
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Al-Ameen College of Pharmacy, Bengaluru 560027
The common neurological condition known as epilepsy is typified by frequent seizures. Despite their effectiveness, traditional antiepileptic medications frequently have negative side effects and resistance problems. Epilepsy affects fifty million individuals globally, accounting for around one-third cases still have uncontrollable seizures and bad drug responses even though there are several antiepileptic medications (AEDs) available. Due to this restriction, there is now more interest in alternative and traditional medicine, especially plant-based treatments, many of which have been practiced for millennia in many different cultures. Using a variety of mechanisms, including GABA modulation, NMDA receptor antagonism, and antioxidant activity, medicinal plants have become popular alternative medicines with anticonvulsant effects. A comprehensive overview of medicinal plants historically utilized for the treatment of epilepsy is what this review attempts to provide, including ethnobotanical knowledge, phytochemical ingredients, pharmacological research, and suggested mechanisms of action. In preclinical and restricted clinical contexts, plants have shown encouraging anticonvulsant and neuroprotective properties.
Herbal medicines are often regarded as advantageous compared to conventional antiepileptic drugs due to several factors. Numerous civilizations have long used them traditionally, and hundreds of plant species have been studied for their anticonvulsant qualities
(1) Herbal remedies typically contain multiple bioactive compounds that can act synergistically, targeting different mechanisms such as enhancing GABAergic transmission, inhibiting glutamate release, modulating ion channels, and providing antioxidant effects (1,2,3). This multimodal action may offer broader neuroprotection and seizure control. Additionally, herbal medicines are generally more accessible and affordable, especially in resource-limited settings, and are perceived to have fewer side effects than synthetic drugs (2). However, because most research is based on animal models and preclinical data, there is a dearth of solid clinical evidence supporting the safety and effectiveness of the majority of herbal remedies, despite these possible advantages. Therefore, evidence-based inspection of herbal medications is necessary (1) and their use should be carefully considered alongside conventional therapies, especially given the variability in herbal preparations and the potential for drug interactions (2,3).
Limitation of conventional drugs
Modern pharmacological treatment primarily involves antiepileptic drugs (AEDs) that act through mechanisms such as enhancing GABAergic inhibition, modulating ion channels, or inhibiting excitatory neurotransmission. While AEDs like phenytoin, valporic acid, carbamazepine, and levetiracetam are commonly used, they are not curative and merely control symptoms (4). Approximately 30% of individuals are deemed pharmaco-resistant, which means that even after taking two or more AEDs, their seizures do not subside (5). Additionally, AEDs often come with adverse effects including sedation, dizziness, cognitive impairment, hepatotoxicity, and teratogenicity (6,7). Tolerance, medication interactions, and a decline in quality of life might result from prolonged use. These limitations have driven researchers and clinicians to explore alternative therapies, especially from natural sources (6)
Epilepsy
The neurological condition known as epilepsy is typified by a predisposition to produce repeated, unprovoked seizures brought on by aberrant brain electrical action. When two or more unprovoked seizures occur more than twenty-four hours apart, or when a single seizure has a significant chance of reoccurring because of an underlying brain problem, a clinical diagnosis is usually made (8). Epilepsy is a condition that affects individuals of all ages and is characterized by a variety of symptoms, such as sensory disturbances, involuntary movements, and altered awareness.
Classification of epilepsy
The classification of epilepsy has evolved significantly, with the International League Against Epilepsy (ILAE) providing the most widely accepted framework. The 2017 ILAE classification introduces a three-level approach (9)
A. Seizure Type Classification
Based on onset:
a. Focal Onset Seizures (start in single hemisphere of the brain only)
b. Generalized Onset Seizures (start in both hemispheres simultaneously)
c. Unknown Onset Seizures
B. Epilepsy Type Classification
Based on seizure type and EEG/imaging:
C. Epilepsy Syndrome Classification
An Epilepsy syndrome is the cluster of features (e.g., age of onset, types of seizures, EEG pattern, genetics). Examples: Childhood absence epilepsy, Juvenile myoclonic epilepsy, Lennox-Gastaut syndrome.
Mechanism of action
Herbal plants exert their anticonvulsant effects through several detailed mechanisms that target the underlying neurobiology of epilepsy. The major mechanisms of action identified in recent research include
Some plant extracts inhibit the glutamate release or antagonize NMDA receptors, reducing excitatory neurotransmission that can trigger seizures. For example, Lavandula officinalis inhibits glutamate release and blocks calcium channels, while Panax ginseng inhibits NMDA receptor-mediated calcium influx (1,10,11)
Many herbal anticonvulsants reduce neuronal excitability by inhibition of voltage-gated Na+, K+, or calcium channels. This action stabilizes neuronal membranes and diminishes the likelihood of abnormal, excessive firing that leads to seizures (12)
Chronic Neuroinflammation contributes to seizure susceptibility and epileptogenesis. Certain herbal medicines suppress inflammatory mediators and modulate immune responses in the brain, providing neuroprotection and reducing seizure frequency (1,10,11)
The pathophysiology of epilepsy is linked to mitochondrial malfunction and oxidative stress. Strong antioxidant qualities found in herbal substances help shield neurons from seizure-induced damage by scavenging free radicals and enhancing mitochondrial activity (10,11)
The main inhibitory neurotransmitter in the brain, gamma amino butyric acid (GABA), is enhanced by a large range of chemicals produced from plants. They may act as GABA receptor agonists or positive allosteric modulators, thereby increasing inhibitory synaptic transmission and suppressing seizure activity (1,10)
Some herbal compounds modulate protein synthesis, autophagy, and metabolic pathways, which can influence neuronal survival and excitability. This includes effects on pathways such as PI3K/Akt/GSK-3 and mTOR signaling, which are involved in cell growth, survival, and neuroprotection (1,10,11)
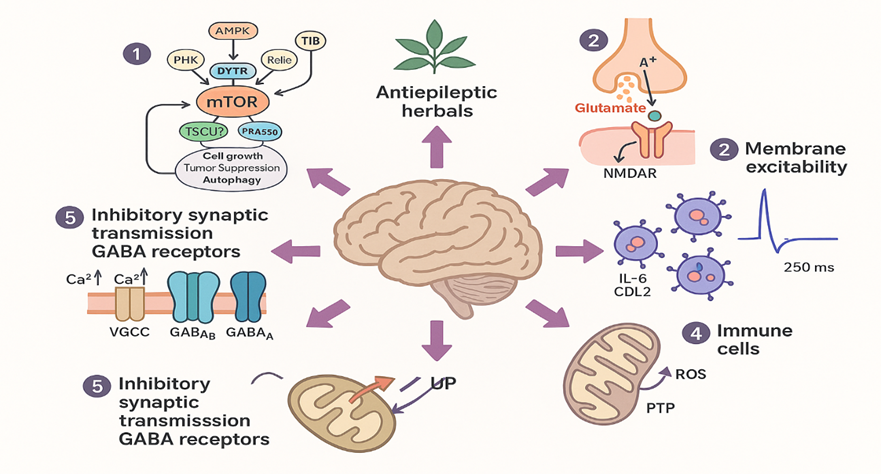
Fig 1: Mechanism of action of some herbal plants exhibiting antiepileptic activity
Influence of Traditional Plants and Medicines
Medicinal plants are increasingly recognized for their significant role in epilepsy management, owing to their broad-spectrum therapeutic properties, favorable safety profiles, and accessibility. Numerous phytochemicals and plant extracts have exhibited anticonvulsant activity in preclinical models by modulating critical targets such as gamma-aminobutyric acid (GABA) receptors, N-Methyl-D-aspartate (NMDA) receptors, and various ion channels implicated in seizure initiation and propagation. These compounds often exert multifaceted effects, including the regulation of excitatory and inhibitory neurotransmission, antioxidant activity, and anti-inflammatory responses, thereby contributing to their neuroprotective potential. Compared to conventional antiepileptic drugs, medicinal plants are typically more cost-effective, widely available, and associated with fewer adverse effects, making them particularly advantageous in low- and middle-income countries with limited access to modern pharmacotherapy. Despite promising preclinical outcomes, further research is necessary to elucidate their precise mechanisms of action, establish standardized dosages, and ensure clinical safety. The World Health Organization has endorsed the integration of plant-based medicines into healthcare systems due to their therapeutic efficacy and reduced risk profiles. Notably, cannabidiol (CBD), a phytochemical derived from Cannabis indica, has received regulatory approval for the treatment of certain severe epileptic syndromes, underscoring the potential of plant-derived compounds in epilepsy therapy. Overall, medicinal plants represent a valuable and underutilized resource in the development of safer, effective, and accessible treatment options for epilepsy. (12,13,14,15).
Prevalence and Epidemiology of Epilepsy
Systematic reviews and meta-analyses estimate the global point prevalence of active epilepsy at approximately 6.4 per 1,000 individuals, with a lifetime prevalence of around 7.6 per 1,000. The annual cumulative incidence is reported at 67.8 per 100,000 individuals, while the incidence rate stands at roughly 61.4 per 100,000 person-years. These epidemiological indicators are significantly elevated in low- and middle-income countries (LMICs), where the median incidence reaches 81.7 per 100,000, in contrast to 45.0 per 100,000 observed in high-income countries (HICs). This disparity is largely attributed to inadequate healthcare infrastructure, a higher burden of central nervous system infections, and an increased prevalence of perinatal complications in LMICs. (16,17)
Globally, the burden of epilepsy is most pronounced in regions such as Africa and Latin America, with the highest incidence rates observed in the Middle East and Latin America. Current estimates indicate that approximately 51.70 million individuals are living with active epilepsy worldwide. Moreover, around 4.6 million new cases are reported annually, highlighting the substantial and ongoing public health challenge posed by this neurological disorder.(18)
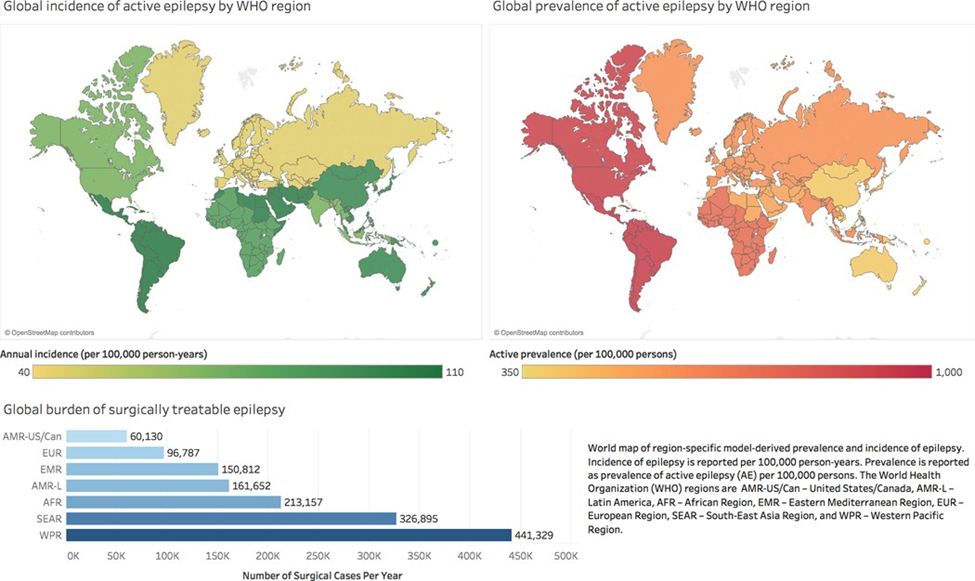
Fig 2: World map of the prevalence and epidemiology of active epilepsy by WHO (18)
Epilepsy and Phytotherapy
Phytotherapy, the use of medicinal plants for therapeutic purposes, has gained attention as a complementary or alternative strategy for epilepsy management, particularly in cases where conventional antiepileptic drugs (AEDs) prove ineffective or elicit significant side effects. Approximately one-third of individuals with epilepsy fail to achieve complete seizure control with standard pharmacological treatments, leading to increased interest in traditional herbal remedies. (19,20). Several plants, including Carum carvi L. and Punica granatum, have demonstrated anticonvulsant and sedative effects, likely mediated through modulation of GABAergic neurotransmission (20). Similarly, herbs such as Ocimum sanctum and Citrus sinensis, commonly used in traditional Indian medicine, exhibit neuroprotective and seizure-modulating properties through antioxidant activity and GABA-mimetic mechanisms (21). Recent studies have also emphasized the therapeutic potential of cannabidiol (CBD), a phytochemical derived from Cannabis sativa, in managing drug-resistant epilepsy syndromes like Dravet syndrome, primarily through its influence on the endocannabinoid system and neuronal excitability (22). These medicinal plants are rich in diverse bioactive constituents—such as flavonoids, alkaloids, and terpenoids—which are thought to underlie their anticonvulsant and anti-inflammatory actions (23). Despite promising preliminary findings, further well-designed clinical trials and efforts toward standardization are crucial to validate the efficacy and safety of plant-based interventions in epilepsy treatment.
Table 1: Plants with Reported Antiepileptic Activity: Family, Parts Used, and Bioactive Compounds (24-69)
|
Biological Name |
Family |
Parts |
Active constituents |
|
Acalypha indica |
Euphorbiaceae |
Aerial part |
Alkaloids, Terpenoids, Flavonoids |
|
Allium cepa L. |
Liliaceae |
Bulb |
Alkaloids, flavonoids, phytosterols |
|
Annona senegalenesis |
Annonaceae |
Leaf |
Acetogenins, alkaloids, flavonoids, terpenes, saponins |
|
Arenaria kansuensis |
Caryophyllaceae |
Whole Plant |
Flavonoids |
|
Artemisia Persia |
Asteraceae |
Whole Plant |
Flavonoids and phenols, Artemisinin |
|
Asterothamnus centrali-asiaticus |
|
Whole Plant |
Flavonoids |
|
Biophytum umbraculum |
Oxalidaceae |
Root |
Flavonoids, phenols, tannins, steroids, terpenoids |
|
Butea monosperma |
Fsabaceae |
Stem |
Flavonoids and steroids |
|
Calotropis procera |
Apocynaceae |
Leaf |
Alkaloids, saponins, and sterols |
|
Canarium schweinfurthii |
Burseraceae |
Stem |
Flavonoids, sterols, phenols |
|
Cannabis sativa |
Cannaceae |
Aerial part |
Cannabinoids, terpenes, flavonoids |
|
Carissa edulis |
Apocynaceae |
Root |
Anthraquinone, tannins, saponins, flavonoids |
|
Carum carvi L |
Apiaceae |
Seed |
Tannins, alkaloids, and terpenoids |
|
Azima Tetracantha |
salvadoraceae |
Root |
Alkaloids, flavonoids, glycosides, terpenoids |
|
Citrullus colocynthis |
Curcurbitaceae |
Fruit |
Glycosides, flavonoids, alkaloids |
|
Citrus Sinensis |
Rutaceae |
Leaf |
Flavonoids, essential oils, phenolic acids |
|
Clerodendrum viscosum |
Verbenaceae |
Leaf |
Flavonoids, terpenes and phenols |
|
Cocos nucifera L. |
Arecaeae |
Root |
Phenols, amino acids, medium chain fatty acids |
|
Combretum micranthum |
Combretaceae |
Root |
Flavonoids , saponins, tannins, terpenoids |
|
Commiphora wightii |
Burseraceae |
Resin |
Guggulsterones, terpenoids, flavonoids, polyphenols |
|
Datura stramonium |
Solanaceae |
Leaf |
Flavonoids, alkaloids, steroids and saponins |
|
Evolvulus alsinoides |
Convolvulaceae |
Aerial Part |
Flavonoids, phenols, tannins, steroids, terpenoids |
|
Ficus abutilifolia |
Moraceae |
Root |
Flavonoids , saponins, tannins, terpenoids |
|
Ganoderma lucidum |
Ganodermataceae |
Mycelium |
Triterpenoids, alkaloids, flavonoids, phenols |
|
Grewia tiliifolia |
Tiliaeceae |
Aerial Part |
Phenols, flavonoids, alkaloids, steroids and saponins |
|
Ipomoea reniformis |
Convolvulaceae |
Leaf |
Phenols, flavonoids, alkaloids, steroids and saponins |
|
Lavandula dental L |
Lamiaceae |
Leaf |
Flavonoids, terpenoids, phenols |
|
Nelumbo nucifera |
Nymphaeaceae |
Fruit |
Flavonoids, alkaloids, saponins, tannins |
|
Ganoderma curtisii |
Ganodermataceae |
Mycelium |
Triterpenoids, alkaloids, steroids, flavonoids |
|
Madhuca longifolia |
Sapotaceae |
Wood |
Alkaloids, flavonoids, terpenoids, saponins |
|
Marsilea quadrifolia |
Marsileaceae |
Leaf |
Polyphenols, flavonoids |
|
Matricaria reticulate |
Asteraceae
|
Flower |
Phenols, flavonoids, alkaloids |
|
Milicia excels |
Moraceae |
Leaf |
Phenols, flavonoids, alkaloids |
|
Nardostachys jatamansi |
Caprifoliaceae |
Root |
Sesquiterpenes, alkaloids, phenols, flavonoids |
|
Ocimum sanctum |
Lamiaceae |
Leaf |
Flavonoids, alkaloids, tannins, steroids, glycosides, |
|
Pergularia daemia |
Asclepiadaceae |
Root |
Cardenolides, phenols, alkaloids, flavonoids |
|
Phyllanthus amarus |
Euphorbiaceae |
Aerial Part |
Lignin, glycosides, tannins, steroids, and phenol |
|
Ocimum basilicum |
Lamiaceae |
Leaf |
Phenolics, flavonoids, alkaloids, tannins, steroids |
|
Pseudospondias macrocarpa |
Anacardiaceae |
Leaf |
Alkaloids, phenols, flavonoids |
|
Punica granatum |
Punicaceae |
Leaf |
Polyphenols, flavonoids |
|
Bupleuri Radix |
Apiaceae |
Root |
Saikosaponin, tannins |
|
Rosmarinus officinalis L |
Labiatae |
Leaf |
Alkaloids, phenols, flavonoids, essential oil |
|
Silybum marianum |
Asteraceae |
Seed |
Flavonoid, alkaloids, phenols |
|
Terminalia chebula |
Combretaceae |
Fruit |
Tannins, flavonoids |
|
Aloe vera |
Asphodelaceae |
Leaf |
Anthraquinones, Polysaccharides, Saponins, flavonoids |
|
Uncaria rhynchophylla |
Rubiaceae |
Aerial Parts |
Alkaloids, triterpenoids, coumarins, glycosides |
|
Vateria indica |
Dipterocarpaceae |
Bark |
Flavonoids, phenolics, tannins, saponins |
|
Viola tricolor |
Violaceae |
Leaf |
Flavonoids, saponins, anthocyanin, coumarins, |
|
Vitex negundo |
Verbenaceae |
Leaf |
Flavonoids, phenolics, tannins, saponins |
|
Withania coagulans |
Solanaceae |
Fruit |
Alkaloids, flavonoids, tannins |
Table 2: Plants with Antiepileptic Potential: Mechanistic Approaches and In-Vivo Evaluation Models (24-69)
|
Biological Name |
MOA |
Animal Model |
|
Acalypha indica |
Enhanced GABA levels in neurons |
MES & PTZ model in Mice |
|
Allium cepa L. |
Modulates GABA receptors |
MES & PTZ model in Mice |
|
Aloe vera |
Inhibit NMDA-induced retinal ganglionic cell apoptosis |
MES & PTZ model in Mice |
|
Annona senegalenesis |
Enhance GABAergic neurotransmission |
PTZ model in Rats |
|
Arenaria kansuensis |
Binds benzodiazepine site of GABAA |
PTZ model in Mice |
|
Artemisia Persia |
Reduces oxidative stress and inflammation (IL-1β, TNF-α inhibition) |
PTZ model in Mice |
|
Asterothamnus centrali-asiaticus |
Binds GABAAR; anticonvulsant activity |
PTZ model in Mice |
|
Azima Tetracantha |
Antagonizes the inhibitory GABAergic neurotransmission and Ca+ channel blockade |
MES & PTZ model in Mice |
|
Biophytum umbraculum |
Increase in GABAergic neurotransmission |
MES& PTZ model in Mice |
|
Bupleuri Radix |
NMDA receptor inhibition; mTOR pathway modulation |
PTZ model in Rats |
|
Butea monosperma |
GABA mediated synaptic inhibition |
MES& PTZ model in Mice |
|
Calotropis procera |
Activation of the GABAergic neurotransmittion |
PTZ , picrotoxin, & strychnine-model |
|
Canarium schweinfurthii |
Prolonging the inactivation of sodium channels and modulate GABAA receptor complex |
PTZ, MES model in Mice |
|
Cannabis sativa |
Modulates GABA receptors |
Phenobarbitone & PTZ model in Mice |
|
Carissa edulis |
Enhancing GABAergic neurotransmission action |
MES,INH, PTZ model in Mice |
|
Carum carvi L |
Modulation of the GABAergic system |
PTZ model model in Mice |
|
Citrullus colocynthis |
Modulating the activity of GABA receptor complex |
PTZ model in Mice |
|
Citrus Sinensis |
Enhances GABAergic activity |
PTZ model in Mice |
|
Clerodendrum viscosum |
Blocking sodium channel |
MES model in Mice |
|
Cocos nucifera L. |
Voltage dependent Na+ channel blockage |
MES PTZ model in Mice |
|
Combretum micranthum |
Ion channel modulation |
MES model |
|
Commiphora wightii |
Modulation of ion channel and GABAergic neurotransmission |
PTZ model in Mice |
|
Datura stramonium |
Modulation of gamma-aminobutyric acid (GABA) and (5-HT) receptors |
PTZ model in Mice |
|
Evolvulus alsinoides |
GABAergic modulation; antioxidant |
PTZ model in Mice |
|
Ficus abutilifolia |
Ion channel modulation |
MES model |
|
Ganoderma curtisii |
Stimulation of GABAergic neurotransmission |
Kainic acid, PTZ, Strychnine model |
|
Ganoderma lucidum |
Stimulation of GABAergic neurotransmission |
Kiana acid, PTZ, Strychnine |
|
Grewia tiliifolia |
GABA receptor agonist; NMDA receptor |
PTZ model |
|
Ipomoea reniformis |
Restoring the GABA level |
MES, PTZ, INH models |
|
Lavandula dental L |
Stimulation of GABAergic neurotransmission |
PTZ model in Mice |
|
Madhuca longifolia |
Na+ channel blockage, NMDA blockage, Ca2+ channel blockage or by Modulation GABA receptors |
MES, PTZ Lithium- pilocarpine model in Mice |
|
Marsilea quadrifolia |
Antioxidant; GABAergic modulation |
PTZ model in Rats |
|
Matricaria reticulate |
GABA receptor modulation; anti-inflammatory |
PTZ model in Mice |
|
Milicia excels |
Blocking the presynaptic inhibition mediated by GABA |
PTZ model in Mice |
|
Nardostachys jatamansi |
Enhancement of GABAergic Activity |
PTZ & MES induces seizure in Rats |
|
Nelumbo nucifera |
Modulates GABA receptors |
Strychnine seizure model in Mice |
|
Ocimum basilicum |
GABAergic modulation |
PTZ model model in zebra fish |
|
Ocimum sanctum |
NMDA receptor antagonism |
MES model in Rats |
|
Pergularia daemia |
↑ GABA (240%), ↓ GABA-T activity; anti-inflammatory, antioxidant |
PTZ model in Mice |
|
Phyllanthus amarus |
Modulates GABA receptors |
PTZ model in Mice |
|
Pseudospondias macrocarpa |
Targets GABAergic, NMDA, K+ channels, and nitric oxide pathways |
Multiple seizure model in Mice |
|
Punica granatum |
Antioxidant; GABA modulation |
MES induces seizure in Mice |
|
Rosmarinus officinalis L |
Enhancement of GABAergic Activity |
Kainic Acid model in Mice |
|
Silybum marianum |
Modulates Ion channels |
PTZ model in Mice |
|
Terminalia chebula |
Decrease in synaptic release NMDA or glutamate |
MES, PTZ model in Rats |
|
Uncaria rhynchophylla |
NMDA receptor inhibition; Na+ channel modulation |
Pilocarpine model in rat |
|
Vateria indica |
Increases GABA levels (via L-glutamate decarboxylase activation); antioxidant effects |
MES, INH, PTZ models in Mice |
|
Viola tricolor |
Modulation of GABAA receptors. |
PTZ& MES model in Mice |
|
Vitex negundo |
Modulating GABAergic pathways and blocking sodium (Na) channels |
MES model in Mice |
|
Withania coagulans |
Inhibition of Na+ channels, GABAA receptor agonists |
MES,PTZ & Strychnine Model in Mice |
CONCLUSION
The exploration of traditional medicinal plants as antiepileptic agents has unveiled a diverse pharmacopeia of botanicals with promising anticonvulsant potential, as substantiated by a growing body of experimental evidence, particularly from animal models. This review underscores the therapeutic relevance of several key plants. The mechanisms identified include enhancement of GABAergic transmission, inhibition of glutamatergic excitotoxicity, modulation of ion channels (Na?, Ca²?), antioxidant activity, and anti-inflammatory effects critically involved in the pathophysiology of epilepsy.
The active constituents D-limonene, carvone, alpha-pinene, linalool of carum carvi L has shown promising antiepileptic effect. The (S)-(+)-carvone has increases the latency of the convulsion and cyanocarvone, increases the activity of acetylcholinesterase enzyme that blocks voltage gated Na+ channel which reduces the nerve excitability with modulation of GABAergic system, whereas linalool have direct interaction with NMDA receptor complex also modifies acetylcholine mechanism.
Animal studies have provided compelling evidence of these plants' ability to delay seizure onset, reduce seizure severity, and prolong survival in chemically or electrically model models. Moreover, phytochemicals such as flavonoids, alkaloids, and terpenes found in these plants are believed to contribute synergistically to their anticonvulsant effects. Despite these promising findings, a translational gap remains between traditional knowledge, preclinical validation, and modern clinical application. The variability in plant extracts, lack of standard dosing protocols, and limited human trials present ongoing challenges. Future research should prioritize the isolation of active compounds, elucidation of precise molecular targets, and rigorous clinical evaluations to develop safe, standardized, and effective phototherapeutics for epilepsy.
In conclusion, traditional medicinal plants offer a valuable, underexplored resource for antiepileptic drug development. Integrating ethnobotanical knowledge with modern pharmacological research holds the potential to expand therapeutic options, particularly for individuals with drug-resistant epilepsy or those seeking complementary approaches to seizure management.
REFERENCES



Nethravathi N, Dr. Rupesh Kumar M, Manjunath C, Ethnopharmacological Approaches to Epilepsy: Mechanisms and Preclinical Evaluation of Traditional Medicinal Plants, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 2643-2656. https://doi.org/10.5281/zenodo.17182931
 10.5281/zenodo.17182931
10.5281/zenodo.17182931