
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Yash Institute of Pharmacy, Chh. Sambhajinagar, Maharashtra, India 431134
Gene therapy works by changing the person’s material to treat or prevent disease. I see gene therapy as a way to fix the problems caused by errors. Gene therapy adds the new genes, swaps out the genes or turns off the genes. Gene therapy delivers the material into the target cells using vectors—most often modified viruses. In my view Gene therapy can be given in two ways. In vivo Gene therapy delivers the genes into the body. Ex vivo, Gene therapy changes the cells, outside the body. Then puts the cells back. Gene therapy began in the 1980s. I have watched gene therapy grow from an idea to a tool that can help people with illnesses. Gene therapy has shown promise for the diseases that affect us. Gene therapy can treat the inherited disorders such, as hemophilia and cystic fibrosis. Gene therapy can also target the conditions such, as cancer, diabetes and HIV/AIDS. Early successes came in the 1990s when gene therapy treated deficiencies. Gene therapy uses vector systems to move genes into cells. Gene therapy often uses adenovirus-based vectors to achieve gene transfer. Gene therapy now includes a range of approaches that aim to fix genes in the body. The basic idea of gene therapy is to fix mutations that cause disease. Gene therapy does this by inserting a gene correcting a gene repressing a gene or by destroying cells. I see that the modern tools, like RNA interference and CRISPR/Cas9 let gene therapy edit genes precisely. In cancer treatment gene therapy tries to hit tumors boost the response and keep cells safe during chemotherapy. Despite challenges related to safety, delivery efficiency, and ethical concerns—particularly regarding germline modifications—advances in gene-editing technologies have significantly improved precision and safety, expanding future therapeutic possibilities.
Gene remedy is a scientific method that treats or prevents sickness by changing someone’s genes.
How it works:
Gene remedy can replace a faulty gene with a healthy copy, or inactivate a disease-causing gene. It can also introduce a new gene into cells to help combat disease [1,2].
How it is delivered:
Genetic material is delivered to cells using a vector, which is usually a virus. The virus is modified to remove any disease-causing elements so that it can enter cells without making the patient sick.
How it is administered:
There are two main methods to administer gene therapy:
What it can treat:
Gene therapy can address a wide range of illnesses, including cancer, cystic fibrosis, heart disease, diabetes, hemophilia, and AIDS.
Availability:
The U.S. Food and Drug Administration (FDA) has approved gene therapy products for several conditions. However, for most individuals, gene therapy is only available as part of a clinical trial [5].
Gene therapy includes using genes to treat or prevent a variety of conditions. This is particularly relevant for haematological diseases like hemophilia and sickle cell anemia, and cancers such as acute lymphoblastic leukemia (ALL). In muscular conditions, such as spinal muscular atrophy (SMA), the introduction of nucleic acids into cells using a vector aims to change gene expression to prevent, halt, or reverse a pathological condition. This also applies to metabolic diseases like mucopolysaccharidoses (MPS IIIA) and monogenic diseases like cystic fibrosis and alpha-1-antitrypsin deficiency [6].
Gene therapy has been a complex topic for decades, ever since its first conceptualization in the 1980s. Although the concept is not new, it evolved rapidly until the early 1990s, when a significant milestone was achieved. Two young girls with adenosine deaminase severe combined immunodeficiency (ADA-SCID) successfully underwent gene transfer. Since then, innovations in therapy techniques and opportunities have expanded, covering not only common diseases such as cancer and inherited lipid disorders but also rare conditions like limb ischemia. As of now, nearly 2,600 gene therapy clinical trials have been either completed or are still in progress worldwide, encompassing a wide range of conditions, including immunodeficiency disorders [7].
Other virus-based gene transfer technologies are also in use and rely on recombinant versions of certain viruses, including adenovirus, adeno-associated virus (AAV), herpesvirus, vaccinia virus, poliovirus, sindbis, and RNA viruses. To date, adenoviral systems have seen the most extensive application in clinical settings. Adenoviral gene delivery systems are based on the discovery that adenovirus genomes with deletions in the E1 region can be propagated in cells that express the E1 genes. Subsequently, it was demonstrated that replication-defective adenovirus genomes containing foreign DNA sequences could be replicated in cells where E1 proteins are provided in trans, leading to the use of these vectors in gene therapy applications [8].
PRINCIPLE OF GENE THERAPY
The idea in the back of gene therapy is instead straightforward, where the concept of disease arising from some of mutation happening on the molecular level or the gene itself, can consequently be corrected through changing the mutation to either prevent or deal with sicknesses. The forms of 'Faults' or mutations which could motive a ailment variety from either deletion, addition or many different as as an example gene deletion in alpha thalassemia [9].
HISTORY OF GENE THERAPY
|
Decade |
Event |
|
1960-1970 |
First direct integration of functional DNA into a human. |
|
|
First proof that a virus can deliver functional genes. |
|
|
Adding foreign genes to cultured cells from patients with Lesch-Nyhan syndrome corrects genetic defects. |
|
1970-1980 |
First failure of gene therapy in three young sisters from West Germany. |
|
|
Gene therapy proposed as a cure for genetic disorders for the first time. |
|
|
Beta-thalassemia gene successfully inserted into the bone marrow of irradiated mice. |
|
1980-1990 |
Microinjection of purified DNA into mouse embryos triggered genetic transformation. |
|
|
First experiment to test the feasibility of gene targeting in the human genome. |
|
|
First retroviral vector suitable for gene therapy created. |
|
|
NIH released first draft guidelines for human somatic cell gene therapy experiments. |
|
|
First stable human antitumor cytotoxic T-cell clones isolated and maintained in culture. |
|
1990-2000 |
First human test demonstrated the safety of a retroviral vector for gene therapy. |
|
|
Successful gene therapy treatment for Ashanti DeSilva for severe combined immunodeficiency caused by a faulty ADA gene. |
|
|
FDA released gene therapy regulations. |
|
|
AdSTK109 vector with the complete human alpha1-antitrypsin genomic DNA locus demonstrated sustained expression in mice. |
|
|
Death of Jesse Gelsinger, the first patient to die in a gene therapy trial. |
|
2000-2010 |
Two SCID-affected French boys reported to be cured by gene therapy. |
|
|
Gene therapy trials for SCID children in France and the United States suspended. |
|
|
Term CRISPR-Cas9 published for the first time. |
|
|
Discovery of induced pluripotent stem cells (iPSCs). |
|
|
Small trial released showing the feasibility of gene therapy to treat hereditary retinal disease. |
|
|
Virtually blind infant with a rare genetic eye condition regains normal vision following gene therapy; stem-cell transplantation shown to be a promising cure for HIV. |
|
2010-2020 |
Successful treatment of beta-thalassemia with gene therapy. |
|
|
Neovasculgen, a gene-therapy drug for the treatment of peripheral artery disease, critical limb ischemia, approved in Russia. |
|
|
Adoptive cell therapy used for the first time on a child with leukemia (CART therapy). |
|
|
Five ADA-SCID children successfully treated with gene therapy. |
|
|
Adeno-associated virus with a clone of REPI used to treat choroideremia patients |
|
|
First oncology gene therapy approved in the United States and Europe |
|
|
CRISPR improves muscle function in a mouse model of Duchenne muscular dystrophy |
|
|
First clinical trial using CRISPR/Cas 9 to treat patients |
|
|
Second patient confirmed HIV-free after stem-cell therapy |
|
|
Nobel Prize in Chemistry awarded for developing CRISPR genome editing |
|
|
Gene therapy restores immunological function in children with rare immunodeficiency |
POTENTIAL APPROACHES FOR GENE THERAPY
In order to alter a cell at a molecular level, there are several methods that can be executed. One technique is corrective gene therapy wherein a mutated non-functional gene that causes diseases is changed by using a healthy reproduction of the gene. This method is typically suitable for dominant issues and is especially useful when the faulty gene produces a disease-causing protein or an interfering substance [11].
Gene augmentation therapy is another method which involves the addition of a normal gene to replace the function of a faulty gene. Here, the faulty gene is not replaced. This approach is not useful when the faulty gene produces a diseasecausing protein. Inactivating or knocking out a mutated gene that is functioning improperly is also an option.
Introducing a new gene into the body to assist in fighting a disease, repairing the abnormal gene to restore its normal function, and modifying the regulation (the degree to which a gene is turned off or on) of a particular gene are also other strategies [12].
TYPE OF GENE THERAPY: [Therapeutic Gene Trials]
Gene therapy to fight cancer falls into three preferred categories:
Most of the therapeutic trials for cancer currently underway involve introducing one of several cytokine genes into either tumor cells or autologous fibroblasts. The purpose of these trials is that, once reintroduced, these genetically modified cells will act as sites of cytokine production, enhancing immunity through various mechanisms (depending on the cytokine chosen).
Another method to boost immunity against tumor cells through gene therapy is to increase the antigenicity of tumor cells. This technique, explored by Nobel and colleagues, involves introducing the HLA-B7 gene into malignant melanomas using either retroviral vectors or DNA/liposome complexes. Tumor cells expressing the foreign HLA molecule can trigger an active allogeneic immune response at the tumor site, leading to a coincidental immune reaction to specific tumor antigens expressed by the malignant cells [15].
A third approach currently being used in clinical settings is the introduction of suicide genes directly into tumors; the gene of interest is the herpes simplex virus thymidine kinase (HSV-TK) gene. Expression of this gene makes cells vulnerable to being killed by ganciclovir. This drug is safe for non-modified human cells but destroys cells carrying the HSV-TK gene by converting the enzyme into nucleotide-like precursors that inhibit DNA synthesis. Retroviruses, which selectively transduce dividing cells, can preferentially deliver the HSV-TK gene to tumor masses via stereotaxic injection of retroviral supernatant to dividing cells in the brain, which may originate from the tumor. Patients are then treated with ganciclovir to selectively remove HSV-TK-expressing tumor cells [16].
Interestingly, experiments in animals have shown that not all tumor cells need to express HSV-TK for this "bystander" effect to occur. This effect is not well understood, but one of several proposed mechanistic theories suggests that toxic metabolites can move through gap junctions between neighboring tumor cells. A similar approach, using different therapeutic genes, involves selectively inducing antiproliferative effects in tumor cells by introducing and expressing genes encoding antisense oligonucleotides [17].
Another method for cancer gene therapy is to protect a patient's hematopoietic system from the toxic effects of high-dose chemotherapy. The chemotherapy resistance gene currently being tested in clinical gene therapy trials is MDR-1. This gene encodes a protein (P-glycoprotein) that acts as a multidrug efflux pump, removing certain chemotherapeutic agents (e.g., taxol) from cells. However, the MDR-1 pump is ineffective against most alkylating agents, commonly used in many high-dose chemotherapy regimes, limiting the use of MDR-1 gene therapy to specific chemotherapy protocols. Additional genes are being considered to provide cells of hematopoietic lineages with selective resistance to chemotherapeutic agents and radiation for future clinical gene therapy applications [18].
Gene therapies are now being implemented clinically for diseases caused by recessive single-gene defects. These disorders could potentially be cured if a functional copy of the mutated gene is expressed in the appropriate target tissue. However, in cases where the gene product is secreted, such as Gaucher's disease and clotting factor deficiencies, several types of somatic cells could serve as targets for gene transfer. In other cases, the functional gene must be delivered and expressed in the correct cell type. For example, in thalassemia, the B-globin gene must be delivered and expressed in cells of the erythroid lineage.
Five diseases caused by genetic mutations are currently the focus of NIH RAC-approved clinical trials: severe combined immune deficiency (SCLD) syndrome, Gaucher's disease, Fanconi anemia (C), cystic fibrosis, and hypercholesterolemia [19].
AIDS is currently the only infectious disease for which there are licensed clinical gene therapy trials. The strategies for treating this disease involve protecting vulnerable cells from infection by the human immunodeficiency virus (HIV) or inhibiting further replication of HIV in already infected cells. These methods are known as intracellular immunization, a term coined by Baltimore in a commentary on a research article by McKnight and colleagues. McKnight and colleagues demonstrated that cells stably expressing a truncated form of the herpes simplex virus (HSV) trans-activator protein VP16 did not support the replication of wild-type HSV, suggesting that the presence of the truncated VP16 interfered with the function of the wild-type VP16, thereby preventing viral replication [20].
Many researchers have since attempted to discover similar mechanisms to disrupt the replication of HIV. Potential techniques for stopping HIV replication in infected cells include trans-dominant negative HIV proteins (e.g., revM10, gag), ribozymes targeting genomic RNA, antisense oligonucleotides to block the translation of HIV coding sequences, and TAR decoys. Additionally, some researchers have chosen immunotherapeutic strategies designed to enhance the immune response to HIV and HIV-infected cells. For a more comprehensive review of gene therapy techniques for AIDS, readers are referred to other sources [21].
Moreover, for gene therapy to be successful, three primary medical challenges must be addressed: first, integrating the human gene into patient cells using techniques like viruses or liposomes; second, ensuring gene delivery to the precise cells; and third, activating the gene effectively within the target cells [22].
Inherited single-gene disorders have limited treatment options. Germline gene therapy (GGT) addresses these issues by correcting mutations in gametes or embryos, thereby preventing the transmission of genetic diseases to future generations [23]. Methods include adding a synthetic gene copy using viral vectors for random integration into the genome. However, this approach raises safety, efficacy, and ethical concerns. Genome editing, using tools like TALENs, ZFNs, and CRISPR-Cas9, creates targeted mutations to modify defective genes. While promising, the effectiveness and safety of conventional gene-editing tools for widespread GGT applications remain uncertain due to the limited scope of treatable mutations and associated risks [24].
GENE THERAPY STRATEGIES:
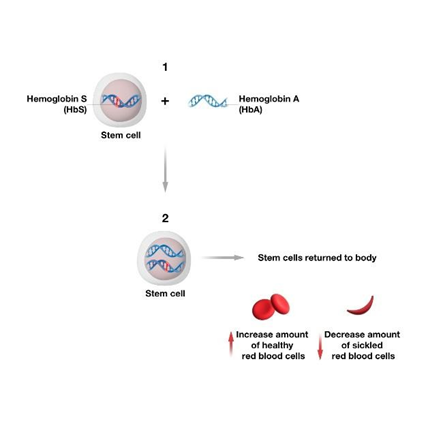
Gene addition therapy includes introducing functional gene copies to treat or remedy diseases, using vectors like genetically modified viruses to deliver these genes to target cells. Common vectors include adeno-associated viruses (AAV) and lentiviruses. This method has been applied to various diseases, including adenosine deaminase severe combined immunodeficiency (ADA-SCID), congenital blindness, hemophilia , Leber’s congenital amaurosis, lysosomal storage diseases, and X-linked chronic granulomatous disease [25].
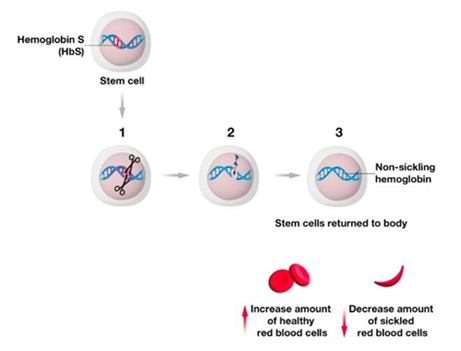
Corrective gene therapy aims to replace a mutated gene or part of it with a normal sequence, especially effective when a faulty gene produces a disease-causing protein. This method includes using gene-editing tools like TALENs, Zinc Finger Nucleases, and CRISPR/Cas9, as discussed later in the paper, to correct the defective gene [26].
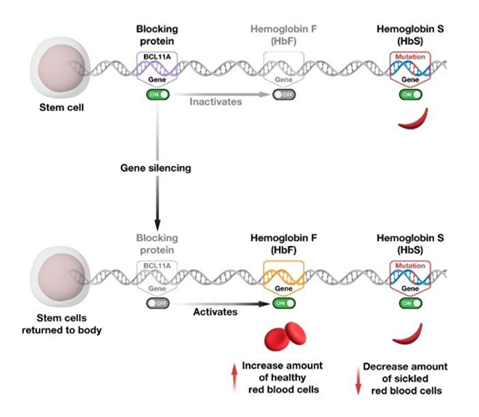
Thanks to advancements in RNA interference (RNAi) pathways and the development of antisense oligonucleotides, gene therapy can effectively silence mutated genes [27]. Antisense oligonucleotides (ASOs) are single-stranded DNA molecules that bind to target mRNA, working through RNase H-dependent mRNA degradation or RNase H-independent mechanisms. RNAi, a key pathway for gene expression regulation and viral defense, is activated when the DICER enzyme processes double-stranded RNA into siRNA and miRNA, leading to gene silencing through the RNA-induced silencing complex (RISC), which includes Argonaute proteins. This process either degrades target mRNA or suppresses its translation [28].
This involves adding one or more genes to cells of a specific type to change the characteristics of those cells. When there are multiple cell types in a tissue and the disease is caused by a malfunction in one type of cell, this technique is logical. For example, type 1 diabetes occurs because many of the insulin-producing islet cells of the pancreas are damaged, while the pancreatic cells producing digestive enzymes are unaffected. Reprogramming these cells to create insulin would help in the recovery of type 1 diabetes patients [29].
For certain diseases, such as cancer, the goal is to kill defective cells. In such cases, cell destruction is a viable option. It can be performed using a transgene that codes for a highly toxic protein that destroys the diseased cells or expresses a protein that labels the cell as an immune system target. This type of cell removal gene therapy is also referred to as gene suicide therapy [30].
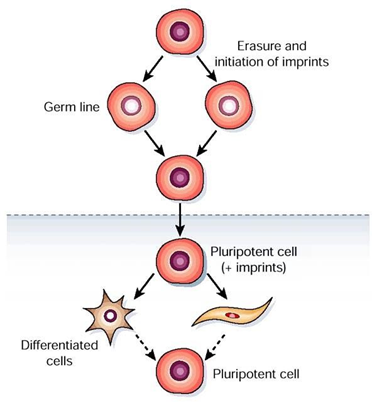
BOUNDARY BETWEEN SOMATIC AND GERM CELLS:
The boundary between somatic and germ cells, known as the Weismann barrier, is still elusive in post-treatment scenarios, which creates concerns regarding the survival of gene-transduced lymphoid cells and the potential for causing severe side effects. However, this concern is not as significant for biosafety issues if breached. Gene marking in myeloid lineage cells, as seen in only 1-2% of CD34 cells, has shown promising results in gene therapy, although the success of engraftment remains limited. Despite rapid advances in research on transduced hematopoietic stem cells, gene therapy interventions in diseases like immune deficiencies, hereditary blindness, hemophilia, blood diseases, lipid metabolism disorders, cancer, and others have been successful, but often at low levels.
Successful trials have been conducted in children with immune deficiencies, such as ADA-SCID, showing improved thymic output and better immune reconstitution with long-term follow-up. However, challenges remain, such as the risk of leukemia and opportunistic infections. Similar successes have been observed in trials using gamma-retroviral vectors for genetic diseases like X-linked SCID (SCID-X1) and Wiskott-Aldrich Syndrome (WAS), providing promising results despite the absence of genotoxicity [31].
Technologies used in Cell and Gene Therapy
a) Cell Engineering:
Cell engineering has made significant progress in recent years and is now at a stage where it can be applied practically in human patients. This involves modifying genes to produce desired cellular products. It is not only employed in basic cellular biology research, which focuses on developing biological substitutes to restore or replace cell function, but also in the production of products that rely on living cells [32].
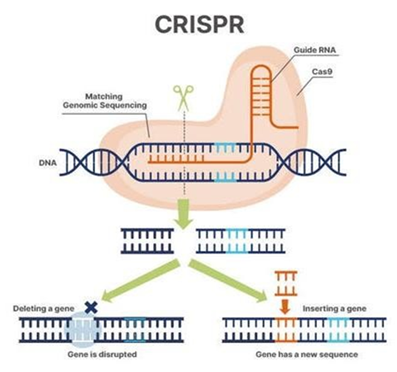
b) CRISPR/Cas9:
CRISPR/Cas9 is a gene-editing tool that makes precise cuts in DNA, allowing natural DNA repair processes to take over. The system consists of the enzyme Cas9 and an RNA guide. CRISPR/Cas9 can perform three main types of genetic edits:
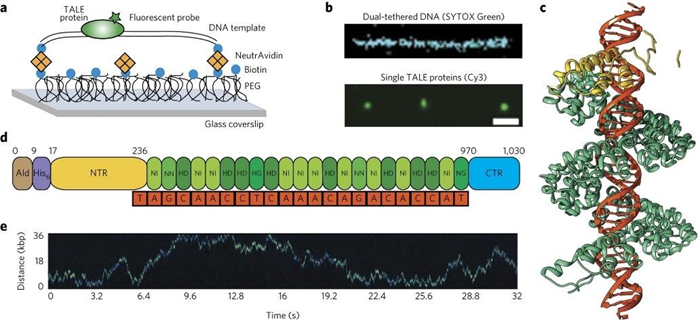
c) TALE:
The discovery of the one-to-one code governing DNA-binding specificity in transcription activator-like effector (TALE) proteins from the plant pathogen Xanthomonas has opened the possibility of designing novel DNA-binding proteins. TALE proteins consist of highly conserved amino acid repeats that bind a single base pair of DNA. These repeats can be concatenated to create long arrays with customized DNA-binding specificities. Transcription Activator-Like Effector Nucleases (TALENs) can be programmed to target nearly any DNA sequence, making them an attractive platform for targeted gene editing. However, the large size and repetitive design of TALE arrays present challenges in protein delivery in vivo [34].
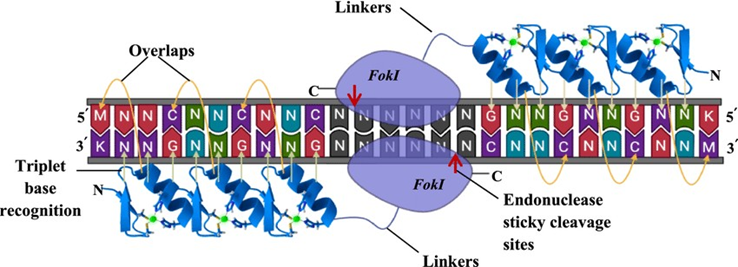
d) Zinc Finger Nuclease (ZFN):
The discovery that the DNA-binding and cleavage domains of the FokI restriction endonuclease could function independently led to the development of zinc finger nuclease (ZFN) technology. By replacing the FokI DNA-binding domain with a zinc finger domain, chimeric nucleases with unique binding specificities are created. Since the FokI nuclease operates as a dimer, inducing a double-strand break (DSB) requires two ZFNs bound to opposite strands of DNA. Initial experiments showed that ZFN-induced DSBs can be repaired by non-homologous end joining (NHEJ) or homology-directed repair (HDR), allowing for targeted genome changes. This technology has been successfully used to alter genes in human somatic and pluripotent stem cells [30,32].
Prospects:
Although in utero gene therapy holds significant promise for preventing excessive genetic diseases, its true application in humans will depend on demonstrating safety and efficacy. Rapid advancements in fetal treatment and imaging technologies will continue to improve the safety of vector delivery. This may provide more protection for the mother compared to pregnancy termination or preimplantation interventions. The safety of gene therapy vectors, particularly in cases of oncogenic events during in utero applications, remains a significant concern. Studies have shown the importance of understanding the mechanisms of these events, which could lead to the design of safer vectors in the next 3-5 years. The fetal mouse model may become a particularly sensitive test system for such vectors. Ongoing research in gene therapy will increase the demand for genetic screening programs and preventive strategies for human genetic disorders, incorporating safe and effective in utero gene therapy in the future [3,15,32].
CONCLUSION
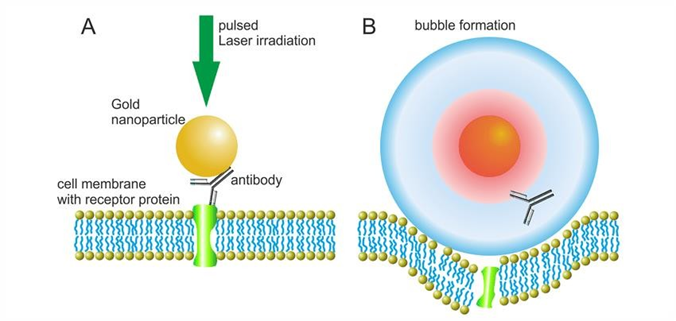
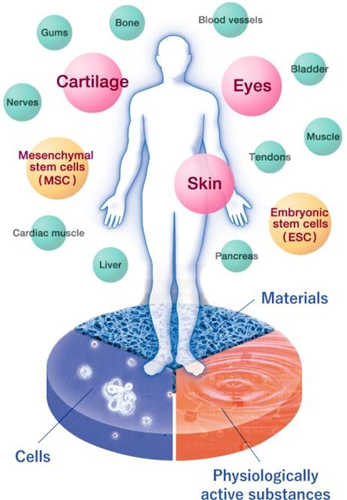
Cell and gene therapy, once regarded as science fiction, is now a reality. The emergence of genome editing tools, better vector design, and the rise of artificial intelligence and machine learning have all contributed to its exponential growth. For the successful implementation of cell and gene therapies, various delivery methodologies are used, the most prevalent of which are viral and nonviral vectors. Adenoviral, retroviral, and lentiviral systems are the most utilized viral vectors. Nonviral methods include both physical and chemical approaches. Gene guns, electroporation, ultrasound, and hydrodynamic therapy are examples of physical procedures, whereas polymers, electrostatic 44interactions, encapsulations, adsorption, liposomes, and dendrimers are examples of chemical methods. Cell and gene therapy are central themes that overlap since they are directed at treating, preventing, or curing diseases. When these therapies are administered synergistically, the potential is enormous and can be utilized for a wide range of applications including infectious diseases, inherited and genetic disorders, cardiac disease, pulmonary disease, gastrointestinal, hepatic disease, renal disease, dentistry, and cancer. Experimentation, bioinformatics, and computational biology together can reveal information about the challenges and prospects of gene delivery. It can be used to compare existing and novel therapeutic designs and foretell how multimodal or multigene therapy would behave. Artificial Intelligence is playing a vital role in making cell therapies cheaper. Oxford Bio-Medica aims to enhance yields and cost-efficiency in manufacturing viral vectors used in gene treatments by leveraging Microsoft's AI platform. Cytera, for example, provide cell culture lab automation solutions, while Synthace is developing software that automates labor-intensive experimental and quality control activities. Chronicle, a new automation program from GE Healthcare, is meant to optimize the complicated processes involved in cell therapy production. Because of its ability to alter the human genome, gene therapy has generated a lot of ethical debate. Moreover, gene therapy is expensive; therefore, it is only available to the wealthy or those who can afford it. Although there is agreement that there is an ethical distinction between gene therapy used to treat sickness and gene therapy to enhance, many people consider that enhancement (non-health related physical, mental, or moral) not acceptable. Currently, gene therapy research is focused on disease cures and preventions rather than pure enhancements. However, defining normal or discerning the fine line between preventive care and enhancement will become more challenging [9,12,25,33].
REFERENCES


Sakshi Chungade, Pooja Karpe, Gene Therapy: Current Progress and Possibilities, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 2185-2197. https://doi.org/10.5281/zenodo.18635447
 10.5281/zenodo.18635447
10.5281/zenodo.18635447