Kamalakshi Pandurangan College of Pharmacy, Ayyampalayam, Tiruvannamalai.
BMIs or value BCIs are the devices still in progress which create a couple connection of the outer workings of a device with a human body and brain for the purposes of a direct inter device intravital communication. They depend on, at the very least, invasive extraction and decoding of some brain activity which is captured through either non-invasive or invasive methods, and translated into motions of speech that can be understood by hand, or robotic arms, and computers. BMIs were first aimed at clinically assisting patients with neurologic disorders such as ALS, and spinal cord injuries, but have now expanded to gaming and virtual reality, alongside non-medical fields. BMIs, in their very basic form, encompass different parts such as acquisition of signal or neural signals, procession of undertones through, intention discerning by the aid of machine, learning, and an effector that will carry out the commands. A feedback loop that allows the device to dynamically adapt and learn over time provides the inbuilt greater functionality and ease of use flexibility. Electroencephalography enables the non-invasive method of signal capture while surgery complicated. The article analyzes several dimensions of BMI technologies such as their development and categorisation, elements, advantages and disadvantages, future prospects and applications, and examines BCIs within the context of neurologic disease management.
Humans have long dreamed of creating gadgets that can see into people's minds and thoughts or of being able to engage and communicate with technology just through thinking. Ancient mythology and contemporary science fiction tales are examples of how these concepts have captivated people's imaginations. However, the ability to directly connect with the human brain has only just begun to be made possible by developments in cognitive neuroscience and brain imaging technologies(1). This capability is enabled by the use of sensors that are able to track some of the physiological processes that take place in the brain in relation to particular types of cognition(2). Contrary to popular belief, it is possible to operate a computer solely using mental power. With the help of braincomputer interfaces, which enable computers to read and interpret signals straight from the brain, quadriplegics, people with 'locked-in syndrome,' and stroke victims can now move their own wheelchairs and even pour themselves coffee from a cup by using their brain waves to control a robotic arm. Direct brain implants have also assisted those who have lost their sight in regaining some of their lost vision(3). Integrating technological progress with neuroscience, BCI technology shows the benefits of multidisciplinary cooperation. In electrode implantation, neurosurgeons are absolutely essential to guarantee less tissue damage (4). While material science helps to improve implant safety and stability (5), this discipline combines biomedical engineering, neurology, computer science, and artificial intelligence to examine neural data and create algorithms. Through significant gains in patient quality of life and the treatment of neurological diseases, such cooperative efforts forward BCI technologies (2). BCI has been a vibrant field of study with an array of stimulating opportunities(6) since Vidal’s inception in 1973 (7-15). Scientists have, for illustration, recorded impressive results showing that BCI can effectively recover the capabilities of people with disabilities, including individuals with symptoms of schizophrenia (psychosis, influential problems, and cognitive dysfunction) (16–22). Based on industries classifications of BCI functions include video games and entertainment (23–25), security and authentication (26), healthcare (22), education (27–29), advertising and neuromarketing (commercial marketing based on cognitive science and neuroscience principles) (30-34), and neuroergonomics (application of biology to ergonomics) (35,36). Because it touches on many different areas of advancements, BCI might keep going to be a popular and competitive field of study for some time to come.
3.Elements of BCI:
The complex system that converts brain activity into executable commands is known as a fully functional Brain-Machine Interface (BMI). Designing reliable and efficient BMI systems requires an understanding of each component. The BMI pipeline's essential elements are as follows.
3.1 Acquisition of signals:
Electrodes or sensors are used to record brain activity at the start of the procedure. The technique employed (ECoG, intracortical electrodes, or EEG) determines the kind and calibre of data acquired. While non-invasive techniques (like EEG caps) yield safer but noisier data, invasive techniques (like Utah array) yield high-resolution spike data. High temporal resolution, low noise levels, and biocompatibility (for implants) are essential requirements(37).
3.2 Preprocessing of signals:
Noise and artefacts from external electronics, blinking, and muscular action are frequently present in raw brain data. Signal quality is enhanced by preprocessing methods including normalisation, artefact rejection, and bandpass filtering. Quick Fourier Transform (FFT), Independent Component Analysis (ICA), and Bandpower computation (e.g., alpha, beta waves) are some of the methods used(38).
3.3 The Extraction of features:
Analysed preprocessed signals help to extract useful information reflecting the intention of the user. Typical elements are spectral power, amplitude variations, and event-related potentials (ERPs). Notable Techniques: P300, SSVEP patterns; common spatial patterns (CSP); event-related desynchronization (ERD)(39).
3.4 Algorithms for classification and translation:
Machine learning techniques arrange the acquired features into relevant commands. These methods can be unsupervised (e.g., clustering’s) or supervised (e.g., SVM, LDA, CNNs). Actions: Sort user intent (left vs. right movement) then translate mental states into useful outputs(40).
3.5 Output Equipment (Effector):
The last result of the classifier is sent to an external gadget (such as a wheelchair, robotic arm, cursor) that does the desired action. Illustrations include: Medical: speech synthesizer’s, prosthetic limbs Commercial: Virtual reality headsets, gaming controllers(41).
3.6 Loop of Feedback:
Real-time feedback included in some BMIs lets users hone their mental methods for greater control. Feedback could be haptic (vibrations), aural (beeps), or visual—that of a screen display(42).
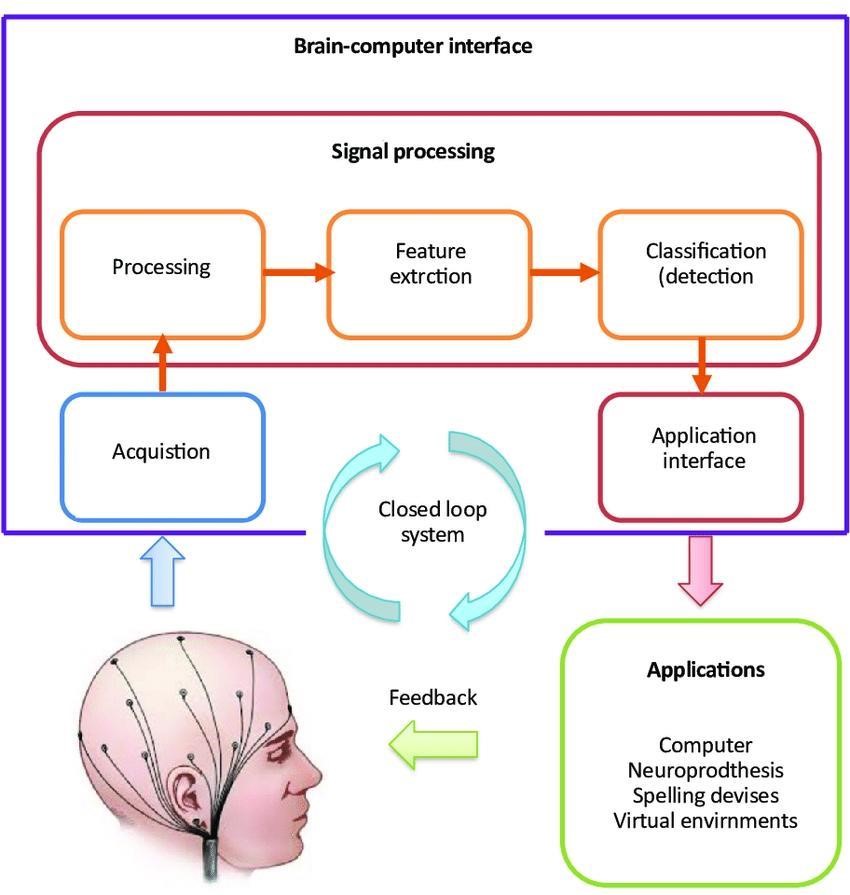
Fig no: 1 Block Diagram of BCI
4.Development And Categorization of BCI:
The evolution of BCI technology has experienced several transforming phases, as shown in With a thorough narrative given in Supplementary File 1 (Supplemental Digital Content 1, http://links.lww.com/JS9/ D262); these phases are classified as the Academic Exploration Phase, the Scientific Validation Phase, and the Experimental Application Phase. Every phase has greatly improved our understanding and ability for directly engaging with the human brain. Three invasiveness levels define BCI technology: intrusive, non-invasive, and semi-invasive. Though with surgical risks and biocompatibility problems, invasive BCIs offer great signal quality and precise control by implanting electro-des straight into the cerebral cortex(43,44). Although they have lower signal quality and are vulnerable to environmental noise interference, non-invasive BCIs fit for first brain function studies and clinical diagnosis since they use external electro-encephalography (EEG) electrodes to detect brain signals with minimal risk(40,45,46). By placing electrodes in sub-dural or subcortical brain areas, semi-invasive BCIs balance fewer risks than invasive techniques with better signal quality than non-invasive approaches(47,48). Moreover, BCIs are categorized as either bidirectional, which allow interactive communication by means of feedback from the device to the brain, so improving control and response for advanced applications, or unidirectional, which transmit signals just from the brain to a device, so limiting feedback and adaptation(4,49).Choosing a BCI system requires careful consideration of these traits against the particular needs of patients and the expected uses(50).
5.Investigations Into BCI For the Management of Neurological Disorders:
5.1 Motor dysfunction:
5.1.1 Epilepsy:
Epilepsy can be described as a paroxysmal condition caused by recurrent aberrant and synchronised neuronal activity(51). Its causes include tumor’s, traumatic injuries, genetic predispositions, and sometimes unknown causes. It usually shows up as symptoms like moderate distraction, autonomic nervous system dysfunction, convulsions, and altered consciousness. In more extreme cases, it might also include behavioral and cognitive changes, which differ in kind and severity from person to person (52). The main areas of study for BCI technology in epilepsy research include neural signal recognition, seizure prediction, seizure origin localization, and closed-loop stimulation treatment improvement. Neural signal detection methods include conventional EEG and its improved forms, including functional magnetic resonance imaging (fMRI) and enhanced video EEG monitoring. Early seizure warnings are made possible by researchers building epilepsy prediction models from neural electrical impulses using machine learning methods. The accurate localization of seizure foci is made possible by advanced imaging technology. The goal of closed loop stimulation treatments is to detect seizure signals in real time and then activate devices for either medication release or brain manipulation to lessen seizures. According to observations, there is a crucial phase connection between cortical neuron discharges and micro-ECoG signals, which is impacted by a number of variables, including outside factors, spatial separation, brain state, and cortical architecture (53). This knowledge is essential for improving BCI technology and understanding the origins of ECoG signals. Smith (2005) notes the limitations of EEG in the treatment of epilepsy, including its limited spatial and temporal coverage, but emphasises how essential it is for identifying, categorizing, and treating epilepsy because of its affordability, convenience, and capacity to show the physiological symptoms of aberrant cortical excitability (54). Therefore, EEG's usefulness as a brain signal detection technique in epilepsy research is still substantial. Although the underlying therapeutic mechanisms are still unclear, a recent study has verified that bidirectional brain-machine interfaces that can stimulate the brain have demonstrated effectiveness in improving seizure control in individuals with intractable epilepsy(55). It has been demonstrated that rather than merely suppressing seizures, systems such as responsive neurostimulation (RNS) promote seizure control by modulating the activity within epileptic networks over an extended period of time. This demonstrates how neuroplasticity may play a key role in how well epilepsy medications work. Additionally, research using non-human primates have confirmed the safety and efficacy of a new invention in the form of a wireless neural prosthesis (ECOGIW-16E), which has been shown to provide direct cortical stimulation (DCS) and prolonged electrocorticography (ECoG) recordings for up to six months(56). This device improves reliability. This tool improves seizure focus localization accuracy and creates new opportunities for BCI and closed-loop seizure management. Further demonstrating its considerable potential for effective neural signal analysis in BCI technology is a memristor-based neural signal analysis system which interprets signals in the analogue domain. This system achieved a high accuracy of 93.46% and a nearly 400fold increase in power efficiency over leading CMOS systems (57). Although these developments, there are still issues with using BCI to treat epilepsy. Crucial concerns include the precision of signal identification and decoding, the security and biocompatibility of long-term implants, and the adjustment of electrical stimulation or medication release parameters for improved therapeutic results. likewise, in the current research atmosphere, bridging the difference between the laboratory research and clinical practice continues to be an important challenge.
5.1.2 Spinal Cord Injury:
Damage to the structure or function of the spinal cord is known as spinal cord injury (SCI), and it usually happens as a result of diseases like myelitis or external forces like falls, vehicle crashes, or sports injuries(58). SCI occurs in 3.6 to 195.4 cases per million persons worldwide(59), and injuries can be categorised as either full or partial. Complete SCI causes an unconditional cessation of motor and sensory functioning below the site of injury by interfering with all neuronal communications within the spinal cord. On the other hand, incomplete SCI allows for some degree of sensory and motor function retention by maintaining some brain activity. BCIs are mostly used in the field of SCI rehabilitation to restore function in the upper and lower limbs (60,61). By managing gadgets like robotic arms or electrical stimulation systems, BCIs boost motor activity and neuroplasticity, the brain's ability to create new neural connections. The effectiveness of BCI in SCI rehabilitation has been confirmed by recent clinical research and case studies. Multimodal BCIs have been shown to improve lower limb mobility and reduce discomfort in SCI patients(58), whereas BCI-assisted motor imagery training dramatically increases upper limb functioning, especially in the early stages of treatment(62). Additionally, precise control of bionic limbs is made possible by sophisticated BCI systems that use implanted microelectrode arrays, improving operational flexibility and specificity. This demonstrates the useful advantages and efficacy of BCI technology in promoting patient independence and well-being, in addition to highlighting the potential of BCIs to enhance daily living and quality of life for SCI patients (63). Regarding advancements in the use of BCI for SCI rehabilitation, barriers such longterm integration problems, patient variability, and technological difficulties limit its widespread adoption. Although intracortical interfaces have made progress, there are still many obstacles because of their invasiveness, according to a review published in Nature Reviews Neuroscience (64). It is expected that future developments in algorithms and technology will increase the effectiveness of BCIs. The use of BCI in rehabilitation is set to grow dramatically as a result of advancements in creating minimally invasive systems, customising therapies to meet the needs of each patient, encouraging interdisciplinary collaborations, and integrating both augmented and virtual reality technology.
5.2 Mental and cognitive disorder:
Alzheimer’s Disease (AD):
The main symptoms of AD, a progressive neurological disease, include behavioral abnormalities, cognitive impairment, and memory loss. The frequency of AD is rising as the world's population ages, which has a significant effect on people, families, and social structures (65). The function of BCIs in treating mental and cognitive diseases is illustrated in Figure 4. Further more, a comprehensive summary of research studies examining the effectiveness of BCIs in the treatment and management of various illnesses may be found in Supplementary Table S2 (Supplemental Online Content 3, http://links.lww.com/JS9/D264). Initial examination, management of symptoms, medical care, and cognitive rehabilitation were the main areas of focus for studies regarding BCI technology in the treatment of AD. These studies use leading-edge technological techniques to improve patients' quality of life, slow the disease's course, and discover non-pharmacological therapy options. Early detection of AD is essential for commencing successful treatments and slowing the disease's progression. The traditional diagnostic methods typically identify the disease at a later stage, even though they primarily rely on neurological symptoms and neuroimaging. According to Dubois et al.(66), traditional diagnoses have several drawbacks, including delays, high biomarker variability, low imaging sensitivity, and outcomes that are influenced by a number of factors. By recording and examining data from electroencephalograms to detect early changes in neurological activity, BCI technology, on the other hand, makes early diagnosis more straightforward(67,68). For example, during cognitive tasks, anomalies in particular EEG frequency bands, such as theta and alpha waves, in AD patients may signal the onset of the disease early. It has been demonstrated by Prichep et al. (69) that measuring certain EEG features, particularly elevated theta power, can precisely foresee future dementia. This approach supports early detection and intervention techniques in AD by showing excellent sensitivity and specificity for identifying possible losses in healthy older adults. Moreover, new research has looked into the possibility of using ultra-weak photon emission from the hippocampus to noninvasively record the progression of AD. This suggests that minimally invasive BCI photon chips could be developed as novel tools for AD diagnosis and monitoring (70). The use of BCI technology in AD treatment and cognitive rehabilitation has attracted a lot of attention lately, especially because it improves patient quality of life and symptom control. By using neural modulation techniques, such as neurofeedback training, which modifies brain electrical activity, BCI can alleviate symptoms and improve mood while lowering anxiety and depressive symptoms. To improve the therapeutic results, BCI can also be combined with other treatment approaches like FES and Transcranial Magnetic Stimulation (TMS). According to research, BCI-driven neurofeedback training can improve memory and recall skills in AD patients while also stabilizing or boosting cognitive processes(71). A preliminary study examined the effectiveness of neurological training in improving reading and visual attention in individuals with moderate Alzheimer's disease, suggesting this strategy as a new avenue for non-pharmacological AD treatment (72). Moreover, in order to support fundamental communication and mental rehabilitation, a recent study suggested a BCI model for AD patients based on classical conditioning and brain state classification. This model correlates both "yes" and "no" ideas with emotional inputs. This study offers novel approaches and possible applications of BCI for cognitive rehabilitation (73).
5.3 Sensory Impairment:
Vision Disorder:
Any disorder that reduces a person's ability to process visual stimuli is referred to as impaired vision. This can impact various elements of a person's life, including their eyesight, visual field, sense of contrast, colored perception, and depth perception. Diminished visual acuity, visual field deficits, color vision abnormalities, decreased contrast sensitivity, and difficulties perceiving depth are some of the clinical symptoms linked to visual impairment. Applications like high-frequency SSVEP-based BCIs that combine with computer vision to enable the control of robotic arms for particular actions are the main focus to investigate into BCI technologies for those with visual impairments. Users can choose and handle things using BCI for automated tasks like holding and positioning through the system's ability to recognize and pinpoint objects within a work environment. These advanced control systems improve task performance's reliability and effectiveness while drastically reducing the user's requirements for operation(74). The use of BCI technology for treating visual problems is still primarily experimental at the moment.
6.ADVANTAGES AND DISADVANTAGES:
Since no program is flawless in every way, each one has advantages and disadvantages. Therefore, even while brain-computer interfaces are a fantastic way to improve direct communication between humans and machines, they do have certain drawbacks.
6.1 ADVANTAGES:
-This technology may eventually enable paralyzed individuals to manipulate prosthetic limbs using their thoughts.
-Assist individuals with disabilities in using their brain activity to operate wheelchairs or other devices.
-Improve the sensor system.
-Give a blind person the ability to sight by sending visual images into their brain.
-Send audio information to a deaf person's brain so they can hear.
-Permit players to manipulate video games with their thoughts.
-Permit a device to speak and display the ideas of a person who's mute.
-By using BCI in addition to telepresence, military officers can monitor any suspicious activity that may occur at the border.
-By identifying what is happening in the driver's head and making a choice in a couple of seconds, a car with BCI abilities may prevent any accidents from happening.
-BCIs can be used anywhere in the globe and are linguistically independent. For researchers and scientists across the globe, this has opened up novel possibilities.
6.2 DISADVANTAGES:
-The complexity of the brain is vast.
-The transmissions are susceptible to interference and are inadequate.
-Brain surgery can be dangerous and can result in brain death.
-BCI technologies are unable to detect certain chemical reactions that occur in the brain.
-The equipment is not as portable as it could be.
-The research is still in its early phases.
-The technology in use today is preliminary. Its growth may be hindered by ethical concerns.
-Very few signals from the brain can be detected by electrodes outside the skull.
-The brain develops scar tissues as a result of electrodes inserted inside the skull.
-BCI doesn't always produce precise findings, it can occasionally misinterpret the user's intentions.
-The user may experience significant physical and mental stress due to the extensive wiring needed.
-This computerized technology makes it possible for anyone to decipher your thoughts and violate your privacy.
7.The Future and Applications of Brain Machine Interface:
Because BCI technology can help persons who have lost or damaged their body parts restore their physical and mental power, it has drawn interest in the medical field. It enables persons with physical impairments to operate devices with their thoughts, enabling them to engage with the outside world independently. Industrial uses of BCI can be found in neurophysiological research, education, and mining(75-78). To create new applications and hasten the fourth industrial revolution, researchers must collaborate and update often.
7.1 Thoughts decoding:
Comprising a complicated organ, the brain generates and regulates our ideas and Physiological characteristics. Though brain-computer interfaces (BCI) may enhance performance in polygraphs, Current technology cannot precisely predict an individual’s thoughts. Researchers are Investigating how BCI might print actual documents, map imaginations into real items, Convert human thoughts into legible text, and extract wills from dying people’s Thoughts(79). Future BCI breakthroughs could involve people with physical limitations Driving and controlling machines remotely using their thoughts, and goods that Directly map human thoughts into tangible items. Advanced BCI technologies, However, could create privacy and security concerns that need global norms for Control(80,81).
7.2 Increasing the capacity of human memory:
The hypothesis of Stephen Hawking on uploading the human mind into a computer calls on issues regarding the possibilities of brain-computer interface (BCI) technology for memory extension(82). Recent advances reveal that brain signals can be obtained and transformed into data reflecting human activities(83,84). Though ethical standards must be observed, future research may investigate using BCI to gather behaviors and attributes for scientific and commercial uses. One could create portable flash drives or other physical memories to access brain data. Reaching this scientific aim calls for extensive multidisciplinary investigation.
7.3 Communication with telepathy:
A method currently in its early phases of research, telepathic communication can be enabled by BCI and computer-brain interface (CBI), Rao et al. showed(85,86). Future research might look at combining LOT and BCI networks to improve data flow. While keeping ethical standards, more research is required to investigate more possibilities and features (87-92).
7.4 Command and automation:
Particularly in home automation and control for physically challenged people, BCI technology is exciting for sectors of automation and control (93). It may also be employed in industrial manufacture as it develops, maybe over a safe wireless network (76,77). Still, more study is required to go over constraints and guarantee flawless interaction with smart sensors.
7.5 Sharing of intelligence:
Can the BCI and the CBI help to remodel the brain so enabling intelligence sharing among people? Though it sounds like fantasy, the basic ideas of the technology imply that brains might be artificially changed. But reaching this mark calls for strong knowledge of the nature and operation of human brains—a level not attained by present knowledge.
7.6 Harnessing brain energy:
With just 2% of the mass of the body, the human brain uses 20% of the total body energy budget to run its operations in an ordinary adult in a normal condition (94). With this energy-consuming ratio, this body organ ranks third in terms of energy hunger (95). We propose to harvest some of this vast amount of energy for running low-energy external devices by combining the BCI technology with other cutting-edge technologies. Researching how much energy a normal BCI system can gather from the brain will help to realize the concept.
7.7 Localized interface between the brain and computer:
Brain signal collection in Brain-Computer Interfaces (BCIs) is inherently non-selective. Whether electrodes are placed on the scalp (non-invasive) or beneath it (invasive), they detect all electrical impulses within their spatial range. As a result, BCIs collect large volumes of neural data and ambient noise, even when only a single function— such as controlling a prosthetic leg—is intended. This abundance of non-targeted data complicates signal processing and interpretation (96,97). However, by localizing the BCI system to specific brain regions responsible for targeted motor or cognitive functions, we can improve signal relevance. For example, in individuals with speech impairments, placing the BCI system over areas that process speech-related neural activity could yield cleaner, more specific signals (98). Such targeted localization not only enhances system performance but also allows for more compact and efficient BCI designs (2,97).
8.CONCLUSION:
The BMIs or Brain-Machine Interfaces mark a notable leap in technological advancement in the fields of neuroscience, artificial intelligence, and engineering. From helping individuals with paralysis regain mobility through robotic limbs controlled by the individual’s mind to other astonishing feats, BMIs have showcased their capability in improving human life. The venture has gone through a transformational journey, starting from old invasive systems that were difficult to use, to modern interfaces that are non-invasive, easy to use, and integrated with AI. Regardless of the advancements made, the practical use of BMIs faces some issues. Barriers to using this technology include low signal quality, differences in user performance, high costs of the system, and the extensive training that needs to be done before utilizing them. Moreover, privacy risks surrounding cognitive processes and mental control put need for proactive policy-making, with the need to establish so-called ‘neurorights’ that serve to guard users from surveillance. The further advancements of BMIs is expected to be achieved as new technologies roll out. New systems that will be more practical, easy to wear, and hybrid are bound to be able to incorporated into everyday life. Brain-to-brain communication stands to make significant changes along with augmented reality, and neural and digital therapy.
REFERENCES

Thillai Vaani Iyyanar*, Deshika Karunanithi, Kamal karunanithi, Senthil Kumar Krishnan, Kannabirran Vaikundam, From neurons to networks: A Review on Brain-Machine Interface Technologies, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 1034-1048. https://doi.org/10.5281/zenodo.16794166
 10.5281/zenodo.16794166
10.5281/zenodo.16794166
