Mar Dioscorus College of Pharmacy, Hermongiri Vidyapeetam, Alathara, Sreekaryam, Thiruvananthapuram.
Acne vulgaris and chronological/photoaging are not only among the most common skin diseases globally, both are also increasing in age-standardized prevalence and economic burden. Conventional monotherapies (e.g., retinoids, benzoyl peroxide, and alpha-hydroxy acids) are hindered by poor patient compliance, irritation, microbial resistance, and insufficient repair of the extracellular matrix. The current project's objective is to develop a multi-targeted, plant-based solution for the management of acne vulgaris and the restorative slowdown of chronological/photoaging through the delivery of Coriandrum sativum (Apiaceae) leaf extract in a thermosensitive hydrogel formulation. The extract contains numerous bioactive constituents, including significant concentrations of linalool, quercetin, and phenolic compounds, all of which exhibit potential synergistic combinations of their antibacterial, antioxidant, and anti-matrix metalloproteinase activity to be more effective against Propionibacterium acnes and against the oxidative damage induced by UVB radiation compared to conventional antioxidants. The ethanol maceration technique developed preserved 85% or more of the extract's bioactive constituents, as demonstrated by multiple standard phytochemical analysis techniques. The incorporation of a Pluronic F127-based hydrogel formulation allowed the sol-to-gel transition of the phytoconstituents to occur at physiological temperature, to provide for extended skin residence times, and to control the release of both lipophilic and hydrophilic phytoconstituents from the formulation. The hydrogel formulation displayed excellent rheological properties, demonstrated significant antibacterial activity, and had an increased retention in the skin. Thus, the findings of this study provide support for the use of thermosensitive hydrogel-based phytotherapeutics as a new option for patient compliance for the management of acne vulgaris and for rejuvenating the skin.
Globally, the most prominent dermatological diseases are acne vulgaris as well as chronological/photoaging. Between 1990 and 2021, the age-standardized prevalence rates of these two skin diseases increased 8,563-9,790 per 100,000 persons for that same period, resulting in over $15 billion spent annually in direct treatment costs. The conventional monotherapy treatment options (i.e., retinoids, benzoyl peroxide, alpha-hydroxy acids) are poorly adhered to due to irritation (e.g., the incidence of retinoid dermatitis is 20-50%), Propionibacterium acnes resistance (i.e., 4-fold increase in MIC from 2010), and proven minimal restoration of the damaged extracellular matrix. Coriandrum sativum (Apiaceae) leaf extract has been shown to have multi-target bioactivity that addresses many of these problems. When used alone, Linalool (40-70% volatiles and MIC 25-50 μg/mL vs. P. acnes) and Quercetin (2.1-4.8 mg/g DW and IC50 132 μg/mL DPPH) work together with total phenolic content (18.5 mg GAE/g or 78% scavenging) to produce superior antibacterial, antioxidant and anti-MMP-1 effects than (epigallocatechin gallate) EGCG from green tea.
The ethanol maceration procedure allows 90% (1:10-16 w/v) ethanol to be used to extract >85% of the active ingredient at 45°C (as demonstrated by Shinoda (flavonoids++), Salkowski (terpenoids +), and FeCl3 (Phenolics +) tests). These same assays showed that the F127 contains thermally reversible gel properties and will gel between the respective ranges upon injection of 20% to 25% (w/v) using Pluronic F127 LCST (20-25°C) at room temperature. After room temperature, the system will undergo a sol-gel transition between 32°C and 37°C and have a 3-4x longer residence time than seen with carbomers (τ >6h).
The F127 micelles (CMC 2.6% w/v) will encapsulate lipophilic linalool while allowing the hydrophilic flavonoids to diffuse at a controlled rate. Based on this concept, the F4 formulations containing 25% of the extracted contents had a G' of 15-20 kPa, viscosities of 10,000-18,000 cP, and a zone of inhibition of at least 20 mm.
SKIN
The largest organ in humans is the skin. The skin consists of three different layers - the epidermis (outer layer), dermis (middle layer), and hypodermis (subcutaneous layer). The epidermis is composed of stratified, squamous epithelial cells that are made up of keratinocytes (dendritic cells, melanocytes, Merkel cells, and Langerhans cells). The epidermal layer can be further broken down by the number of layers in each layer of keratinocyte morphologies and their degree of differentiation into cornified cells (the outermost layer is called the stratum corneum). The dermis is composed of collagen and other amorphous CT that contains nerve and blood vessels (vascular/nerve tissue), fibrous tissue, hair follicles, sebaceous glands, eccrine sweat glands and ectodermal appendices like fibroblasts, macrophages and mast cells. The hypodermis or subcutaneous tissue is a true endocrine organ because it contains adipocyte lobules which are interspersed with fibrous septa and blood vessels. The various components of the skin can communicate with each other and with other tissues and provide for homeostasis through their production of cytokines, neurotransmitters and hormones, as well as the respective receptors for each of these substances; the neuro-immuno-endocrine function of the skin is closely linked to both central and peripheral regulatory systems in the human body. Additionally, the skin is a large reservoir for stem cells which can be activated to both regenerate the body surface and to heal wounds. All three layers of the skin assist in providing the body with a great many of its vital functions, such as the protection of the body from physical, chemical and biological insult; the prevention for excessive loss of body fluid; and the regulation of thermoregulation.
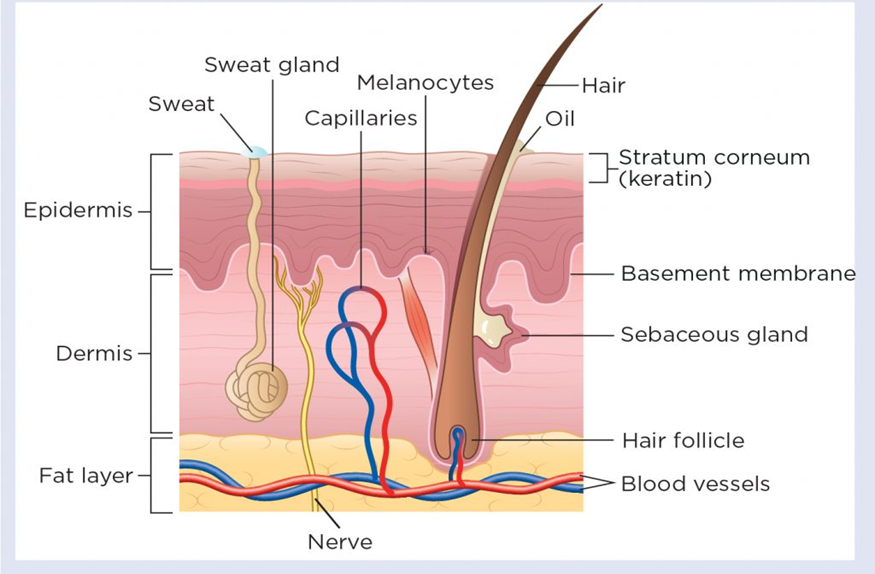
Figure 1. Cross section through the skin
EPIDERMIS
The outermost layer of skin is called the epidermis. It is made up of a layered arrangement of flat cells that are continually being produced and shed; most of these flat cells are keratin-forming cells (keratinocytes). Keratinocytes produce the protein keratin and make up most of the epidermis (i.e., they are what arrange themselves into layers). Because the epidermis is composed largely of keratin, it is a very strong, resilient, and somewhat flexible structure. The primary purpose of the epidermis is to provide an outer barrier protecting against irritants and allergens from the environment while preventing excessive water loss from the body (regulating internal temperature). The epidermis is composed of four layers in most body areas and five layers in thick skin (e.g., palms, soles, and fingers). The various layers of the epidermis are: Stratum corneum (the outermost layer): This layer consists of many layers of flattened (coenocytic) dead skin cells that have been filled with keratin and have waterproof properties. Stratum lucidum (found only in thick skin – palms, soles, fingers): The stratum lucidum is an extremely thin layer and consists of dead skin cells; the presence of this layer distinguishes thick skin from thin skin. The (granular layer) is the stratum granulosum and is where the flat, no nucleus cells will reach when moving up the strata. The stratum spinosum (prickle cell layer) is formed next from the stratum basale as cells move up. Cells in this layer, stratum spinosum, are adhering to each other through intercellular adhesive junctions, also called desmosomes. Within the stratum spinosum are special immunity cells called Langerhans, whose form is similar to a tree branch and grow from a bone marrow. The Langerhans are critical to skin-related immunological events. Stratum basale (germinative layer) is at the bottom of the epidermis directly next to the dermis and contains both dividing and non-dividing keratinocytes. The keratinocytes' inner/basal area contains little structures called hemi desmosomes. Basal layer cells have melanin (a pigment) called melanocytes.
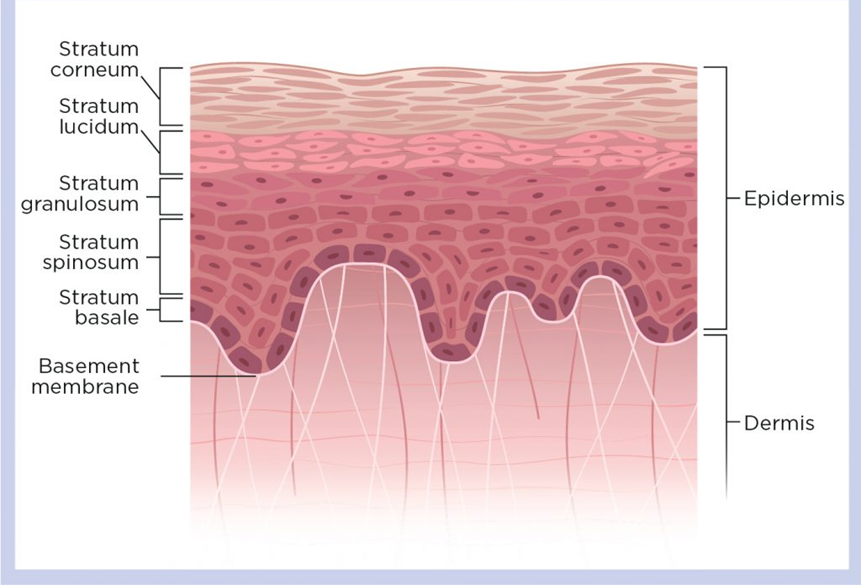
Figure 2. Layers of Skin
DERMIS
The dermal layer of skin is the innermost layer and is the largest layer of skin this layering - the epidermis averages (1.5mm) thick. The dermal layer of skin connects the outer epithelial layer to the subcutaneous fat layer, and it is the main job of the dermal to support and protect the epidermal. The structure and function of the dermal layer of skin includes:
Collagen is the predominant material present in the dermal layer of skin, and elastin is also present, since connective tissue is primarily made of the combination of two strands of collagen. In addition, several types of specialized cells inclusively distributed throughout the dermal layer of skin, including mast cells and fibroblasts, are located within the three-dimensional network of connective tissue that creates dermal structures. The main types of structures found in the dermal layer of skin include blood vessels, lymphatic vessels, sweat glands, and nerves. The epidermal appendages are located within the dermal and subcutaneous layers of skin but connect to the surface of skin.
The dermal layer of skin contains two distinct layers:
The papillary dermal layer is a thinner layer of loose connective tissue that contains many small blood vessels (capillaries), elastic fibers, and some collagen fibers. The reticular dermal layer is made of dense connective tissue with larger blood vessels and contains closely woven elastic fibers and thicker collagen fiber bundles, as well as specialized connective tissue cells such as fibroblasts, mast cells, and nerve cells. The dermis is surrounded by:
Mast cells in the dermis have granules containing vasoactive substances (histamine is one of) and play a role in regulating the immune and inflammatory reactions of the skin. Blood vessels in the dermis form a complex network which have an important role in thermoregulation. Blood vessels in the dermal region can be classed into two networks:
HYPODERMIS
The subcutaneous tissue below the dermis is called the hypodermis; It is composed mostly of adipose tissue. Hypodermis provides much of the structural integrity of skin while keeping us warm in cold weather and absorbing shocks. There are blood vessels and nerves that run through the hypodermis.
Functions of Skin: [4]
METHOD OF USEAGE
Transdermal drug delivery system
Thermosensitive hydrogels play an important role in transdermal drug delivery systems because of their superior biocompatibility, increased mechanical properties, simple formulation, and prolonged drug administration. Many researchers used thermosensitive hydrogel in smart patches and creams to treat dermal infections. Nirmayanti et al reported a thermos responsive hydrogel for the sustained release of valsartan to treat hypertensive patients through a transdermal drug delivery system. The proposed gel is composed of poloxamer 407 and Poloxamer 188 in varying amounts and their characteristics were found to be altered by poloxamer concentrations. The reported hydrogel subjected to characterization and in vivo testing, which demonstrated the enhanced characteristics including bioavailability in comparison to oral tablet[1].
Oral drug delivery system
Oral drug delivery is thought to be a promising route to cure diseases effectively, but it has certain limitations including low bioavailability. It causes severe side effects through the gastrointestinal tract because the liver digests the oral formulations before it reaches the target sites, so to overcome these issues researchers formulated the oral drugs with thermosensitive material vehicles to prevent the drug from being digested [2]. Ophthalmic drug delivery system
The eye is a major organ of the body that is very soft and sensitive. In general, doctors and professionals suggested eye drops for various ophthalmic problems such as glaucoma, amblyopia, and so on which could not reach the target locations due to the eye's biological barrier layers. The frequent use of eye drops can cause vision loss, so researchers developed smart hydrogels to address these problems [3].
Nasal medication delivery
Nasal administration is almost preferred by professionals to deliver proteins and peptides due to the large surface of the nasal mucosal membrane and it provides greater absorbance to the therapeutics as compared to oral administration. However, there are some challenges including proteolytic enzyme attack, macromolecule absorption, and so on, that need to be overcome if the choice of administration is nasal route [4]. Characteristics of thermosensitive hydrogels
Thermosensitive hydrogels synthesized using the above routes are expected to possess better thermal stability and fire resistance for their potential use in high temperature and fire-fighting application. The following subsection deals with various thermal and flame retardance properties of the thermosensitive hydrogels. Temperature-assisted mechanical behaviour
According to a recent research work, a heat-sensitive hydrogel, Pluronic F127 (PF127) remains in liquid state at room temperature but solidifies to form a semisolid gel at elevated temperatures. The fact that the PF-127 hydrogel is capable of transitioning from a liquid state around ambient temperature to an amorphous solid state at 37°C is evidence of its exceptional temperature sensitivity. The irregularities in the agarose gel medium were filled with PF127 hydrogel. Researchers tested ZnMet-PF127 hydrogel along with PF127 hydrogel at concentrations ranging from 10% to 25% to evaluate the gelation and stretchability. 20% of ZnMet-PF127 hydrogel began to gel at a temperature of about 20°C. There was little difference between PF127 hydrogel and ZnMet-PF127 hydrogel concerning gelation warmth and elastic modulus[7]. Crystallization behavior of thermosensitive hydrogels
The amorphous polymer-based hydrogel’s transformation rate to a crystalline material under the action of a temperature gradient is usually measured using differential scanning calorimetric analysis. It comprises two phases: nucleation and growth. Understanding the crystallization kinetics is vital in understanding the behavior of hydrogels under variations in temperature and other thermal properties. Usually, the degree of crystallinity (Xc) of a material can be calculated using the following Equation 1. It is measured from the area under the crystallization zone or the crystallization enthalpy of the hydrogel (ΔHm), mass of the material (m) and the enthalpy of the fully crystalline polymer (ΔHc-100%).’
????????=Δ?????????
????×Δ?????????–100%
Flame retardancy of thermosensitive hydrogels
Thermosensitive hydrogels are considered to be potential and sustainable alternatives to synthetic hydrogels for fire resistance applications. Analysis of conventional flame-retardant properties such as burning rates, smoke release rate, limited oxygen index, heat release rates, and other properties has been conducted by many researchers lately. In a recent research work, polyethylene glycol (PEG)-based thermosensitive hydrogels to retard the spontaneous combustion of coal in coal mines. When this hydrogel was applied onto the coals, the weight loss of the hydrogels was less than 6%, while the mitigation of CO was about 73%. These hydrogels exhibited strong fluidity and high temperature response at higher temperatures. The viscosity of the hydrogels increased rapidly after the phase transitions which gelled the pores of the coal retarding its rate of combustion[8].
Regulatory Framework
Under FDA 21 CFR 3.2(e), these are combo products requiring dual drug-device review pathways, with CMC dossiers proving polymer GRAS status (e.g., Poloxamer F127 per 21 CFR 172.820) and LCST reproducibility (±2°C). EMA follows MDR 2017/745 Class III classification, mandating Notified Body certification for novel excipients. ICH Q1A(R2)/Q8 mandates 6-month accelerated stability (40°C/75%RH) showing gel integrity and >90% drug assay. Sterilization using gamma (25–40 kGy) per USP <71> retains thermosensitivity versus. ethylene oxide residuals.
Safety Testing Requirements
ISO 10993-1 suite demands tiered biocompatibility: acute systemic (no edema), sensitization (score <1), genotoxicity (Ames negative), and 90-day implantation (minimal fibrosis). Extractables/leachables (USP <1661>) limit oligomers to <0.15% w/w; degradation via hydrolysis must yield biocompatible monomers. Clinical IND requires IRB-approved Phase I data on injection-site reactions [9].
APPLICATIONS OF THERMOSENSITIVE HYDROGEL
Thermosensitive hydrogels for ophthalmic diseases
Considering the eye as a reasonably independent organ, topical dosage of ophthalmic medications is the most favored and commonly acknowledged approach for many anterior segment eye illnesses attributable to its practical properties and non-invasiveness. However, conventional eye preparations suffer from multiple physiological protective barriers, including lachrymation, blinking, and nasolacrimal drainage, which result in extremely low bioavailability (< 5 %) and bring the development of local drug delivery great challenges [133,134]. Fortunately, thermosensitive in situ hydrogels can enhance drug bioavailability by avoiding the above-mentioned issues that can not only be administered as a liquid eye drop but also increase the drug's local retention
Thermosensitive hydrogels for rhinosinusitis
A promising delivery system called TEMPS (thermogel extended-release microsphere-based delivery to the paranasal sinuses) that could provide sustained steroid release for sinonasal mucosa inflammation has been designed by Steven R. Little group [131]. The combination of controlled-release microspheres with thermosensitive hydrogels could encapsulate corticosteroids and conform to the sinonasal mucosa by mimicking the native mucus layer for localized delivery to the sinuses.
Thermosensitive hydrogels for periodontitis
Utilizing this strategy, an injectable hydrogel prepared by CS, gelatin, and β-GP was applied to continuously release aspirin and erythropoietin (EPO), respectively. Clinically, repeated administration is required for aspirin and EPO due to their short half-lives. In this work, the releasing profile showed that the mixed hydrogels loaded with aspirin/EPO exhibited no toxicity and continued a sustained release
Thermosensitive hydrogels for osteogenesis
Poloxamer is an ABA-type triblock copolymer, which is particularly attractive material for biomaterial-guided gene vector delivery in a consistent and minimally invasive way. The data in a clinically relevant minipig model supported that thermosensitive hydrogels were capable of controlled release of a therapeutic rAAV vector overexpressing the chondrogenic sox9 transcription factor, and the early bone loss of subchondral bone plate reversed postoperatively.
Diabetic wounds
Chen suggested an injectable niobium carbide (Nb2C)-based hydrogel (Nb2C@Gel) with antioxidative and anti-infection properties, which was implanted Nb2C nanosheets into poly(lactic-co-glycolic acid) poly (ethylene glycol) poly(lactic-co-glycolic acid) (PLGA-PEG-PLGA) triblock copolymers. This composite hydrogel exhibited good biocompatibility and could efficiently eliminate ROS in DU. In addition, Nb2C@Gel was also a NIR-activatable hyperthermia-assisted antibacterial platform against both Escherichia coli and Staphylococcus aureus[10]
FUTURE OF THERMOSENSTIVE HYDROGEL
Hydrogels are extensively used in biomedical fields, particularly drug delivery, thanks to their biocompatibility, biodegradability, nontoxicity, and high water content. Their physically or chemically crosslinked polymeric networks allow precise control over physicochemical properties and spatiotemporal drug release. Key applications include wound dressings, tissue engineering, bio-sensing, bio-printing, and electrospinning. Growing interest focuses on stimuli-responsive hydrogels, modulated by temperature, pH, light, or ultrasound, acting as "smart" systems that protect labile drugs and enable on-demand release.
Synthetic thermo-responsive polymers like poloxamers (Pluronics®, e.g., PF127)—triblock copolymers of PEO-PPO-PEO—form viscous hydrogels at body temperature through hydrophobic micelle aggregation and supramolecular interactions. They suit transdermal, injectable, ophthalmic, and vaginal delivery. pNIPAm, with LCST near body temperature, enables fast switching; examples include sustained colchicine release to vascular cells, self-regulated nanofibrous systems, biodegradable levofloxacin-loaded gels, photo-thermal "pillows," and alginate-graft injectables for cell transplantation.
However, PF127 formulations can exhibit cytotoxicity (e.g., 40-90% cell viability in various lines), prompting shifts to bio-polymers. These natural-origin hydrogels offer rheological control, no cytotoxicity, enzymatic degradation, and metabolic byproduct removal. Blended with other biomaterials, they enhance drug delivery and tissue engineering, with promising transdermal prospects[11].
CONCLUSION
A revolutionary development in drug delivery, thermo-sensitive hydrogels allow for the regulated release of active ingredients at specific locations and the precise elimination of therapeutic obstacles. These cutting-edge injectable formats provide a practical and contemporary substitute for conventional delivery methods. Their creation promises an easy-to-use, mess-free, in-situ gelling mode of administration that will improve patient compliance and therapeutic efficacy. Hydrogels that are sensitive to temperature have the potential to be a crucial part of biomedical goods in the future. Hydrogel that are sensitive to temperature have the potential to be a crucial part of biomedical goods in the future.
ACKNOWLEDGEMENTS:
We want to offer this endeavor to GOD ALMIGHTY for all the blessings showered on us during the course of this review. We take the privilege to acknowledge all those who helped in the completion of the review. At first, we express a deep sense of gratitude and indebtedness to the Department of Pharmaceutics of Mar Dioscorus College of Pharmacy for helping in the completion of our review. We are extremely grateful to our principal for her guidance and valuable suggestions, which helped to complete our work. We are deeply obliged to Mrs. Lekshmi M.S Panicker, our guide as well as mentor, for her guidance, immense knowledge, insightful comments, constant support, and encouragement, which helped us complete our work within the time schedule. We express our sincere gratitude to Mrs. Praveena M, our co-guide, for sharing her expertise by giving constructive comments and suggestions upon reviewing our study.
REFERENCES

Lekshmi M.S Panicker, Praveena M V, Al Sahir N, Jude Ron Lenic, Farsana N, Formulation and Evaluation of Anti-Acne and Anti-Ageing Thermosensitive Hydrogel, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 1897-1906. https://doi.org/10.5281/zenodo.18621515
 10.5281/zenodo.18621515
10.5281/zenodo.18621515
