
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Central India College of Pharmacy, Lonara, Nagpur 441111, Maharashtra, India
Gangrene is a serious and life threatening condition in which body tissues die due to poor blood flow, severe infection, or both. It is seen more often in people with diabetes, vascular diseases, or injuries that do not heal properly. This review highlights recent progress in the diagnosis and treatment of gangrene, with a special focus on regenerative therapies and digital health technologies. The article explains common warning signs, risk factors, and how gangrene typically develops. Newer diagnostic tools, such as artificial intelligence–based wound analysis, infrared thermal imaging, and smart wearable sensors, are helping doctors detect changes earlier and monitor wounds more accurately. Although standard treatment including antibiotics, wound care, surgical removal of dead tissue, and hyperbaric oxygen therapy continues to play a major role, modern research is opening exciting new possibilities. Regenerative approaches like stem cell therapy, platelet rich plasma (PRP), growth factor dressings, and nanotechnology-based materials show encouraging results in improving blood flow, speeding up healing, and reducing the chances of amputation. Herbal and plant-based compounds are also being explored for their anti-inflammatory and wound healing effects. Combined with digital tools, AI prediction models, and personalised treatment planning, these innovations may transform how gangrene is managed in the future. Overall, the review suggests that integrating traditional medical care with advanced technologies and regenerative medicine can greatly improve recovery, quality of life, and long-term outcomes for patients with gangrene.
Cell death in the body happens mainly in two ways: apoptosis and necrosis. Apoptosis is a natural and controlled process that removes damaged or old cells without harming nearby tissues. Necrosis, however, is uncontrolled and happens when cells die due to poor blood flow, serious infections, or injuries. This causes tissue damage and inflammation. Gangrene is the visible result of necrosis, occurring when a large area of tissue dies because of reduced blood supply and infection.¹?²
Gangrene, also called tissue death or mortification, happens when blood cannot reach certain body parts. Without oxygen and nutrients, tissues start to die. It can develop after injuries, infections, or in people with long term conditions like diabetes. If not treated promptly, gangrene can spread, leading to serious infections or even death.¹
One common cause is peripheral vascular disease (PVD), where blood flow to limbs, especially legs and feet, is reduced due to atherosclerosis (fatty deposits in arteries). Weak tissues are easily infected. Early treatment with antibiotics, wound care, and removal of dead tissue can often save the affected area. Delayed care may require amputation. Gangrene can be dry, wet, or gas gangrene. Dry develops slowly due to poor circulation, wet occurs with infection, and gas spreads rapidly with gas formation in tissues.³
Recent advances in AI technology are helping doctors detect gangrene earlier. AI can analyze images of wounds and predict tissue damage faster than traditional methods. New devices using infrared scanning, thermal imaging, and smart sensors can detect poor blood flow before gangrene becomes severe.³ Additionally, herbal treatments like turmeric, neem, and aloe vera show promise in supporting wound healing and reducing infection. These natural remedies, alongside modern medicine, may improve recovery and prevent complications.
In India, gangrene affects around 5% of the population, mainly between 20 and 40 years, highlighting a major health concern. Combining early detection, AI technology, modern treatment, and supportive herbal care can help doctors manage gangrene more effectively and improve patient outcomes.²
MATERIALS AND METHODS:
A structured literature review was performed in PubMed, Scopus, and Google Scholar databases between 2010 and 2025 using the keywords Gangrene, Ischemia, Necrosis, Regenerative Medicine, Artificial Intelligence, and Wound Healing. Articles were limited to English language human studies, reviews, and clinical trials. Case reports, non-peer reviewed materials, and purely experimental animal studies were excluded. Data were qualitatively synthesised under thematic categories including epidemiology, diagnosis, therapeutic strategies, and technological innovations.
EPIDEMIOLOGY AND RISK FACTORS
Gangrene is a dangerous problem that occurs when body tissues die because of a lack of blood flow or an infection.² It affects millions of people all over the world and can cause serious illness or even death if not treated in time. The global distribution and risk factors related to gangrene are illustrated in Figure 1. Globally, more than 200 million people have peripheral artery disease (PAD), and about 10% of them develop a severe form called critical limb ischemia, which can lead to gangrene. People with mild PAD or leg pain while walking (known as intermittent claudication) also have a 5–10% chance of developing serious blood flow problems within five years.???
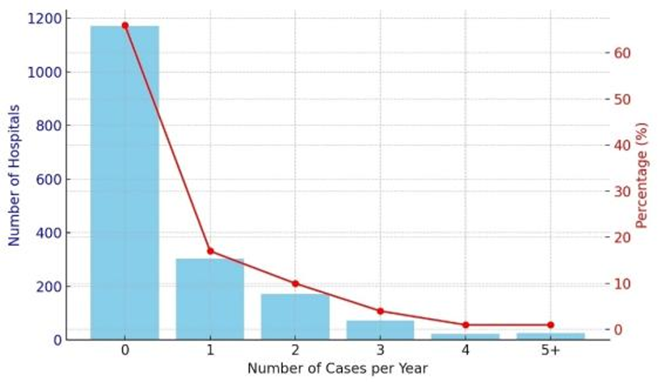
Figure 1: Epidemiology of gangrene across different regions.
The figure presents reconstructed data illustrating the prevalence of gangrene based on global reports. Data and concept adapted from [4].
Clostridial gas gangrene, although rare, is one of the most dangerous types because it spreads fast and has a very high death rate. It often happens after trauma, surgery with contaminated instruments, or sometimes without any clear cause.² People with weak immune systems, those who use intravenous drugs, take blood thinners, or have cancer are more likely to develop it. Older adults usually have infections caused by many bacteria together, while younger patients often get it from a single germ like Staphylococcus or Streptococcus.?
Environmental exposure also plays a role since Clostridium spores are found widely in soil, making injuries in such areas risky. Natural disasters and road accidents can increase cases of gangrene. In Europe, outbreaks among drug users have shown very high death rates.? Some medicines, such as SGLT2 inhibitors used for diabetes, have also been linked to rare cases of gangrene.²??
In the United States, critical limb ischemia affects about 1% of people over 50 years old. In India, growing cases of diabetes, obesity, and vascular disease increase the risk, especially in rural areas where early medical care is limited. Poor wound care and late diagnosis make the problem worse.²??
ETIOPATHOGENESIS AND CLINICAL TYPES
Aetiology
Gangrene happens when parts of the body die because they don’t get enough blood, get infected, or are injured. Usually, more than one factor is involved. The main cause is poor blood flow, which is common in people with blocked arteries, diabetes, or other blood vessel problems. Infections make it worse because dead tissue lets bacteria and fungi grow easily.? Certain bacteria, like Clostridium perfringens and C. septicum, can cause fast spreading gas gangrene. Fournier gangrene is a serious infection in the genital and perineal area, often coming from skin or urinary infections. Injuries, burns, cuts, pressure sores, surgeries, or small wounds in diabetics can also lead to gangrene. Rarely, injuries to the penis in children or adults may cause it.²
Pathophysiology of Gangrene
Gangrene is a fast spreading infection that destroys muscles and soft tissues. Most cases are caused by bacteria called Clostridium, especially C. perfringens, which is responsible for about 80 to 90% of cases.¹ Other species like C. septicum and C. histolyticum can also cause it. These bacteria are found in soil, dust, and in the gut or genital areas of humans. Not every wound gets infected; it depends on factors like immunity, diabetes, nutrition, and how deep or damaged the wound is.? The detailed mechanism of infection, toxin release, and tissue damage is illustrated in Figure 2.
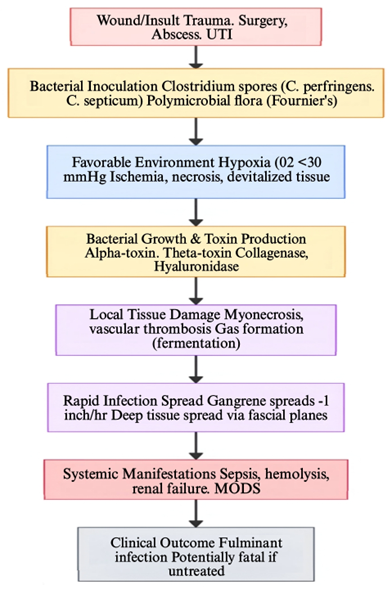
Figure 2: Pathophysiology of gangrene.
This schematic illustrates how reduced blood flow, infection, and tissue necrosis interact to cause gangrene.
In areas with low oxygen, the bacteria grow quickly. C. perfringens releases toxins, such as alpha toxin, that destroy cells, blood vessels, and tissue, while other enzymes help it spread rapidly. Gas is produced during bacterial growth, leading to the characteristic crackling under the skin. Fournier gangrene affects the genital area and involves multiple bacteria working together, often after a urinary infection, abscess, or minor injury.² Non-Clostridial bacteria like E. coli and Klebsiella also contribute to the condition. The toxins can enter the blood, causing sepsis and organ failure.¹
Types of Gangrene
Gangrene is mainly divided into dry, wet, and gas gangrene, each with different causes and seriousness.
Dry Gangrene happens when blood flow is very poor, usually in fingers or toes. Lack of oxygen makes tissue die and dry out. It often occurs in people with diabetes, blocked arteries, high cholesterol, or long term smoking. The affected area turns dark, shrivelled, and clearly separated from healthy tissue. If it lasts long, the dead part may fall off naturally. Early on, infection is usually low, but it can turn into wet gangrene if bacteria invade.? The typical appearance of dry gangrene is shown in Figure 3

Figure 3: Clinical presentation of gangrene.
Wet Gangrene occurs when dead tissue gets infected by bacteria. It spreads fast, causing swollen, smelly, and discoloured tissue, sometimes with blisters. It is dangerous because bacteria and toxins can enter the blood, leading to sepsis. Diabetes, severe artery disease, and kidney problems increase the risk.??? An example of wet gangrene is illustrated in Figure 4.

Figure 4: Clinical presentation of wet gangrene.
Gas Gangrene is a severe type of wet gangrene, mostly caused by Clostridium perfringens. It can follow a wound (traumatic) or come from inside the body in sick or diabetic patients (non-traumatic). Gas forms in tissue, causing crackling under the skin, and it spreads very fast, often needing urgent treatment.? The characteristic findings of gas gangrene are depicted in Figure 5.

Figure 5: Clinical features of gas gangrene.
The image highlights tissue necrosis, edema, and crepitus caused by gas producing bacteria. Reproduced from Tsutsumi Y.? Licensed under Creative Commons Attribution (CC BY 3.0).
CLINICAL PRESENTATION AND DIAGNOSIS
Gangrene, including Fournier gangrene, presents with clinical signs that reflect tissue ischemia and infection. The earliest symptom is severe pain, often throbbing or burning, which may worsen with movement, particularly in patients with peripheral vascular disease (PVD). Pallor of the affected area, especially when elevated, indicates reduced blood flow, and the tissue may feel cool to the touch due to impaired perfusion.???
Loss of sensation is common, particularly in patients with diabetic neuropathy, which can mask pain and delay recognition. As gangrene progresses, ulceration develops, usually over bony prominences, and a gangrenous odour may arise from necrotic tissue colonised by bacteria, signalling advanced infection. Early recognition of these features is crucial, as prompt surgical intervention can prevent rapid progression and systemic complications.? The key clinical and diagnostic findings of gangrene are summarised in Table 1.
Table 1: Conventional and emerging diagnostic methods for gangrene – findings and clinical utility
|
Sr. No |
Diagnostic method |
Findings |
Clinical Utility |
References |
|
1 |
AI-assisted Imaging & Predictive Models |
Detects early tissue changes in images (photos, infrared, MRI, CT) and predicts progression of gangrene |
Enables earlier and more accurate diagnosis, helps clinicians prioritize treatment, monitors wound healing trends, and reduces reliance on subjective assessment |
3 |
|
2 |
Laboratory Test |
Leukocytosis, elevated CRP/procalcitonin |
Confirms infection/sepsis: guides management |
9 |
|
3 |
Ultrasound |
Subcutaneous gas. Edema. Fascial thickening. Cobblestoning |
Rapid bedside detection of early necrosis |
9 |
|
4 |
X-ray |
Subcutaneous gas |
Quick detection: absence does not rule out disease |
9 |
|
5 |
CT scan |
Fascial thickening. Fat stranding, gas, abscesses, fluid collections |
Most sensitive and specific: assesses extent/source |
2 |
|
6 |
MRI |
Soft tissue edema, gas on gradient-echo. T2 high signal |
High resolution soft tissue imaging: limited by cost/time |
9 |
|
7 |
Doppler/Ankle brachial index |
Reduced blood flow. Arterial occlusion |
Evaluates vascular status, important in PVD |
9 |
TREATMENT AND MANAGEMENT OF GANGRENE
Gangrene management requires an integrated approach involving pharmacological, non-pharmacological, and emerging interventions. The primary goals are infection control, restoration of perfusion, tissue preservation, and prevention of systemic complications.
Pharmacological Management
The main goal of drug treatment in gangrene is to stop infection, control pain, improve blood flow, and prevent the disease from spreading to other parts of the body. Starting the right medicines early can help reduce complications and increase the chance of saving the affected tissue.¹¹
In cases of wet or gas gangrene, strong antibiotics are started right away to fight both oxygen loving (aerobic) and oxygen free (anaerobic) bacteria. Doctors often begin with broad medicines like piperacillin tazobactam or carbapenems (such as imipenem or meropenem) that work against many types of germs. If the infection is caused by Clostridium perfringens, high doses of penicillin G or clindamycin are used since they can block toxin effects. Once lab tests show the exact bacteria, the antibiotics are changed to match. Using a mix of antibiotics usually gives better results, especially in diabetic or poor blood flow cases where several germs are present.¹??¹¹
Gangrene often causes strong pain and swelling because of tissue death and infection. Painkillers like NSAIDs or opioids are used to relieve the pain. But NSAIDs should be used carefully if the person has kidney or blood vessel problems. Sometimes, doctors may give a short course of steroids to reduce inflammation, but these are avoided if the infection is still active.¹¹
Medicines that help improve blood flow can be helpful, especially in dry gangrene caused by poor circulation. Drugs like heparin or low molecular weight heparin stop blood clots and improve flow in small blood vessels. Vasodilators such as pentoxifylline or alprostadil can also help bring more oxygen to the tissues and reduce pain from poor blood supply, though their success varies among patients.¹²
Some additional medicines can help recovery. Antioxidants like vitamin E and alpha lipoic acid may support healing, and creams with silver sulfadiazine or iodine help prevent wound infection. Drugs that improve oxygen delivery to tissues can also be used along with hyperbaric oxygen therapy for better healing.¹³
Non-Pharmacological Management
Non drug treatment plays an important role in managing gangrene and works together with medicines to help recovery. These methods mainly focus on improving blood flow, removing dead tissue, stopping infection, and helping wounds heal properly. A combined effort from surgeons, infection doctors, and wound care teams gives better results for the patient.
Surgery is important in treating gangrene. The main procedure is called debridement. This involves carefully removing dead or infected tissue to stop the infection from spreading and to allow healthy tissue to grow. In severe cases, amputation might be necessary to save the patient’s life and prevent the infection from entering the bloodstream. If gangrene occurs due to poor blood flow, procedures like angioplasty, bypass grafting, or stent insertion can help restore circulation and promote healing. Getting surgical care early greatly lowers the chance of losing a limb.²
Proper wound care is very important for healing and preventing new infections. Dressings that keep the wound slightly moist such as hydrogel, hydrocolloid, or honey based dressings can help new skin grow faster. A special method called negative pressure wound therapy (vacuum assisted closure) helps remove extra fluid, reduce swelling, and increase blood flow around the wound. Cleaning the wound regularly and changing dressings under clean conditions are necessary steps for good recovery.¹¹
In HBOT, the patient breathes pure oxygen inside a chamber with increased air pressure. This process helps more oxygen reach the affected tissues, slows the growth of infection causing bacteria, and promotes the repair of damaged areas. When used together with surgery and antibiotic treatment, HBOT has been found to improve healing and lower the risk of losing a limb.²
Healthy habits play a strong role in both preventing and treating gangrene. People with diabetes should control their blood sugar levels carefully. Quitting smoking, eating a balanced diet, and doing light exercise or physiotherapy can help improve blood flow and speed up healing. Patients should also learn proper foot and skin care and report any small cuts or sores early to avoid serious infection or tissue damage.¹?
Novel and Adjunctive Therapies
Even with progress in standard treatments, gangrene still causes high illness and death rates. New and supportive therapies are being explored to improve healing, stop infection, and repair damaged tissue. These modern approaches integrate ideas from biotechnology, artificial intelligence, and traditional medicine to develop more comprehensive and effective treatment plans.
Natural and herbal medicines are getting more attention for their helpful effects in gangrene care. Many plants have antibacterial, antioxidant, and blood flow–improving properties. For example, curcumin (from turmeric) helps reduce swelling and supports wound healing by controlling inflammation and fighting harmful oxygen molecules. Aloe vera helps the skin repair itself by increasing new cell and collagen growth. Neem and turmeric have strong germ killing effects against bacteria that cause gangrene. Plant chemicals like flavonoids and polyphenols also help improve blood flow and oxygen to tissues. While human studies are still limited, early research suggests these natural remedies may help wounds heal faster when used with regular treatment.¹?
New treatments in regenerative medicine aim to repair damaged tissues and improve blood supply. Stem cell therapy, especially using mesenchymal stem cells (MSCs), helps grow new blood vessels and supports tissue healing by releasing helpful growth factors like VEGF and TGF-β. Platelet rich plasma (PRP) therapy uses a patient’s own platelets, which contain substances that promote healing and help close wounds. These treatments look very promising for diabetic and poor circulation–related gangrene, but more studies and standard treatment methods are still needed before they become common.¹?
Artificial intelligence (AI) is playing a growing role in finding and managing gangrene early. Machine learning tools can study wound pictures and tell the difference between healthy and dead tissue with good accuracy. AI can also help doctors choose the right antibiotics, predict how bad an infection might get, and follow the healing process through digital wound tracking. Deep learning systems and mobile health apps can even help diagnose wounds remotely, which is especially useful in areas with fewer medical facilities. Using AI in treatment helps doctors make faster and more accurate decisions.³ An overview of AI and machine learning approaches for gangrene detection and management is illustrated in Figure 6.
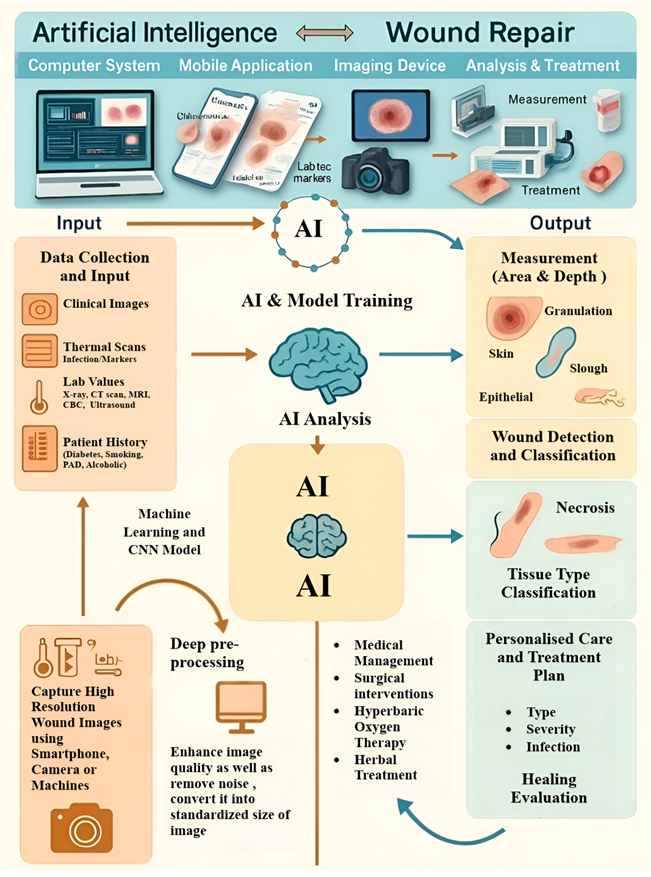
Figure 6: Artificial intelligence–assisted detection of gangrene wounds.
The image illustrates a machine learning model analyzing wound images to detect early tissue necrosis and predict disease progression.
Nanotechnology offers new ways to treat gangrene more effectively. Nanoparticle based dressings that include silver, zinc oxide, or herbal extracts can fight bacteria and help new tissue grow at the same time. Hydrogel materials mixed with nanoparticles or growth factors create a healthy environment for wound healing and controlled medicine release. These new materials could make long term wound care safer and more effective by speeding up healing and reducing side effects from medicines.¹? A summary of pharmacological, non-pharmacological, and emerging treatment strategies for gangrene is presented in Table 2.
Table1: Conventional and Emerging Treatment Modalities for Gangrene: Mechanisms and Clinical Utility
|
Pharmacological Management of Gangrene – Mechanisms and Clinical role |
||||
|
Drug class |
Examples |
Mechanisms |
Clinical role |
References |
|
Antibiotics |
Piperacillin Tazobactam, Clindamycin |
Inhibit Bacterial growth and toxin production |
First line infection control |
10,11 |
|
Analgesic/ NSAID’s |
Ibuprofen, Morphine |
Pain and inflammation reduction |
Symptomatic relief |
11 |
|
Anticoagulant/ Vasodilators |
Heparin, Alprostadil |
Prevent microcirculation, prevent clot forming |
Adjunct for ischemic limbs |
12 |
|
Antioxidant/ Topical agent |
Vitamin E, Silver Sulfadiazine |
Enhance wound healing, control local infection |
Supportive therapy |
13 |
|
Non-pharmacological management of Gangrene – interventions and clinical utility |
||||
|
Interventions |
Mechanisms |
Clinical utility |
Reference |
|
|
Debridement/ Amputation |
Removal of necrotic tissue and infection source |
Prevents spread and promotes healing |
2 |
|
|
Revascularization/ (Bypass, Angioplasty) |
Restores arterial blood flow |
Enhances tissue oxygenation |
11 |
|
|
Wound dressing/NPWT |
Maintains moisture, removes exudate |
Accelerates wound healing |
11 |
|
|
Hyperbaric Oxygen Therapy |
Increases oxygen delivery to ischemic tissues |
Reduces infection, improves recovery |
2 |
|
|
Lifestyle modification |
Glycemic control, smoking cessation, nutrition |
Prevents recurrence, enhances outcomes |
14 |
|
|
Emerging and Adjunctive Therapies for Gangrene – Mechanism and Clinical Potential |
||||
|
Therapy |
Mechanism |
Clinical benefits |
References |
|
|
Herbal Compounds (Curcumin. Neem, Aloe vera) |
Anti-inflammatory. Antimicrobial, wound healing |
Enhances tissue repair |
14 |
|
|
Stem Cell Therapy / PRP |
Promotes angiogenesis and regeneration |
Restores perfusion and healing |
15 |
|
|
Artificial Intelligence |
Image based diagnosis, wound monitoring |
Early detection, precision management |
3 |
|
|
Nanotechnology Based Dressings |
Targeted antimicrobial delivery |
Reduces infection. Accelerates healing |
16 |
|
IMPACT OF COMORBIDITIES IN PROGNOSIS
The outcome of gangrene largely depends on other health problems a person may have. Diabetes is one of the biggest factors that make recovery harder. It slows down wound healing, reduces blood flow in small vessels, and weakens the immune system. People with diabetes are more likely to get repeated infections and often need larger or multiple amputations compared to those without diabetes.¹? Peripheral artery disease (PAD) and atherosclerosis also make things worse by reducing blood supply to tissues, causing them to die. In these cases, procedures like angioplasty or bypass surgery play a crucial role in whether the limb can be saved and the patient survives.¹??¹? An overview of the impact of common comorbidities on gangrene prognosis is illustrated in Figure 7.
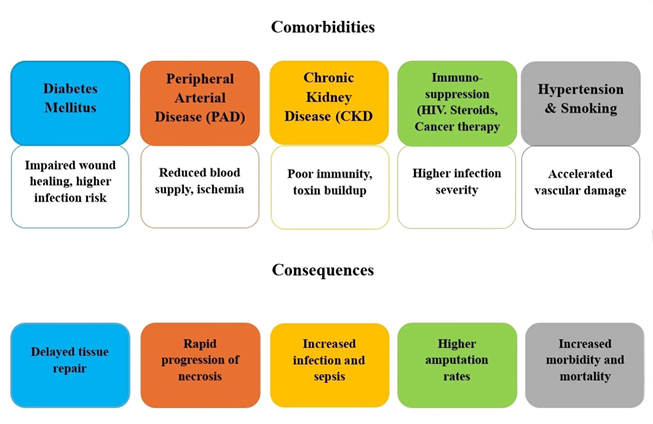
Figure 7: Impact of comorbid conditions on gangrene outcomes.
The diagram demonstrates how conditions such as diabetes, peripheral vascular disease, and immune deficiencies can worsen disease prognosis.
Chronic kidney disease (CKD) can also worsen outcomes. Poor blood vessel health, toxin buildup, and weak immunity increase tissue damage and complications. Rare cases like penile gangrene in dialysis patients show how severe CKD related problems can be. Obesity can indirectly make recovery harder by reducing local blood flow, raising infection risk, and making surgery more difficult. For gangrene caused by infections, such as gas gangrene, quick recognition and prompt surgical removal of dead tissue are vital. Delays increase the risk of serious infections and death. Antibiotics and proper wound care are also crucial.¹?
In general, recovery depends on how much tissue is affected, how fast treatment starts, and how well infections are controlled. Saving the limb is always the goal, but sometimes major amputation is necessary. Advances in surgery, prosthetics, and coordinated care have improved quality of life, but early detection and managing other health problems remain key to better outcomes.¹?
PREVENTION AND EARLY DETECTION OF GANGRENE
GUIDELINES AND RECOMMENDATIONS
National Treatment Protocols and Preventive Screening (India)
In India, management of gangrene is guided by recommendations from the Indian Council of Medical Research (ICMR) and the National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS). Clinical evaluation supported by Doppler studies is essential for early detection. In cases where tissue is unsalvageable, surgical debridement or amputation is indicated. Broad spectrum empiric antibiotics such as piperacillin tazobactam or meropenem are recommended initially, with modification based on microbiological culture. Glycaemic control in diabetic patients is strongly emphasised, while hyperbaric oxygen therapy is used selectively. Preventive strategies under NPCDCS include routine foot examinations, monofilament testing, and ankle brachial index measurements in high risk populations, particularly diabetics.²??²¹
International Treatment Protocols and Preventive Screening
Globally, the Infectious Diseases Society of America (IDSA) and the Centres for Disease Control and Prevention (CDC) recommend urgent surgical consultation in suspected necrotising infections, combined with empiric antibiotic therapy using carbapenems or beta-lactam/beta-lactamase inhibitor combinations with clindamycin and vancomycin. Hemodynamic support in intensive care is crucial in septic patients, and hyperbaric oxygen therapy can be used as an adjunct.
According to the European Society of Cardiology (ESC) and the National Institute for Health and Care Excellence (NICE), procedures such as angioplasty or bypass are recommended for patients with ischemic dry gangrene, aiming primarily to preserve the limb rather than resort to amputation. International guidelines also highlight the importance of preventive care, including annual thorough foot examinations, educating patients on daily self-inspection of their feet (ADA), establishing multidisciplinary diabetic foot clinics, and implementing population wide screening programmes for peripheral arterial disease, diabetes, and hypertension (WHO, ADA, ESC).²²
SOCIOECONOMIC AND PUBLIC HEALTH IMPACT
Diabetic foot ulcers (DFUs) are more common among Black and Hispanic people compared to White individuals. This happens because many people from these groups face challenges like low income, less education, and not having good health insurance.²³ These problems make it harder to get regular check ups or see specialists on time. As a result, many people visit doctors only when the ulcers are already serious, which often leads to hospital stays or even amputations. Social issues such as living in poorer areas, fewer job opportunities, and unfair healthcare systems also make the situation worse, showing how deeply inequality affects health.²?
Where a person lives also makes a big difference. Amputation rates vary from place to place, often because some areas don’t have enough medical facilities or trained doctors. People in rural or low income regions usually have to travel far to get help, so they may wait longer before getting treated, leading to more severe outcomes.²³
These ulcers also put a big strain on both families and the healthcare system. Treating foot complications costs a lot more than regular diabetes care and often requires hospital visits, emergency care, and home treatments. Severe cases can cost tens of thousands of dollars, and people may also lose income or be unable to work. To fix this problem, everyone needs fair access to early treatment, proper foot care, and complete medical support from a team of healthcare professionals.²?
FUTURE PERSPECTIVE
In the future, the management of gangrene will likely improve with better awareness, early diagnosis, and new treatment options. One major focus will be on finding gangrene at an early stage before tissue death becomes severe. This can happen with the help of simple screening tools and mobile health technology that allow quick detection, especially for people with diabetes or poor blood flow. Education and community programs will also play a big role in teaching people how to notice early warning signs and care for wounds properly.²??²?
Medical treatment for gangrene will continue to grow with the use of advanced wound care, natural medicines, and better infection control.²? Scientists are also studying how stem cells and tissue engineering can help repair damaged tissues and improve blood flow to affected areas. These new methods may reduce the need for amputation in the future.²³
In addition, better public health policies and access to healthcare will help prevent gangrene, especially in low income and rural areas where people often reach hospitals too late. Affordable healthcare, better diabetes control, and good hygiene practices will make a big difference.²??²?
Overall, the future looks positive if technology, education, and healthcare systems work together. By combining prevention, early detection, and modern treatment, many lives and limbs can be saved from gangrene. The main goal for the coming years will be to reduce the number of cases and make sure every person gets the right care at the right time, no matter where they live.²³?²??²?
CONCLUSION
Gangrene is a serious issue that can lead to major health problems, such as infections, loss of a limb, or even death. However, if detected early and treated correctly, the outcomes improve significantly. People with diabetes, poor blood circulation, or weak immune systems are at higher risk for gangrene, so they should have regular check-ups. Doctors can identify it early through physical exams, lab tests, scans, and new AI tools that can spot damaged tissue more quickly. Treatment typically involves antibiotics, cleaning or removing dead tissue, caring for wounds, and sometimes using oxygen therapy at high pressure. New methods like stem cells, platelet rich plasma, herbal medicines, and special dressings made with nanomaterials are promising for helping wounds heal and preventing amputations. Managing other health issues, maintaining healthy habits, and recognising warning signs early are also crucial. Improved awareness, education, and better access to medical care, especially in rural or low income areas, can help to avoid serious cases. Combining early detection, proper treatment, and knowledge can save lives and limbs.
ACKNOWLEDGMENT
The author gratefully acknowledges the support of Central India College of Pharmacy and its faculty members for providing guidance and resources during the preparation of this review. Appreciation is also extended to family and colleagues for their encouragement. This manuscript has been submitted to the International Journal of Pharmaceutical Sciences.
REFERENCES






Faraz Pathan, Rubina Sheikh, Ayesha Siddiqua, Ashna Khan, Sana Malik, Prerona Das, Gangrene: Early Detection, Emerging Therapies, and The Role of Artificial Intelligence, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 2329-2343. https://doi.org/10.5281/zenodo.17922427
 10.5281/zenodo.17922427
10.5281/zenodo.17922427