1,5 Rungta Institute of Pharmaceutical Sciences, Bhilai
2,3,4 Rungta Institute of Pharmaceutical Sciences and Research, Bhilai
Psoriasis is a skin disease which is characterized by inflammation that has immunity-mediated origin. The long term use of standard topical drugs is often associated with undesired effects. Thus there exists a need for safer and more tolerable alternatives1. Studies show that Allicin, the main bioactive component of garlic (Allium sativum) can be an effective treatment for Psoriasis. Allicin has strong anti-inflammatory, antibacterial, antioxidant and immunomodulatory properties2. The aim of the present study is to formulate and evaluate a topical gel of allicin with the help of an appropriate gelling agent to possess an ideal consistency, stability and therapeutic efficacy2. The gel subjected to evaluation for preliminary physiochemical parameters which includes pH, homogeneity, viscosity, spreadability, extrudability, in-vitro drug diffusion, skin irritation and stability1 and was found to be satisfactory. The gel formulation was found to have very good physicochemical characters, stability and controlled release of allicin1. According to the results, the allicin gel formulation can be safely used for the topical treatment of psoriasis. It is effective in terms of an alternate treatment option. Further studies are needed on medicinal efficacy3.
One form of psoriasis isn’t the same in everyone, showing different types because of varied genetic roots. Because of genes, some people are more likely to develop certain symptoms than others. This skin issue stands apart from most long-term inflammations by its strong tie to HLA-C1. Most individuals with it carry the HLA-Cw0602 version - about twice as many as those without the condition. While inflammation plays out across body defenses, both immediate and learned responses get involved. Even healthy skin cells react when exposed to similar triggers found in affected areas. Skin trouble called psoriasis turns on immune responses normally quiet in healthy people. From deep within, dendritic cells plus T-helper types - especially Th1 and Th17 - get too active, releasing large amounts of signaling proteins such as TNF-α, IL-17, and IL-23. This flood keeps swelling going, while speeding up how fast skin forms layers2. Some folks carry gene markers, like HLA-Cw6, making them more likely to develop it. Outside factors matter just as much: infections, injured skin, pressure on mind or body, even some drugs can spark first signs or worsen current symptoms3. Newer findings point toward tiny life forms living on or inside us playing a role in starting flare-ups. Microbes including Streptococcus pyogenes, Staphylococcus aureus, along with fungi named Malassezia, show ties to sudden outbreaks or worsening patches - especially on scalp or in droplet-shaped rashes known as guttate form. Out of nowhere, psoriasis can show up - young kids get it, older adults too4. Most often though, it starts showing during the late teens or by the mid-thirties. Alongside skin changes, some people face related health issues like stiff joints, heart troubles, or shifts in metabolism5.
1.1 Types of Psoriasis:
Psoriasis is mainly of seven Types:
1. Plaque Psoriasis:
Plaque Psoriasis is the most common kind of psoriasis, affecting around 80-90% of the population. This is distinguished by the growth of inflamed, red areas coated in silvery-white scales. They usually occur in specific locations, such as the scalp, elbow, knees, or back. Sometimes they might cause burning and irritation4.
2. Inverse Psoriasis:
Psoriasis typically grows in skin folds such as armpits, groins, beneath breasts, and genitals. It can produce thin plaque, but without the scales, it is smooth, glossy, and red. And develop via frictions and sweats5.
3. Guttate Psoriasis:
Guttate Psoriasis usually occurs when a streptococcus causes a sore throat. It shows as little drop-shaped lesions on the trunk, arms, legs, and scalp. They are particularly frequent among children and young adults. These psoriatic lesions are smaller than plaque Psoriasis5.
4. Pustular Psoriasis:
Pustular Psoriasis is characterized by small, pus-filled bumps on top of non-infectious, sterile plaques. They mainly affect the hands and feet. They are the most severe kind and can cause the flu, fever, chills, dehydration, and a fast pulse6.
5. Erythrodermic Psoriasis:
Erythrodermic Psoriasis is a severe and rare form of psoriasis that involves around 90% of the skin's surface. This might lead to skin discolouration and shedding.4. This can lead to extreme itching, discomfort, and skin peeling. Psoriasis can sometimes be life-threatening owing to significant loss of fluids and proteins.6
6. Sebo Psoriasis:
Sebo Psoriasis is a chronic skin disorder that has characteristics of seborrheic dermatitis (greasy, yellowish scales) and psoriasis (thick, red, well-defined plaques). It mostly affects oily regions such as the scalp, face, behind the ears, and skin folds. Treatment often consists of medicinal shampoos, topical corticosteroids, or antifungals, with flare-ups treated by treating both inflammation and scaling7.
7. Nail Psoriasis:
Nail psoriasis (psoriatic onychodystrophy) is a chronic inflammatory disorder that causes structural destruction to the fingernails and toenails. It affects 10-80% of psoriasis patients, especially those with psoriatic arthritis. Pitting, discoloration (yellow/red), crumbling, and nail bed separation (onycholysis) are common signs that cause discomfort and functional impairment5.
2. HISTORY:
Psoriasis is the oldest skin illness documented in history. Medical literature from antiquity, including manuscripts that were given to Hippocrates, shows an account of the disease by which the skin becomes scaly. Before the 19th century, psoriasis was incorrectly diagnosed leprosy and other chronic skin diseases. According to our current understanding, psoriasis is a chronic disease that is immunologically mediated by inherited susceptibility and environmental factors that generate abnormal keratinocyte proliferation and systemic inflammation8. Psoriasis is a common public health problem affecting people the world over. Data from Global Burden of Disease (GBD) indicate that between 40-65 million people with psoriasis exist globally, and the age standardized prevalence estimation is between 0.5 to 1% of entire population7. Other epidemiological sources provide prevalence estimates for adults ranging between 0.15 and 3.68% depending on the geographical area, with lower frequencies observed in Asia and Sub-Saharan Africa and higher in Europe and North America7. The disorder may manifest at any age but is generally most likely to occur in younger adulthood or later middle age, with peak prevalence at 40–60 years8.
3. ETIOLOGY:
Skin trouble called psoriasis sticks around long-term, sparked by genes, immunity glitches, alongside outside influences. Studies scanning entire genomes point to markers like HLA-Cw6, making some react oddly in immune terms. When the IL-23/Th17 pathway runs off track, chemicals - IL-17, IL-22, TNF-α - spill out too much, pushing skin cells to grow fast while maturing poorly. Infections from strep bacteria, cuts, life strain, tobacco use, drugs such as β-blockers or lithium - these nudge flare-ups among those already set up by DNA. Quick skin renewal, new blood vessels forming, ongoing swelling - all shape red, flaky patches typical of this condition1.
4. DIAGNOSTIC APPROCHES OF PSORIASIS:
Psoriasis diagnostics are mostly Spotting often begins by looking closely at the skin. Well-marked red patches covered in shiny silver flakes show up most on elbows, knees, the lower back, or scalp. These signs help doctors tell it apart from other rashes10. Under magnification, tiny dot-like blood vessels stand out amid pale scale layers. Checking tissue under a microscope adds clarity when appearance alone isn’t enough. Blood work or scans step in only if confusion remains11. To measure how widespread it is, tools like PASI and BSA assign values based on coverage and thickness. Each person's pattern guides how numbers are interpreted. Scoring helps track change over time rather than label stages. Pictures from scans - like X-rays, ultrasounds, or MRIs - help spot swelling in joints or harm to tissue when doctors think someone might have psoriatic arthritis. Blood tests? They usually check what it’s not, sorting through other possible conditions while also looking at health issues that show up alongside it, instead of proving psoriasis itself12.
5. TREATMENT APPROCHES OF PSORIASIS:
5.1 Introduction of Allicin:
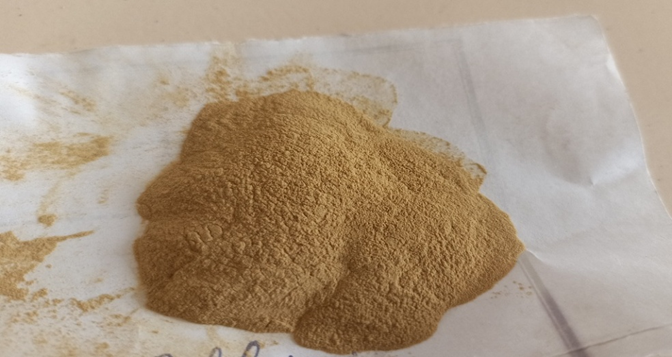
When garlic cloves are crushed, a sulfur-containing compound called allicin forms through an enzymatic reaction involving alliin and alliinase. This substance shows clear anti-inflammatory, antimicrobial, and antioxidant activity, along with influencing immune function. For people with psoriasis, one benefit lies in its ability to slow excessive growth of skin cells while reducing key inflammatory signals like TNF-α, IL-17, and IL-23 - molecules tied to plaque formation1,3,8. Because it limits bacterial presence and counters oxidative damage, both triggers for worsening patches, localized application could help manage flare-ups. Applied directly to affected areas, it supports healing of the outer skin layer and regulates immune behavior, leading to less redness, thinner scales, and reduced lesion size - an option rooted in plant-based chemistry for addressing chronic plaques 10.
What makes allicin notable is how its ability to combat oxidation may lower harm caused by unstable molecules tied to irritated, aging tissue. Yet effectiveness drops fast when exposed to warmth, oxygen, or stomach activity due to inherent fragility and poor uptake in the body. To tackle such issues, researchers look into modern carrier technologies - liposomes, for instance, or transethosomal designs - that protect the compound while boosting penetration through skin layers during treatment of swelling-related conditions1,5,7.
5.2 Materials and Quantity table:
|
Sr. no. |
Material |
Quantity |
Properties |
|
1. |
Allicin |
0.10 g
|
Anti-microbial Anti-Oxidant |
|
2. |
Carbopol 934 |
0.10 g
|
Gelling Agent |
|
3. |
Polyethylene Glycol |
0.50 g
|
spreadability enhancer |
|
4. |
Triethanolamine |
0.5 ml
|
Neutralizing Agent |
|
5. |
Ethanol |
1 ml
|
Penetration enhancer |
|
6. |
Tween 80 |
0.5 ml |
Surfactant |
|
7. |
Rose Water |
2 ml |
Fragrance |
|
8. |
Methyl Paraben |
0.50 g |
preservatives |
|
9. |
Distilled Water |
Quantity sufficient |
Vehicle |
5.3 Material used for allicin based Topical Gel:
1. Allicin: A strong natural substance with antioxidant, antibacterial, and anti-inflammatory properties. beneficial for preventing psoriasis1.
2. Carbopol934: Carbopol 934 is a synthetic polyacrylic acid polymer that is commonly used as a gelling agent in topical preparations. It enhances the viscosity, clarity, and stability of gels and creams. It also improves drug release, spreadability, and bioadhesion, making it excellent for creating dermatological and pharmaceutical topical gels1.
3. Polyethylene Glycol: Polyethylene Glycol (PEG) is a water-soluble polymer often found in pharmaceutical and cosmetic applications. It functions as a solvent, plasticiser, humectant, and penetration enhancer. In topical gels, PEG increases medication solubility, spreadability, and moisture retention4,5.
4. Triethanolamine: Triethanolamine is an organic alkaline chemical that is extensively used in topical medicinal and cosmetic formulations to modify the pH and neutralize it. It neutralizes acidic polymers in gel formulations (e.g., with Carbopol) to produce a clear, stable gel. TEA increases the formulation's consistency, emulsification, and general stability8.
5. Ethanol: Ethanol is a volatile organic solvent commonly included in topical medicinal formulations. It works as a solvent, antimicrobial preservative, and penetration enhancer by disrupting the lipids in the stratum corneum, which improves medication absorption through the skin7.
6. Tween 80: Tween 80, also referred to as polysorbate 80, is a non-ionic surfactant that is frequently utilized in food, cosmetic, and medicinal formulations. It helps combine oil and water by acting as an emulsifier and solubilizing agent. It is frequently utilized in creams, lotions, vaccinations, and oral preparations and increases stability and drug solubility10.
5.4 Preparation of Allicin based Topical Gel:
1. Weighting of Ingredients: Using a calibrated digital balance, accurately weigh all of the essential ingredients: Carbopol 934, polyethylene glycol (PEG), ethanol, sodium cholate, allicin, triethanolamine, and distilled water.
2. Prepare Carbopol Dispersion: In a clean beaker, add the necessary amount of distilled water. Gradually sprinkle Carbopol 934 over the surface of the water while stirring continuously to prevent lump formation. Continue stirring until the Carbopol is completely dispersed and forms a uniform, lump-free solution.
3. Preparation of Solvent Phase: In a separate beaker, add the appropriate amount of polyethylene glycol (PEG). Add ethanol and thoroughly mix to get a homogenous mixture.
4. Addition of surfactant: Dissolve sodium cholate in the PEG-ethanol mixture and stir constantly until a clear solution is formed.
5. Incorporation of Allicin: Add an appropriately weighed amount of allicin to the PEG-ethanol mixture. Because allicin is light and oxidation sensitive, cover the beaker with aluminum foil and limit the amount of time it is exposed to direct light and air.

6. The combination of phases: To achieve a homogenous mixture, slowly add the prepared solvent phase (PEG-ethanol-allicin combination) to the Carbopol dispersion while gently stirring. After all this add methyl Paraben for Preservative and add the rose water for fragrance
8. Neutralization and Gel Formation: Drop triethanolamine (1-2 drops at a time) into the mixture while gently stirring. After each addition, carefully monitor the pH.
9. pH adjustment: Continue to add triethanolamine dropwise until the pH reaches the ideal range of 6.5-8.5, which is appropriate for topical application and guarantees good gel formation.
10. Final gel formation: Stir gently until a clear, smooth, homogenous, and stable allicin gel is formed. Transfer the created gel to an airtight container and keep in a cool, dark location.
6. RESULT:
The viscosity of the Allicin topical gel was evaluated using a Brookfield Viscometer. The obtained viscosity range was within the limits, indicating suitable thickness and consistency. This viscosity guarantees that the gel formulation spreads well on the skin, releases drugs properly, and is stable enough for successful topical treatment.
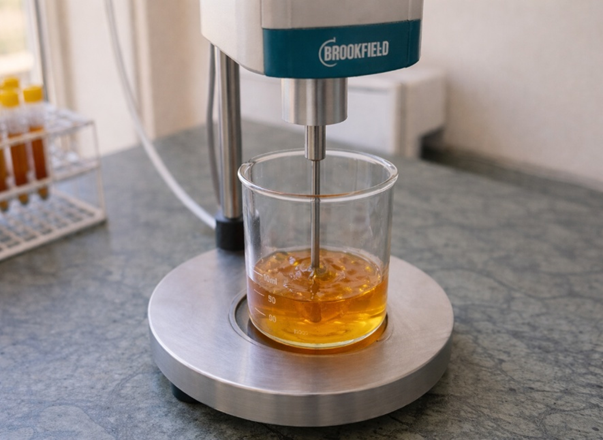
Fig- Viscosity test
The spreadability of the Allicin topical gel was determined using the glass slide technique. The gel spread up to 5.5 cm under the imposed weight. This result shows high spreadability, which allows for simple application to the skin and uniform distribution of the formulation.
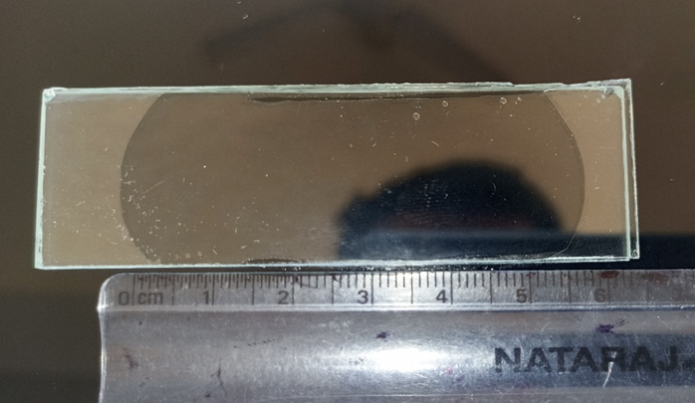
Fig – Spreadability Test
The pH of the Allicin topical gel was tested with a digital pH meter and also with pH paper. The recorded pH value was 7-8, which is near to neutral. This suggests that the formulation is appropriate for topical administration and is unlikely to irritate the skin.
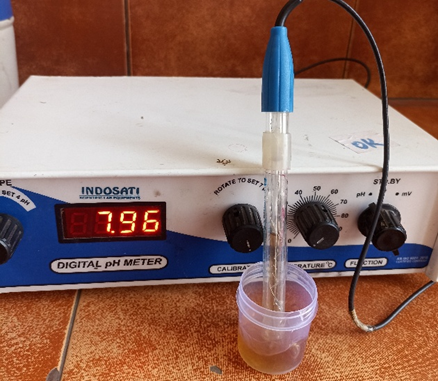
Fig- pH meter
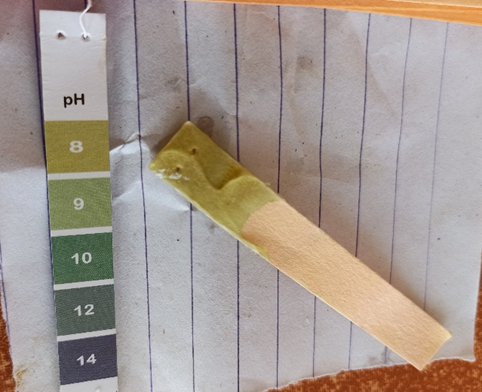
Fig – pH paper
The Allicin topical gel was submitted to stability tests for many weeks. Throughout the trial, no significant changes were noticed in color, odor, pH, viscosity, or spreadability. The results showed that the gel formulation was stable and suited for topical application.
8. DISCUSSION
Despite its simplicity, the testing confirmed the Allicin gel meets key requirements for skin-based treatment. A smooth appearance and feel emerged during assessment - important traits influencing whether users will stick with it. When checked with a standard viscometer, the product held thickness suitable for staying put once placed on the body. Application ease came through clearly: coverage was even, requiring little effort across targeted areas. Although close to neutral pH helps minimize skin reactions, long-term performance stood out more clearly through testing. Over time, key properties stayed consistent - pointing toward thoughtful development behind the product’s makeup.
9. CONCLUSION
A successful outcome emerged through development of an allicin-based gel meant for skin use. Brownish in shade, it carried a mild smell, felt even to touch, yet appeared slightly hazy. Such traits indicate proper preparation, along with suitability for placement on epidermal layers. With firmness just enough to resist quick runoff, the product stays put - giving the working compound room to act efficiently.
The smooth texture made applying the gel straightforward, covering the skin evenly without resistance. Uniform distribution matters because it allows the active ingredient to reach all parts of the targeted area effectively. A nearly neutral pH marked another benefit, aligning with natural skin conditions - this balance supports comfort and lowers chances of stinging or inflammation.
Despite ongoing monitoring, no changes emerged in how the product looked, felt, or performed. Stability held firm across weeks, showing little sign of degradation. From start to finish, physical traits stayed unchanged. That steady behavior points toward reliable shelf performance. Over time, user handling would likely remain unaffected. Safety markers stayed within acceptable limits. Ease of use persisted through every phase observed. Throughout trials, dosing precision showed little variation. External factors had limited influence on internal structure. Batch uniformity supported repeatable outcomes. Patient access could benefit from such predictability. No signs pointed toward early breakdown. Overall response aligned with expectations at multiple stages.
REFERENCES

Mohnish Kumar, Praveen Kumar Sahu, Dr. Gyanesh Kumar Sahu, Suchita Wamankar, Dr. Chanchal Deep Kaur, Formulation and Evaluation of Allicin Based Topical for the Treatment of Psoriasis, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 1300-1310. https://doi.org/10.5281/zenodo.19475502
 10.5281/zenodo.19475502
10.5281/zenodo.19475502
