when applied to wounds increases both the rate of wound closure and the tensile strength of the wound via the proliferation of cells . It does so by accelerating the flow of blood towards the wounded area. Aloe is the best wound dressing ever discovered. The mechanism explained behind t his acceleration is as follows: Aloe vera gel increases the collagen content and extent of collagen cross linking of the wound, resulting in enhanced wound contraction and breakage of scar tissue.Chithra et al. also reported the enhancement in content of hyaluronic acid and derm at an sulphate in the granulation tissue of healing wound. A 5.5 kDa glycoprotein, isolated from A. vera showed an increase in epithelial cell migration and enhanced wond healing process in a human keratinocyte monolayer.

Fig. 9
Aloe vera is currently utilized in manufacturing more than 95 % of the derm at ecologically valuable products. This is because it possesses implausible moisturizing properties. It improves the ability of skin t o hydrate itself and help in removal of dead skin cells. It does so by producing collagen and elastin fibers, making the skin more elastic and less wrinkled, thereby reversing the degenerative skin changes. It softens the skin, by its cohesive action on superficial flaking epidermal cells and also by the action of amino acids. For such incredible characters, Aloe vera is an ideal ingredient in cosmetics and dermatological procedures.
Inflammation is an innate response of the body against an injury, characterized by swelling, pain, redness and heat , resulting in delay in the healing process. The anti-inflammatory action of Aloe vera gel not only relieves pain and discomfort , but also accelerates the healing process. The effect observed for acetylated mannan in Aloe gel resembles the anti-inflammatory action of mannose-6- phosphate. Aloe vera also inhibit the cyclooxygenase pathway, reducing the production of prostaglandins, thereby reducing the inflammation. In a study conducted by Vazquez et al., the aqueous and chloroform extracts of Aloe vera were found to have anti oedema effects. Further, they were found to decrease the neutrophil count progressing towards the peritoneal cavity. A.vera also showed a great anti-inflammatory pot entry for the treatment of H. Pylori infection.
Studies have found that ingestion of Aloe vera on a daily basis can help prevent and cause a regression of arthritis. Aloe gel also reduces pain related to endinit and injuries. When applied directly to the area of pain, Aloe vera penetrates the skin to soothe the pain. Biological Vehicle: Act s as a biological vehicle to aid penetration and absorption of other bio- active ingredients into deep tissue.[17]
Aloe vera whole leaf, including the gel and latex, contains more than 200 phytocompounds (Davis, 1997). The gel contains more than 98% of water (Bozzi et al., 2007). The solid content of the gel is about 0.66% and about 0.56% solid content is soluble in different solvents. However, the chemical composition, potency and amount of the constituents are influenced by changes in the seasons, soils, climatic conditions, extraction and harvesting methods and shows fluctuation (Boudreau and Beland, 2006; Rodriguez Rodriguez et al., 2010).
The growth stages also contribute to its phytochemical constituents (Hu et al., 2003). The solid portion of the gel consists of about polysaccharides (~55%), sugars (~17%), minerals (~16%), proteins (~7%), lipids (~4%) and phenolic compounds (~1%) (Luta and McAnalley, 2005). It contains vitamin A, C, E, thiamine, niacin, riboflavin, choline and folic acid as well (Lawless and Allen, 2000). Vitamin B12 is also found in trace amounts which are generally available from animal sources (Coats 1979; Atherton, 1998).
Ethnic and medicinal usage of the plant
Aloe vera has been documented as a pharmaceutical remedy since ancient times, with references dating back to Mesopotamian (1750 B.C.E.) and Egyptian (550 B.C.E.) civilizations. Greek physician Dioscorides (74 B.C.E.) described its use for wound healing, infections, hair loss, and hemorrhoids.
Modern research on Aloe vera began in 1935, when it was reported as a treatment for radiodermatitis. Subsequent studies highlighted its effectiveness in treating burns, inflammation, and various ailments. The plant holds significance in Indian Ayurveda, where it is used as a tonic, purgative, and treatment for respiratory and digestive issues.
Recent studies have expanded its medicinal applications, demonstrating its efficacy in reducing alcohol-induced gastritis, enhancing wound healing, and modulating inflammatory responses. Aloe vera has also shown promising results in experimental models of diabetes, liver damage, ischemia-reperfusion injury, and even cancer. Additionally, its active compound, Aloe-emodin, has exhibited anti-rheumatoid arthritis properties.
Overall, Aloe vera continues to be a subject of interest in complementary and alternative medicine due to its broad therapeutic potential.
Cytokines, Cox-2, and RA Pathogenesis Cytokines such as TNF-α, IL-1β, and other interleukins play a crucial role in RA progression by facilitating immune cell infiltration in inflamed joints. Cox-2, which promotes prostaglandins, is a key driver of inflammation and pain in RA. Clinical trials have demonstrated that cytokine and Cox-2 inhibitors can effectively reduce RA symptoms when used alone or in combination with conventional therapies.
Plant-Based Compounds in RA Management
Besides conventional drugs, plant-based compounds have shown potential in modulating cytokine activity, as observed in in silico, in vivo, and cell culture studies.
While Aloe vera has shown promising interactions with inflammatory markers in silico studies, its role in RA remains insufficiently explored in animal models. More comprehensive in vivo studies are required to confirm its efficacy in reducing inflammatory symptoms associated with RA. Plant-derived compounds show strong potential in managing RA by modulating cytokine activity and inflammatory pathways. While many herbal extracts have been studied in animal models, Aloe vera's anti-RA effects need further exploration to establish its role as a complementary treatment for inflammatory arthritis.
Conclusion
Aloe vera is a medicinal plant that has been used since ages for its diverse therapeutic properties. The chemical composition of Aloe vera is particularly interesting as several of its components have therapeutic and pharmacological properties. The cultivation of Aloe vera has acquired great commercial importance for medicinal products and cosmetics. Farmers in India regularly face problems like lack of rain, low groundwater level, soil degradation etc. Aloe vera is cultivable in diverse ecological habitats and its cultivation can provide regular income and high returns on investment.[18]
As a member of the Zingiberaceae family, turmeric (Curcuma longa) is perhaps the most important plant used in herbal medicine. The Arabic term "Kourkouma," which implies saffron, is the source of the Latin name "Curcuma." It expands in warm,humid situations that are humid and call for lots of water.
It has big, oblong leaves and a short pseudostem. There is a parent, or mother, rhizome and several branching subsidiary rhizomes within the subterranean rhizome.
Turmeric's vivid yellow color also gives it the nickname "Indian saffron." Turmeric's main constituent, diferuloylmethane, or curcumin, is a yellow pigment that gives it its unique qualities.[19]

Fig. 10
Turmeric plants have long, simple leaves with long petioles, or leaf stems, and grow to a height of about one meter (3.3 feet)... The leaves emerge from the branching rhizomes that are slightly below the soil's surface, the leaves emerge. Younger rhizomes are pale, whereas older rhizomes are slightly scaly and brown in color. While young rhizomes are pale from yellow to orange- brown. The tiny yellow-orange blossoms are carried in the axils of waxy bracts, which are often light green or somewhat purple in hue. It was used as a spice and a perfume in antiquity. The rhizome smells like pepper, tastes warm and slightly bitter, and is a bright orange-yellow color that stains well. In addition to Africa, it is grown in China, India, Indonesia, Thailand, and other tropical countries.Based on the region of production, the two primary commercial varieties of turmeric in India are "Madras" and "Alleppey" turmeric.
While the British and Middle Eastern markets favor Madras turmeric, which has less curcumin and volatile oils, the United States imports Alleppey turmeric as a spice and food colorant. Madras turmeric is ideal for curry powder and mustard paste because of its brighter, lighter yellow color. The "Bengal" variety is mostly utilized as a coloring agent. Turmeric has historically been utilized in Eastern Asian medical systems, including traditional Chinese medicine, as well as Ayurveda and other traditional Indian medical systems. It was customary in India to utilize conditions pertaining to the joints, digestive system, skin, and upper respiratory tract.[20] Curcumin an important constituent of turmeric, has been reported to alter the nuclear factor (NF) kappaB transcription activity, inhibit prostaglandin E2 production and COX-2 expression, thereby acting effective healing agent(21).

Fig. 11
Effect of turmeric and curcumin on arthritis
Multiple studies proved curcumin therapeutic effect against the progression of arthritis. Arthritis has a strong inflammatory background. The main cytokines involved in the inflammatory cascade of arthritis are tumour necrosis factor-α (TNF-α), interleukin (IL)-6, and IL-1 [22]. Studies show that curcumin inhibits the production and activity of main inflammation-associated markers, such as TNF-α, nuclear factor-κB (NF-κB), cyclooxygenase-2 (COX-2), mammalian target of rapamycin (mTOR), interleukins.
This effect enables curcumin to reduce inflammation in diseases like arthritis, psoriasis, inflammatory bowel disease, and asthma. Turmeric has been used medicinally throughout Asia to treat stomach and liver ailments and has been used externally to help the healing of wounds and bruises, and still applied to all sorts of skin conditions—from smallpox and chickenpox to blemishes, shingles, minor cuts, and burns.[23]
Turmeric, particularly its active component curcumin, exerts its therapeutic effects in arthritis primarily through its potent anti-inflammatory and antioxidant mechanisms.
In arthritis, especially in conditions like osteoarthritis and rheumatoid arthritis, chronic inflammation leads to joint damage and pain. Curcumin works by inhibiting several molecules and pathways involved in inflammation. It suppresses the activity of nuclear factor-kappa B (NF-κB), a protein complex that regulates the expression of various pro-inflammatory genes, including cytokines like tumor necrosis factor-alpha (TNF-α), interleukin-1 (IL-1), and interleukin-6 (IL-6), which are key mediators in joint inflammation. Additionally, curcumin inhibits cyclooxygenase-2 (COX-2) and lipoxygenase (LOX) enzymes, both of which are involved in the synthesis of inflammatory mediators such as prostaglandins and leukotrienes. These actions collectively reduce the inflammatory response in the joints, thereby relieving pain, swelling, and stiffness.[24] Curcumin also exhibits strong antioxidant activity by neutralizing free radicals and enhancing the activity of endogenous antioxidant enzymes like superoxide dismutase (SOD), catalase, and glutathione peroxidase. This reduces oxidative stress in joint tissues, which is another contributor to cartilage degradation in arthritis. Furthermore, curcumin modulates the immune response by inhibiting T-cell proliferation and reducing the activity of B-cells, which helps in managing autoimmune aspects of rheumatoid arthritis. Due to its poor bioavailability when taken orally, curcumin is often consumed with black pepper (which contains piperine) or fats to enhance absorption. With regular use, turmeric can significantly alleviate the symptoms of arthritis by interrupting the inflammatory cascade and protecting joint tissues from oxidative damage.[25].
Major Chemical Constituents
Turmeric (Curcuma longa) contains several bioactive constituents that contribute to its wide range of medicinal properties, the most important of which are the curcuminoids.
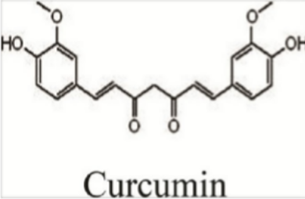
Fig. 12
The primary curcuminoid is curcumin, which is well known for its powerful anti-inflammatory, antioxidant, anticancer, and antimicrobial effects.
Along with curcumin, turmeric also contains demethoxycurcumin and bisdemethoxycurcumin, which exhibit similar therapeutic activities but in varying degrees of potency.
In addition to curcuminoids, turmeric is rich in essential oils, such as turmerone, atlantone, and zingiberene, which possess antimicrobial, antifungal, and neuroprotective properties. Ar- turmerone, in particular, has been shown to support neural regeneration and improve cognitive function.
Another important group of compounds in turmeric are polysaccharides, especially Ukonan A, B, C, and D, which have been studied for their immune-boosting, anti-tumor, anticoagulant, and blood sugar-lowering effects. Furthermore, turmeric contains small amounts of essential vitamins and minerals, such as vitamin C, vitamin E, potassium, iron, manganese, and zinc, which help support immune function, antioxidant defense, and metabolic activities. The combination of these constituents makes turmeric a powerful medicinal herb used traditionally and scientifically for managing a variety of chronic diseases, including arthritis, cancer, diabetes, and neurodegenerative conditions.[26]
Conclusion
Curcumin, the principal bioactive compound of turmeric (Curcuma longa), has emerged as a promising natural agent in the management of arthritis due to its strong anti-inflammatory, antioxidant, and immunomodulatory properties. It effectively inhibits key inflammatory mediators such as NF-κB, COX-2, TNF-α, and various interleukins that are involved in the pathogenesis of both osteoarthritis and rheumatoid arthritis.
Additionally, its ability to neutralize free radicals and enhance antioxidant enzyme activity helps protect joint tissues from oxidative damage. Clinical studies and meta-analyses have shown that curcumin supplementation can significantly reduce joint pain, stiffness, and swelling, often with fewer side effects compared to conventional non-steroidal anti- inflammatory drugs (NSAIDs).
Although its bioavailability remains a challenge, this can be improved through co- administration with piperine (from black pepper) or fats.
Given its safety profile, cost-effectiveness, and therapeutic potential, curcumin stands out as an effective adjunct or alternative treatment option for arthritis, warranting further development as a natural anti-arthritis drug.
4. PAEONIA LACTIFLORA
Paeonia lactiflora Pallas (family Ranunculaceae), also named Chinese Paeony, is a herbaceous perennial herb and is also widely grown as an ornamental plant in gardens, with several hundred selected cultivars; many of the cultivars have double flowers, with the stamens modified into additional petals.

Fig. 13
It flowers in the late spring. The flowers are very beautiful with various colours, so they are awarded the fame of “love flower” in China.
Radix Paeoniae is the dried root of P. lactiflora Pallas, which is cylindrical, straight, or slightly curved, 5–20 cm long and 1 -- 2.5 cm in diameter. It is used as a medicinal herb in traditional Chinese medicine, where it is called (pinyin: sáo tàu; literally: “Paeony Medicine”).A water/ethanol extract of Radix Paeoniae Alba is known as total glycosides of paeony (TGP), of which paeoniflorin is the major active component [27].
Paeoniflorin (C23H28O11, with a molecular weight of 480.45) is a water-soluble monoterpene glycoside, the content of which constitutes>90% of TGP and 0.05–6.01% of Radix Paeoniae Alba. The content of paeoniflorin is used for the standardization of the dosage of TGP in modern medicine. Orally administered paeoniflorin is metabolized into three metabolites, paeonimetabolin I–III, by intestinal bacteria [28].
A decoction of Radix Paeoniae has been used in the treatment of headaches, dizziness, costal and abdominal pain, spasmodic pain of the limbs, anemia, menstrual disorders, spontaneous sweating and night sweating in traditional Chinese medicine with a long history. In recent decades, Radix Paeoniae Alba has been found to be effective in the treatment of rheumatoid arthritis (RA), systemic lupus erythematosus, hepatitis, and other inflammatory/autoimmune diseases. The main pathological change of RA is characterized by hyperplasia of synovial membrane, infiltration of inflammatory cells, and neovascularization, which finally lead to cartilage erosion and articular destruction. In recent years, a lot of studies describing the analgesic, anti-inflammatory, and immunomodulatory effects of TGP or paeoniflorin have been published. Here, we briefly reviewed the possible mechanisms responsible for the therapeutic effects of TGP in RA. Paeonimetabolin-I, a major metabolite, is demonstrated to be a potent anticonvulsant [29].
Anti-inflammatory effects
Chronic and persistent inflammation in the synovial membrane is the pathological basis of RA. The direct anti-inflammatory effects of TGP were observed in various animal models of both acute and chronic inflammation, such as dimethylbenzene-induced ear swelling, carrageenan- induced paw edema, subcutaneous tampon induced granuloma, complete Freund's adjuvant- induced arthritis (AA), and collagen-induced arthritis (CIA) [30]. In both AA rats and CIA rats intragastric administration of TGP (25–100 mg/kg/d) for 7–14 days significantly diminished the severity of hind paw swelling and the scores of polyarthritis in a dose-dependent manner. Histological examination demonstrated that the synovial infiltration of lymphocytes was also markedly inhibited by TGP [31].
Similar effects of paeoniflorin on the severity of hind paw swelling and the scores of polyarthritis were also confirmed in the rats with experimental arthritis [32]. In addition, intraperitoneal injection of paeoniflorin inhibited the severity of intratracheal instillation of lipopolysaccharide (LPS)-induced acute lung injury in mice by suppressing inflammatory cell infiltration and lowing microvascular permeability [33]. Subcutaneous injection of TGP also inhibited capillary permeability associated with inflammation induced by intraperitoneal injection of acetic acid in mice [34].
These data support that Radix Paeoniae suppresses both acute and chronic inflammation by lowing microvascular permeability and inhibiting the infiltration of inflammatory cells. Further evidences indicate that TGP or paeoniflorin exerts anti-inflammatory effect by inhibiting the production of inflammatory mediators, such as prostaglandin E2, leukotriene B4, nitric oxide, reactive oxygen species and proinflammatory cytokines.
Clinical aspects
There have been numerous clinical reports on the efficacy and safety of TGP in various diseases. Unfortunately, few of them have been substantiated by randomized controlled trials with large sample sizes. The first prospective, double- blind trial of TGP was conducted in 1993, and 450 patients with RA were randomized to receive oral TGP (1.8 g/d)or methotrexate (10 mg/w) for 12 weeks.

Fig. 14
Therapeutic response was achieved in 71.7% of TGP-treated patients and 81.7% of methotrexate treated patients, respectively. The side effects of TGP occurred in 13.3% patients, and most of them were gastrointestinal tract disturbances, especially mild diarrhea.
They will be self-resolved in 1–2 weeks. No adverse effects on hepatic, renal and hematological tests were found. The similar results were observed in a phase III clinical trial of 1016 patients with RA [35]. A preparation of TGP was approved by the State Food and Drug Administration of China to enter the market as a disease-modifying drug for RA in 1998. However, there is no report available to show whether TGP treatment retards the radiographic progression of the disease. Some pilot studies also showed therapeutic benefits of TGP in systemic lupus erythematosus [36], Sjögren syndrome, ankylosing spondylitis , chronic urticaria , et al. Reports of traditional use indicate that Radix Paeoniae may have abortifacient activity, so the use of Radix Paeoniae is contraindicated in pregnancy.
Conclusion
Radix Paeoniae is the dried root of P. lactiflora Pallas, which is widely used in traditional Chinese medicine. Paeoniflorin is the major component of the active monoterpene glycosides extracted from Radix Paeoniae.
Numerous preclinical studies have demonstrated the analgesic, anti-inflammatory, immunomodulatory and cartilage protective effects of TGP/ paeoniflorin in vitro and in vivo.
It exerts antiinflammatory effect by inhibiting the production of inflammatory mediators, such as prostaglandin E2, leukotriene B4, nitric oxide, reactive oxygen species and proinflammatory cytokines, from lymphocytes, macrophages and fibroblast-like synoviocytes.
It also inhibits chemokine production from endothelial cells, induces the production of antioxidants and decreases micro-vascular permeability. It balances the differentiation and function of Th1 and Th2 cells, inhibits the proliferation of lymphocytes, and induces apoptosis of lymphocytes. It also inhibits the activation of neutrophils. TGP/paeoniflorin may alleviate the synovial hypertrophy and joint destruction of RA by anti-inflammation, anti-proliferation of synoviocytes, anti-neovascularization and reduction of cartilage-degradation enzymes. Clinical data support the therapeutic efficacy of TGP in RA without severe adverse effects, but no evidence demonstrates whether TGP retards the radiographic progression of RA.
5. TRIPTERYGIUM WILFORDII
Tripterygium wilfordii Hook. f. is a traditional medicinal plant originally found in Taiwan. It has been known in Europe since the late 1850’s but has not been widely investigated in the West before the 1970’s. In the last few decades increasing efforts have been made to elucidate its value as an antiinflammatory and immunosuppressive agent , in particular for the treatment of rheumatoid arthritis.[37] It is also regarded to be a cytotoxic drug, a male contraceptive, a treatment option for idiopathic refractory nephrotic syndrome, various gynecologic diseases and others.
It contains considerably toxic compounds which lead to a basically negative benefit-risk ratio. On the other hand this obstacle might be overcome by structural modification of the constituents which may also serve as lead compounds for further drug development.
Scientific interest in this plant continuously rose during the last 40 years as did the number of publications on this medicinal plant .
The plant is said to be already mentioned in the Chinese herbal “Dian Nan Ben Cao” written in the 15th century by Mao Lan, and, according to Lipsky and Tao (1997), the ‘Compendium of Materia Medica” compiled by Li Shi-Zheu in 1578, also reported a variety of medicinal uses.[38]

Fig. 15
The internationally accepted name of the plant is Tripterygium wilfordii Hook f., in China the terms “Lei Gong Teng” “and ‘Thunder God Vine’ are common. The usual German expression is, even though the roots are the source of therapeutically useful extracts, “Wilfords Dreiflügelfrucht”.
This terminology makes the individual lending the species his name unusually prominent. Thus, it might be interesting how this terminology developed and how the plant, which is now an important research object, found its way into the Western botanical classification system.[39]
CHEMICAL CONSTITUENTS –
Sesquiterpenes can be divided into nitrogen?containing (sesquiterpene alkaloids) and nitrogen?free sesquiterpenes(dihydro agar of uran sesquiterpene polyol esters) based on their distinct structural characteristics.
Diterpenes, the major active constituents of TwHF, include abietane?, kaurane?, and pimarane?type diterpenoids. The triterpenes contained in TwHF are mainly divided into the friedelane, oleanane, and ursane types of chemical constituents, which prominently exhibit anti?inflammatory, anticancer, antiviral, antifibrotic, immunosuppressive, metabolic dysfunction regulation, and spermicidal activities.[40]
Alkaloids can be divided into sesquiterpene alkaloids (the main active alkaloids in TwHF) and spermidine alkaloids, and both of these types exhibit strong pharmacological activities such as anti?inflammatory, antiviral, immunosuppressive, and insecticidal activities. Two unusual prenylated and C?methylated flavanones, namely (±)?5,4??dihydroxy?2??methoxy?6?,6"?dimethypyrano?(2",3":7,8)?6?methyflavanone and (2S)?5,7,4??trihydroxy?2??methoxy?8,5??di(3?methyl?2?butenyl)?6?methyflavanone, were isolated and identified from the stems and roots of TwHF. [41]
Three esterifying lignans isolated from the leaves of TwHF, namely, (+)?(8R,7?S,8?R)?9?acetoxy?9??benzoyloxy?isolariciresinol, (+)?(7R,8S,8?S)?9?benzoyloxy?lariciresinol, and (+)?(7R,8S,8?S)?9?benzoyloxy?5?methoxy?lariciresinol, exert moderate inhibitory effects on NO production in LPS?induced macrophages.
Several organic acids, including 3?oxo?olean?9,3?acetoxy oleanolic acid, tricosanoic acid, stearic acid, and palmitic acid, were isolated and identified from the root bark of TwHF, and some of these compounds can exhibit obvious anti?inflammatory and anticancer activities. Anthraquinones, coumarin, and other constituents have also been isolated from TwHF.[42]
THERAPEUTIC EFFECT –
TwHF is used to be a novel immunosuppressive and anti- inflammatory agent, especially for rheumatoid arthritis (RA), nephrotic syndrome, diabetic nephropathy, and kidney transplantation. It has also been reported as an antitumor agent. In addition, reports discussed the role of TwHF in the treatment of HIV/AIDS (73) and male fertility regulation.
Anti?inflammatory effects
During the development of RA, many immune cells, such as T and B cells, gather at the inflamed joints, promote the production of pro?inflammatory factors and induce fibroblast synovitis cell proliferation, and these effects lead to synovitis, which is one of the primary pathological manifestations of RA.
Tao et al. revealed that alcohol/ chloroform and ethyl acetate extracts of TwHF suppress the upregulation of Cox?2 and thereby inhibit the production of PGE?2 in fibroblasts.
Celastrol can reduce the inflammatory response of synovial fibroblasts by activating the calcium signaling pathway and can inhibit cellular proliferation by inducing DNA damage, cell cycle arrest, and apoptosis in vitro.
In addition, both celastrol and TP inhibit synovial fibroblast migration and invasion by suppressing NF?κB?mediated matrix metalloproteinase 9 (MMP?9) expression and blocking the activation of the JNK–MAPK pathway.[43]

Fig. 16
Cartilage and bone protective effects
As an important component of synovial joints, cartilage can be significantly damaged with the hyperplastic synovial membrane during RA progression due to cell directional invasion.
The role of TwHF?based therapy as a modulator of cartilage and bone destruction has drawn some attention in recent years, and the available evidence shows effects on receptor activator of nuclear factor?κB (RANK)/RANK ligand (RANKL)/OPG (osteoprotegerin) signaling, which affects the balance between osteoclasts and osteoblasts and regulates bone metabolism.
In particular, our data show that TP can exert chondroprotective effects in IL?1?treated synovial fibroblasts via directly suppressing proMMPs 1 and 3 production and simultaneously upregulating the tissue inhibitor of metalloproteinase (TIMPs), and in CIA rats model by interfering with MMP 3 and MMP 13 expression, and augmenting TIMP 1 and 2 expression.[44]
In addition, it can inhibit RANKL expression and upregulate the expression of OPG. Accordingly, celastrol and (5R)?5?hydroxy TP (LLDT?8) also reportedly alleviate joint inflammation by regulating RANKL/RANK/OPG signaling.
Outside of RANK/RANKL/OPG signaling, Li et al. found that TP could enhance the suppressive effect of Tregs on osteoclast differentiation and bone resorption by increasing IL?10 and TGF?β1 secretion and induce MC3T3?E1 cell cycle arrest and apoptosis, which indicates that the bone protective effect of TP might be related to its immunomodulatory functions.[45]
Achyranthes L. (Amaranthaceae), also known as Chaff Flower and Niuxi mainly includes two famous medicinal species namely A. bidentata and A. aspera. A.bidentata has been widely used as blood-activating and stasis-resolving medicine for the treatment of various diseases including amenorrhea, dysmenorrhea, lumbago, gonalgia, paraplegia, edema, stranguria, headache, dizziness, odontalgia, oral ulcer, hematemesis, and epistaxis.

Fig. 17
A.aspera has been widely used to treat various diseases, including gynecological disorder, asthma, ophthalmia, odontalgia, haemorrhoids, and abdominal tumor, and has been applied to difficult labour, wound healing, insect and snake bites.
Among the 21 species, Achyranthes bidentata and Achyranthes aspera are the two most mainly used medicinal plants. Achyranthes bidentata is widely used in China, India, Korea, Java, Japan, and other districts.
Achyranthes aspera is widely distributed in China, India, South Korea, Bangladesh, Pakistan, Sri Lanka, Philippines, and Kenya. The root of A.bidentata and A. aspera is one of the most commonly used medicinal parts [46]. In clinical application, it was used for amenorrhea, dysmenorrhea, waist and knee pain, muscle and bone weakness, stranguria, edema, headache, and vertigo.
Chemical constituents
In recent years, phytochemical research revealed that more than 270 metabolites have been isolated from A. bidentata including terpenoids, steroids, alkaloids, flavonoids, organic acids, alkanes, phenylpropanoids, volatile oils, and others.
In addition, modern pharmacological studies have revealed that A. bidentata exerted alleviating osteoarthritis effect, anti-osteoporosis activity, neuroprotective effect, antidiabetic activity and associated complications, immunoregulatory activity, anti-inflammatory effect, anti-tumor activity, hepatoprotective effect, protection of intervertebral disc, protecting cardiomyocytes, antioxidant effect, anti-acute gout effect, antiatherogenic effect, antibacterial effect, eosinophilic asthma and anti-obesity effect and other effect.
So far, a lot of studies on metabolites and pharmacological activity of A. bidentata have been done, and research on the toxicology of A. bidentata is limited until now. Unfortunately, there is no comprehensive and systematic review about botany, traditional uses, phytochemistry, pharmacology, and toxicology of A. bidentata. To further explore the medicinal value of A. bidentata, we comprehensively and systematically reviewed the botany, traditional uses, phytochemistry, pharmacology, and toxicology, which provides a reference for an in-depth investigation of A. bidentata.[47]
Pharmacological activities of A. bidentata
The different extracts and metabolites of A. bidentate exhibited a broad spectrum of pharmacological effects, including alleviating osteoarthritis (OA) effect, anti osteoporosis activity, neuroprotective effect, antidiabetic activity, immunoregulatory activity, anti- inflammatory effect, anti-tumor activity, hepatoprotective effect, protection of intervertebral disc, protecting cardiomyocytes, antioxidant effect, alleviating stroke, antiatherogenic effect, antibacterial effect and associated complications, and so on.

Fig. 19
Anti Osteoporosis activity
A lot of different crude extracts of A. bidentata showed significant anti osteoporosis activity. In 2000, Xiao et al. found that the mixture extract of petroleum ether and ethyl acetate of A. bidentata had a strong effect on promoting the proliferation of osteoblast cells UMR106 using an MTT method.[48]
The mixture extracted by petroleum ether and ethyl acetate promoted cell proliferation significantly during the dosage of 0.0001 mg/ml to 0.000001 mg/ml.
Among them, the proliferation rate was the highest when the order of magnitude was 0.000001mg/ml, and the average growth rate was 55%.
In 2011, Yang et al. [49] indicated that 95% ethanol extract isolated from A. bidentata exhibited anti osteoporosis activity in ovariectomized (OVX) rats. After the treatment of 95% ethanol extract isolated from A. bidentata, bone mineral density (BMD) and type I collagen in OVX rats were up-regulated significantly at 160 and 320 mg/kg, and the bone turnover rate was improved in a dose-dependent manner. In the other investigation, different extracts of roots of A. bidentata exhibited the inhibitory effect of bone resorption induced by parathyroid hormone (PTH) in a bone organ culture using neonatal mouse parietal bones.
Astragalus membranaceus (Fisch.) Bunge, also known as “Astragali radix” or “Huangqi”, is the source of one of the most well-known Chinese medicinal herbs, produced from its dry root.

Fig. 20
Huangqi, translated as “yellow leader” in Chinese, refers to the yellow color of the roots as well as its leading status as one of the most important tonic herbs in traditional Chinese medicine [50].
Astragalus membranaceus as one of the most important Qi tonifying adaptogenic herbs in traditional Chinese medicine has a long history of medicinal use. In traditional Chinese medicine, which laid a lot of emphasis on Qi (vital energy) and Yin-Yang balance (negative and positive equilibrium). Chinese herbs have been used as traditional medicine immune booster for human beings for thousands of years in China and many parts of Asia. The goal of this review is a survey on some important ancient and modern pharmaceutical sciences of astragalus.[51]
CHEMICAL CONSTITUENTS
The main reported chemical constituents of A. membranaceus were triterpenes, polysaccharides, flavonoids, and saponins. The presence of compounds such as terpenoids and flavonoids that usually occur in free or glycosidic form is of relevant pharmacological interest due to the bioactivities attributed to these classes of compounds.
The flavonoids include flavonols, flavones, flavanones, and isoflavonoids which have been described as having many types of bioactivities.
Compounds extracted with 75% methanol from different parts of Astragalus (roots, stems, leaves, petioles, and flowers) were analyzed by UPLC-MS/MS
technique, to evaluate flavonoids and triterpenoids distribution, together with 13 of their metabolites, showing that isoliquiritigenin, liquiritigenin, daidzein, and bioactive isoflavones accumulate in both roots and flowers.
The content in the isoflavones, calycosin, and calycosin-7-O-β-d- glucoside, was found to be the highest in the leaves and roots of A. membranaceus, as revealed by HPLC analysis.

Fig. 21
With calycosin content in leaf (145.56 μg/g DW) higher than in root (1.64 μg/g DW), while calycosin-7-O-β-d-glucoside content in root (4.88 μg/g DW) higher than leaf in (2.0 μg/g DW)[52]. Kwon et al. (2013) analyzed the content in Astragalosides, known as the highly bioactive compound in A. membranaceus root, and reported that Astragalosides are more concentrated in periderm and cortex than in xylem; and that unpeeled roots were richer in these compounds isolated 24 secondary metabolites (isoflavonoids, astragalosides, and benzoquinone) from A. membranaceus roots, and the (–)-methylinissolin 3-O-β-d-glucoside was detected for the first time in this study, and shown to possess potent anti-inflammatory activity, evaluated by the inhibition of nitric oxide (NO) released by lipopolysaccharide (LPS)- stimulated macrophages (RAW 264.7 cells). Ethanolic extract of Astragali Radix, analyzed by RP-HPLC, main content included triterpene saponins, namely astragaloside I–IV, isoflavonoids (formononetin and calycosin) which are the main bioactive compounds.[53]
Pharmacological effects
In traditional Chinese medicine, A. membranaceus has been used for the treatment of general weakness and chronic illness and to increase overall vitality. Different peripheral effects such as improved sensitivity to insulin, immune modulation, antiviral activity, antitumor activity, and enhancement of cardiovascular functions have been described. The protection of cardiovascular function might be explained in terms of protection against membrane lipid peroxidation.[54]
Anti-inflammatory activity
Polyphenolic compounds from various herbs have been found to exhibit anti-inflammatory activities. HPLC analysis of AR showed the presence of several secondary metabolites including polyphenolic flavonoids, such as formononetin, which have various biological effects on cell signaling, cell division and growth, and gene expression,and are presumed to partially contribute to the anti-inflammatory effects of AR.

Fig. 22
Reported that AR displays anti-inflammatory effects in zymosan air-pouch mice by reducing the expression of iNOS, cyclooxygenase-2 (COX-2), IL-6, IL-1β, and tumor necrosis factor-α (TNF-α) as well as by limiting the production of nitric oxide.
In a similar manner, AR reduces the expression of IL-6, iNOS, and COX-2 in lipopolysaccharide (LPS)-treated Raw 264.7 cells. They further demonstrate that AR attenuates the activity of p38 and extracellular signal-regulated kinases 1 and 2 and stimulates mitogen- activated protein kinase phosphatase-1 (MKP-1) in LPS-treated Raw 264.7 cells.
In addition, AR interferes with the translocation of NF-kB to the nucleus,subsequently resulting in NF-kB-dependent transcriptional repression.
Taken together, these data reveal that AR has an antiinflammatory effect mediated by the MKP-1-dependent inactivation of p38 and the inhibition of NF-kB-mediated transcription. These reports support the traditional use of AR and suggest that it is a safe and mild antiinflammatory agent for treating various inflammatory disorders.[55]
Effects on blood pressure
Astragalus has a biphasic regulation of the blood pressure. It can increase the total body protein and albumin level, reduce the urinary protein, and increase the cardiac stroke volume and dilation of the blood vessels to lower or raise the blood pressure. Research has shown that acute intraperitoneal injection of Astragalus to all rats, observed at different times, exhibited no acute antihypertensive effect. Intraperitoneal injection of an aqueous extract of Astragalus to rats exhibited no acute hypertensive effect. In addition, repeated injections, over a long term, significantly inhibited blood pressure elevation in spontaneously hypertensive rats (SHR), eventually causing a gradual decline, without induced blood pressure increase in SHR other than the increase prior to the start of the experiment. Astragalus had no obvious effect on normal rat blood pressure, The control of blood pressure related to the Astragalus dose showed that the higher the administration dosage, the more obvious the decline in the SHR blood pressure [56].
Conclusion
Astragalus membranaceus, a fundamental herb in traditional Chinese medicine, has demonstrated a wide range of pharmacological benefits supported by both ancient practices and modern scientific research. Its rich content of bioactive compounds such as polysaccharides, flavonoids, and saponins contribute to its immunomodulatory, antioxidant, anti-inflammatory, antihyperglycemic, antiviral, and cardioprotective activities. These effects not only validate its traditional use but also highlight its potential in the prevention and treatment of various chronic diseases, including diabetes, cardiovascular disorders, and immune dysfunctions. Continued exploration and integration of A. membranaceus into modern medicine could offer safer, natural therapeutic alternatives, reinforcing the bridge between traditional knowledge and contemporary healthcare.
Ligusticum chuanxiong Hort., Family Umbelliferae, is a well-known traditional medicinal herb and mainly distributed in Sichuan Province of China. L. chuanxiong is first recorded in the Shen Nong Ben Cao Jing, the rhizome of which is warm in property and pungent in flavor, with functions of promoting the circulation of the blood and qi,expelling wind, and alleviating pain.

Fig. 23
Therefore, L. chuanxiong has long been used as a traditional Chinese medicine for the treatment of headache, rheumatic arthralgia, menstrual disorders, swelling pain due to traumatic injury and coronary heart diseases.
Usually it is added to a soup, such as Chuanxiong mutton soup and Chuanxiong fish’s head soup. Major chemical components of L. chuanxiong are essential oils, alkaloids, phenolic polysaccharides and proteins (Zhang et al., 2003). [57]
Ligusticum chuanxiong Hort (LC), family Umbelliferae, is also called Ligusticum wallichii Franchat. It is mainly distributed in Sichuan province (China) and first recorded in the Divine Husbandman’s Classic of the Materia Medica (Shen Nong Ben Cao Jing).
Chemical constituents
Ligusticum chuanxiong Hort., commonly referred to as Chuanxiong Rhizoma, is a well- known traditional Chinese medicinal herb used primarily to promote blood circulation, relieve pain, and treat cardiovascular and neurological disorders. Its therapeutic effects are largely attributed to its diverse chemical constituents, which include phthalides, alkaloids, essential oils, phenolic acids, and polysaccharides.
Among these, phthalides are the most characteristic and bioactive group, with Z-ligustilide, butylidenephthalide, and senkyunolides (A, H, I) being predominant. These compounds possess significant pharmacological properties such as vasodilation, anti-inflammatory, neuroprotective, and anti-platelet aggregation effects (Zhou et al., 2016; Xiong et al., 2011).
Another key component is the alkaloid tetramethylpyrazine (ligustrazine), which has been widely studied for its potent neuroprotective, antiplatelet, and anti-hypoxic effects, and is often used as a chemical marker for quality control in herbal formulations (Li et al., 2012; Chinese Pharmacopoeia Commission, 2020).

Fig. 24
In addition, L. chuanxiong contains a range of volatile essential oils, including myristicin, α- pinene, and sabinene, which contribute to its fragrance and exhibit antimicrobial and antioxidant activities (Zhou et al., 2016). Phenolic compounds, such as ferulic acid, caffeic acid, chlorogenic acid, and vanillic acid, are also abundant and are known for their free radical scavenging, anti-inflammatory, and cardioprotective properties (Xiong et al., 2011; Li et al., 2012). Furthermore, bioactive polysaccharides present in the rhizome have shown immunomodulatory and antioxidant potential, enhancing the plant’s therapeutic profile (Zhou et al., 2016).[58]
Pharmacological effects
Ligusticum chuanxiong exhibits a variety of pharmacological effects due to its active constituents such as phthalides, alkaloids, essential oils, phenolic acids, and polysaccharides. Phthalides like Z-ligustilide and senkyunolide A show vasodilatory, anti- inflammatory, neuroprotective, and antiplatelet effects, making them effective in treating cardiovascular and neurological disorders (Zhou et al., 2016; Xiong et al., 2011).
The alkaloid tetramethylpyrazine (ligustrazine) improves blood circulation, protects against hypoxia, and exhibits strong neuroprotective and antithrombotic activity, commonly used in managing stroke and heart diseases (Li et al., 2012). Essential oils like myristicin and α-pinene provide antioxidant and antimicrobial benefits, while phenolic compounds such as ferulic and caffeic acids contribute to free radical scavenging and anti- inflammatory actions.
Additionally, polysaccharides show immunomodulatory and antioxidant properties, supporting the herb’s traditional use in chronic disease management (Chinese Pharmacopoeia Commission, 2020; Zhou et al., 2016).[59]
Anti-inflammatory Activity of Ligusticum chuanxiong
Ligusticum chuanxiong demonstrates significant anti-inflammatory properties, primarily due to its active constituents such as Z-ligustilide, senkyunolides, ferulic acid, and tetramethylpyrazine (ligustrazine). These compounds inhibit the production of pro- inflammatory cytokines like tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and interleukin-1β (IL-1β). Z-ligustilide has been shown to suppress nuclear factor-kappa B (NF-κB) activation, a key pathway involved in inflammation.
Ferulic acid and caffeic acid also scavenge reactive oxygen species (ROS), thereby reducing oxidative stress-induced inflammation. Moreover, ligustrazine reduces inflammatory damage by inhibiting cyclooxygenase-2 (COX-2) expression and improving microcirculation in inflamed tissues.
These mechanisms make L. chuanxiong effective in managing inflammatory conditions such as arthritis, cardiovascular inflammation, and neuroinflammation (Zhou et al., 2016; Xiong et al., 2011; Li et al., 2012).[60]
Conclusion
Ligusticum chuanxiong is a valuable traditional medicinal herb with a wide range of pharmacological effects, primarily attributed to its rich content of phthalides, alkaloids, essential oils, phenolic acids, and polysaccharides. Among its various therapeutic properties, its anti-inflammatory activity stands out, mediated by the suppression of pro-inflammatory cytokines, oxidative stress, and key inflammatory pathways such as NF-κB and COX-2. These bioactivities support its traditional use in treating conditions involving inflammation, cardiovascular dysfunction, and neurological disorders. The scientific validation of its effects further highlights its potential as a complementary agent in modern medicine for managing inflammatory and circulatory diseases.
Aconitum kusnezoffii Reichb., commonly known as Kusnezoff’s aconite, is a perennial herb from the Ranunculaceae family that is traditionally used in East Asian medicine, particularly in China, Korea, and Russia. The processed root, referred to in Traditional Chinese Medicine (TCM) as "Zhi Fu Zi," is used to treat cold-related conditions such as arthritis, joint pain, heart failure, and yang deficiency syndromes.
It functions by warming the body, alleviating pain, and stimulating circulation (Zhou et al., 2015). The pharmacological actions of A. kusnezoffii are mainly attributed to its potent alkaloids, including aconitine, mesaconitine, and hypaconitine, which exert significant effects on the nervou cardiovascular systems (Li et al., 2011).
These compounds can be highly toxic if not properly processed, leading to severe adverse effects such as arrhythmias, numbness, and cardiac arrest (Chan, 2009).
Traditional detoxification methods—such as boiling, soaking, or steaming—are essential to reduce toxicity and ensure safe use (Tai et al., 1992). Despite its toxicity, when used with caution and expertise, A. kusnezoffii demonstrates remarkable therapeutic value in managing chronic inflammatory disorders like rheumatism and neuropathic pain (Chinese Pharmacopoeia Commission, 2020).[61]
Chemical Constituents
The primary bioactive components of Aconitum kusnezoffii Reichb. are diterpenoid alkaloids, which are largely responsible for its potent pharmacological effects as well as its well-documented toxicity.

Fig. 26
Among these, the most significant are aconitine, mesaconitine, and hypaconitine, which belong to the class of C19-diterpenoid alkaloids. These alkaloids act primarily on voltage-gated sodium channels, leading to increased sodium influx, which contributes to their analgesic and anti-inflammatory effects but also poses a risk of severe cardiotoxicity and neurotoxicity if not properly processed (Li et al., 2011; Zhou et al., 2015). Other identified constituents include jesaconitine, benzoylaconine, and lappaconitine, the latter being relatively less toxic and used in some clinical settings in China as an analgesic (Chan, 2009). These compounds vary in concentration depending on the plant’s origin, age, and processing method. Traditional detoxification processes, such as boiling or soaking, are essential to hydrolyze the ester bonds in aconitine-type alkaloids, converting them into less toxic derivatives like benzoylaconine and aconine (Zhou et al., 2015). The complexity and potency of these chemical constituents make A. kusnezoffii a pharmacologically valuable but dangerous plant, requiring expert handling in both traditional and modern medicinal practices.[62]
Anti-Arthritis and Anti-Inflammatory Actions of Aconitum kusnezoffii Reichb. (Kusnezoff’s Aconite)
Aconitum kusnezoffii Reichb. has long been used in traditional Chinese medicine for its potent analgesic and anti-rheumatic effects, particularly in the treatment of arthritis and inflammatory joint conditions. The primary mechanism behind its anti-arthritic action lies in the activity of C19-diterpenoid alkaloids such as aconitine, mesaconitine, and hypaconitine, which act on the central and peripheral nervous systems to relieve pain and stiffness associated with rheumatoid and osteoarthritis. These compounds are believed to modulate voltage-gated sodium channels, leading to reduced excitability of pain-conducting neurons and thus alleviating the symptoms of joint inflammation and pain.
In addition to its analgesic properties, A. kusnezoffii exhibits anti-inflammatory activity by downregulating pro-inflammatory cytokines such as TNF-α, IL-1β, and IL-6, which are commonly elevated in inflammatory diseases like arthritis (Zhou et al., 2015). These alkaloids inhibit COX-2 and NF-κB pathways—two major signaling cascades involved in the inflammatory response. Furthermore, processed extracts of A. kusnezoffii have been shown to reduce edema in animal models and decrease the expression of inflammatory mediators in synovial tissue, contributing to joint protection and improved mobility.
However, due to the plant’s narrow therapeutic index and potential for severe toxicity, especially cardiotoxicity and neurotoxicity, modern applications require careful detoxification and strict dosage control. Traditional processing methods, such as boiling or steaming, hydrolyze toxic diester alkaloids into safer monoester forms, which retain therapeutic efficacy while minimizing toxicity (Chan, 2009).
These findings support the traditional use of Aconitum kusnezoffii in anti-arthritic formulations and point to its potential as a natural alternative for managing chronic inflammatory conditions, provided that safety concerns are adequately addressed.[63]
Formulation and Incorporation of Herbal Drug for Arthritis into a Transdermal Patch
The formulation of a transdermal patch incorporating a herbal drug for arthritis involves a series of carefully designed steps, beginning with the selection and extraction of the herbal component. In this study, Curcuma longa (turmeric), known for its potent anti-inflammatory and antioxidant properties, is chosen due to its active constituent curcumin, which has been extensively studied for its efficacy in managing arthritis-related symptoms. The turmeric rhizomes are first cleaned, dried, and powdered.
Extraction of curcumin is carried out using a Soxhlet apparatus with ethanol as the solvent for approximately 6–8 hours. The resulting extract is filtered and concentrated using a rotary evaporator, then dried and stored in an amber-colored bottle to protect it from light and degradation.[64]

Fig. 27
For the preparation of the transdermal patch, the solvent casting method is employed, which is widely recognized for its simplicity and suitability for incorporating both hydrophilic and lipophilic drugs. A polymeric solution is prepared using Hydroxypropyl Methylcellulose (HPMC), which serves as the film-forming polymer, dissolved in a hydroalcoholic solvent system consisting of ethanol and distilled water in a 1:1 ratio.
The solution is stirred continuously and allowed to stand overnight to ensure complete hydration of the polymer. To this hydrated polymer solution, a measured amount of curcumin extract is added, ensuring uniform dispersion by continuous stirring. A plasticizer, such as Polyethylene Glycol 400 (PEG-400), is then incorporated to enhance the flexibility and mechanical strength of the patch. Additionally, a permeation enhancer like eucalyptus oil may be added to facilitate the passage of curcumin through the stratum corneum of the skin, thereby improving transdermal absorption.[65]
The resulting homogeneous mixture is poured onto a leveled glass plate or Petri dish, ensuring a uniform thickness of the film. It is then allowed to dry at room temperature or in a hot air oven at a controlled temperature of around 40–45°C. Once dried, the film is carefully peeled off and cut into patches of the desired size, typically 2×2 cm², each containing a fixed amount of the active herbal extract. These patches are then subjected to a series of physicochemical evaluations including thickness measurement, weight variation, folding endurance, surface pH, drug content uniformity, moisture content, and in vitro drug release studies using a Franz diffusion cell. Such evaluations ensure the quality, consistency, and therapeutic potential of the formulated patch.
The patches are stored in airtight containers or aluminum foil pouches to protect them from environmental factors such as moisture and light.
This method not only enables the sustained release of curcumin over an extended period but also avoids the gastrointestinal side effects commonly associated with oral anti-inflammatory medications. Thus, the development of a transdermal patch incorporating a herbal anti-arthritic drug like curcumin represents a promising approach for the effective and patient-friendly management of arthritis.[66]
FUTURE PROSPECTS
While the study establishes a strong foundation for the use of herbal transdermal patches in arthritis management, there is significant scope for further research and development. Future studies should focus on in vivo pharmacokinetic and pharmacodynamic evaluations to better understand the systemic absorption and therapeutic efficiency of the patches. Clinical trials are essential to validate the efficacy and safety of these herbal patches in human subjects and to explore any long-term effects or allergic reactions. Advancements in nanotechnology and bioadhesive polymers can further enhance skin permeation and therapeutic efficacy. Incorporating techniques such as microneedle-assisted delivery, nanostructured lipid carriers (NLCs), and ethosomal or transfersomal systems could significantly improve drug permeation and control release rates. Additionally, combination therapy with other plant extracts like Boswellia serrata, Aloe vera, or Withania somnifera could be investigated for synergistic effects.
Further, the development of smart patches integrated with sensors for monitoring therapeutic response and patient compliance could represent the next generation of herbal drug delivery systems. Overall, herbal transdermal patches present a promising, patient-friendly, and effective alternative for long-term management of arthritis, aligning with the global shift toward natural and sustainable healthcare solutions.
CONCLUSION
The present study successfully demonstrates the potential of transdermal patches as an effective delivery system for herbal anti-arthritic drugs. Utilizing Curcuma longa (turmeric) as the primary herbal agent, known for its active compound curcumin, the study highlights its potent anti-inflammatory, antioxidant, and immunomodulatory properties that make it an ideal candidate for managing rheumatoid arthritis. The solvent casting method employed for formulation was found to be efficient in producing stable and uniform patches with desirable mechanical and physicochemical characteristics. Evaluations including thickness, weight variation, drug content uniformity, folding endurance, surface pH, and in vitro release studies confirmed the quality and performance of the developed transdermal system.
By bypassing hepatic first-pass metabolism and gastrointestinal degradation, the transdermal route offers a promising alternative to conventional oral therapies, minimizing side effects and improving patient compliance. The use of biocompatible polymers like HPMC, along with plasticizers and permeation enhancers, facilitated the controlled and sustained release of the herbal extract, ensuring prolonged therapeutic action at the site of inflammation. The findings indicate that herbal-based transdermal systems can effectively deliver therapeutic agents for chronic inflammatory conditions such as arthritis.
REFERENCES



Krishnendu Ghosh, Debayan Bag, Soumyajit Roy, Formulation, Evaluation and Validation of Herbal Anti Arthritic Transdermal Patches: A Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 3014-3046. https://doi.org/10.5281/zenodo.17989377
 10.5281/zenodo.17989377
10.5281/zenodo.17989377