1,4 Dr. Chandramma Dayananda Sagar Institute of Medical Education and Research (CDSIMER), Harohalli, Kanakapura, Ramanagara, Karnataka, India.
2,3,5 College of Pharmaceutical Sciences, Dayananda Sagar University, Harohalli, Kanakapura, Ramanagara, Karnataka, India.
Background: The prescribing practices and the rational use of the antibiotics promote safe and cost-effective treatment of infections thereby reducing the length of the hospital stay and prevention of adverse events and polypharmacy in the elderly. The study aims at creating awareness among the healthcare professionals regarding safe antibiotic prescribing practices in the elderly population. Results The number of antibiotic prescriptions was found to be 796. 51.2 % of the patients had respiratory tract infections. Cephalosporin (318), Macrolide (139) and Penicillin (111) were the most prescribed class of antibiotics in the study population. According to WHO AWaRe classification, ‘Watch’ category had the majority with 616 prescriptions. As per WHO prescribing indicators, the average number of drugs per prescription was found to be 9. The percentage of the antibiotic prescriptions was found to be 22.27% and that of the encounters with injection at 37.77%. 4.53% of the prescriptions were given by the generic name. 33.49% of the drugs were prescribed from the essential drug list/formulary. Conclusion: The study highlighted the antibiotic prescribing practices in the elderly and helps in the formulation of new policies and procedures to strengthen the antimicrobial stewardship programme and detection of polypharmacy in the elderly.
Senescence is a natural phenomenon of all living organisms in which the body functions of the man start declining over age. It has a huge impact on the Pharmacokinetics and Pharmacodynamics of drugs. Elderly form a large section of the hospitalized patients in medical wards1. Infectious diseases pose a major challenge in the elderly for two reasons: the susceptibility to infection increases with age and when infections do occur, they often present atypically. While fever and leucocytosis are often absent, geriatric syndromes like delirium, falls and incontinence are the common presentation of infection. Hence, serious infections are likely to be missed and the focus of infection misdiagnosed1. The age alters the drug disposition of the medication leading to adverse events, lack of efficacy and toxicity.
According to the National Centre for Disease Control (NCDC), the data shows that 50% of the antibiotic use in the hospitals are found to be irrational. This can be reduced by implementing a strategic tool, “Alert antimicrobials” in the hospital. It involves in preparing guideline for the key antibiotics such as “ciprofloxacin, ceftazidime, cefotaxime, ceftriaxone, vancomycin or teicoplanin, imipenem, levofloxacin, meropenem, moxifloxacin, piperacillin-tazobactam, linezolid (oral/IV), voriconazole, caspofungin, valganciclovir, ertapenem and newer preparations of amphotericin.” The irrational use of these antibiotics make way for the occurrence of Clostridium difficile diarrhoea and Central Nervous System (CNS) toxicity including seizures2. Globally, the antibiotic use in elderly range from 4.9% to 48.5% in which one fourth of them are found to be inappropriate3.
The elderly are already fraught with polypharmacy, multimorbidity and frailty. Hence, irrational prescribing of antibiotics can result in drug-drug and drug-disease interactions and adverse drug reactions. This will impact the quality of life of the older person4. Figure 1 alert the prescribers to be vigilant, while prescribing the various classes of antibiotics in the elderly5. Geriatric facilities are reservoirs for multi-drug-resistant organisms and appropriate infection control measures are needed1. As per Global Antimicrobial Resistance and Use Surveillance System (GLASS) report (2022), 42% of the antibiotic-resistant strains belong to third generation cephalosporin-resistant E.coli strain and that of Methicillin Resistant Staphylococcus Aureus strain (MRSA) constitutes 35% among seventy-six countries6.
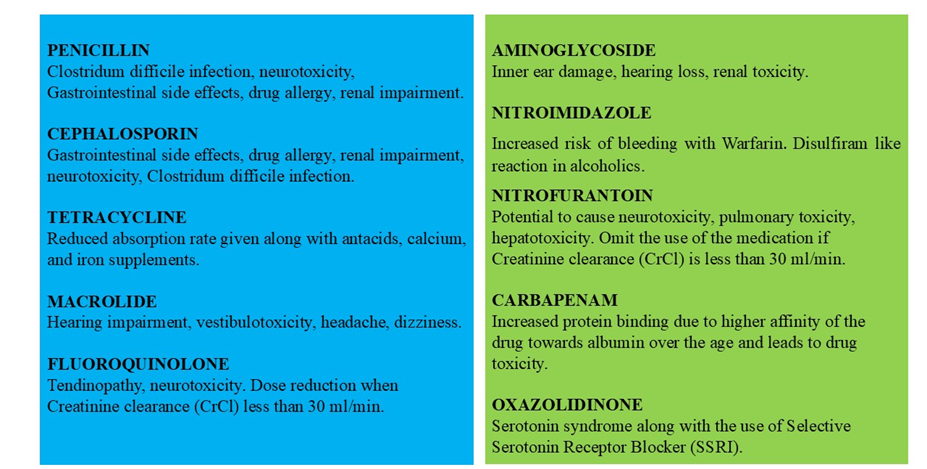
Figure 1. Safety concerns with antibiotic use in elderly5.
Adequate infection control practices have been the key strategy to combat the antimicrobial resistance for both hospital and community acquired infections. The right choice of antibiotic matters in the elderly failing which it leads to the emergence of antibiotic-resistant strains and multiple comorbidities, thereby reducing the life expectancy of the population. Hence the antibiotic prescribing practices can be strengthened by boosting the antimicrobial stewardship programme in the hospital with the help of the strategies mentioned below.
World Health Organization (WHO) developed the AWaRe (Access, Watch, Reserve) classification in 2017 as a tool to support antibiotic stewardship efforts and promote the rational use of antibiotics. “Access” contains antibiotic which are used as first or second-line treatment for common infections, are often narrow-spectrum and more affordable and widely available. “Watch” includes antibiotic with a higher risk of resistance, often broader-spectrum and used with caution. “Reserve” has antibiotics reserved for the treatment of multidrug-resistant infections as a last resort. The importance of WHO AWaRe classification is that it helps in optimizing treatment, combat antimicrobial resistance, and protects future antibiotics.
Studying the antibiotic prescribing patterns, its rationality and the appropriateness of antibiotic prescribing in the geriatrics will improve awareness and help develop better strategies to tackle the problem. It may pave the way for better prescribing, help antibiotic stewardship strategies and reduce Drug Related Problems (DRP) in the elderly4.
AIM
The study focuses on the safe antibiotic prescribing practice in the elderly population thereby creating awareness among the healthcare professionals.
MATERIALS AND METHODS
This study was conducted in the General medicine department of a tertiary care hospital, Karnataka, India from January 2023 to July 2023 with a sample size of 385 study subjects. The ethical clearance was obtained before initiating the study. The consent procedure was not applicable. The data was extracted from the patient medical records using a self-designed, validated data collection form. It was then evaluated using WHO prescribing indicators, AWaRe classification, and standard guidelines for the treatment of various diseases.
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Institutional Ethics Committee (IEC) of the hospital, Dr. Chandramma Dayananda Sagar Institute of Medical Education and Research (CDSIMER) before initiating the study. (IEC No.: CDSIMER/MR/0075/IEC/2023).
Informed consent: The need for informed consent was waived off by the Institutional Ethics Committee (IEC) of the hospital, Dr. Chandramma Dayananda Sagar Institute of Medical Education and Research (CDSIMER) as it is a retrospective observational study.
Study design: A retrospective observational study.
Sample size: It is estimated that a sample size of 385 is sufficient to achieve an estimated proportion of 50% at 95% confidence interval and at 5% marginal error with reference to the article reported by Ruchi et al.8 Convenience sampling method was done.
Place of study: Harohalli, Ramanagara district, Karnataka, India.
Source of data:
The relevant data will be collected from the patient medical records in the Medical Records Department (MRD) of the hospital.
Duration of study: The study was conducted for a period of seven months.
Inclusion criteria: Patients 60 years or older admitted to the medical wards or medical intensive care unit (ICU) and receiving at least one systemic antibiotic (oral or parenteral route).
Exclusion criteria: Patient case records with incomplete data and those using topical antibiotic were excluded.
Statistical Analysis: The variables were analysed using descriptive statistics. The level of significance was 5% at 95% confidence interval. The analysis was done using SPSS (Statistical Package of Social Sciences) version 26 for Windows 10.
RESULT
The prescriptions of the elderly patients had screening to identify the patients who were on antibiotics. Out of 548 patients, 163 (29.75%) of them were eliminated as they were not on antibiotics. 385 (70.25%) of the elderly were on antibiotics. The number of antibiotic prescriptions was found to be 796. A total of 3574 drugs were identified in the study population.
Out of 385 study subjects, males (203, 52.7%) were predominant than females (182, 47.2%). 163 study participants belong to the age group, 70-79 years old. Table 1 provide the baseline characteristics of the study. The mean age of study population was 71 years with average age of males being 72 years and that of females 71 years. The hospital stay range from 1 to 31 days. The mean length of hospital stay was found to be 8 days. 124 (32.2%) patients had longer stay in hospital and got admitted in Intensive Care Unit (ICU). 261 (67.7%) of them had stay in the wards of the hospital.
Diabetes mellitus (44.16%), Hypertension (39.22%) and Ischaemic Heart disease (7.79%) were found to be the top three comorbidities in the study population. Congestive Cardiac Failure, Bronchial Asthma, Hypothyroidism and Chronic Obstructive Pulmonary disease (COPD) were the other comorbidities seen among the study subjects (Table 1). 51.2 % of the patients had respiratory tract infections. 13 % of the patients had urinary tract infection. The suspected focus of infection was not mentioned for 10.9 % of patients. 7.3 % of the patients had multiple foci of infection. Others include antibiotic prophylaxis and ENT (Ear Nose Throat) infection. The rest of the patients had infection over gastrointestinal tract and in the skin and the soft tissues (Table 1).
The study subjects were 385 in number. The total number of antibiotic prescriptions was found to be 796. The mean number of antibiotics per patient was found to be 2.04 ranging from 1 to 5 in number. Cephalosporins (318, 40%), Macrolides (139, 17%) and Penicillins (111, 14%) were the most prescribed class of antibiotics in the study population (Table 2). Out of 796 antibiotic prescriptions, 248 of them had Ceftriaxone (31%), a cephalosporin given for Respiratory Tract Infection (RTI). 137 prescriptions had Azithromycin (17%), a macrolide as the antibiotic of choice for Respiratory Tract Infection. 60 prescriptions had Metronidazole (7.5%) for Gastroenteritis and 64 of them had Piperacillin- Tazobactum (8%) for Respiratory Tract Infection (RTI). Also, 31 prescriptions had Nitrofurantoin (3.8%) to treat Urinary Tract Infection (UTI). Majority of the patients were on empirical therapy. 97 (25%) patients had request for cultures. Serum procalcitonin test was ordered for 26 (6.7%) patients. Antibiotic prophylaxis was given for three patients who underwent cataract surgery.
The prescribed antibiotics were classified according to WHO AWaRe classification (Table 3). It helps to assess the appropriateness of antibiotics used in the study population. ‘Watch’ category had the majority with 616 prescriptions (77.39 %) while 168 (21.10 %) belonged to ‘Access’ category. Only 12 (1.5 %) antibiotics were prescribed from the ‘Reserve’ category as per WHO AWaRe classification.
According to WHO prescribing indicators, the average number of drugs per prescription was found to be 9. The percentage of the antibiotic prescriptions was found to be 22.27% and that of the encounters with injection at 37.77%. 4.53% of the prescriptions were given by the generic name. 33.49% of the drugs were prescribed from the essential drug list/formulary (Table 4).
|
Table 1. Baseline characteristics |
|||
|
Sr. no |
Variables |
Frequency (N=385) |
Percentage (%) |
|
1. |
Age |
||
|
60-69 years |
156 |
40.5 |
|
|
70-79 years |
163 |
42.3 |
|
|
80-89 years |
58 |
15 |
|
|
>=90 years |
8 |
2 |
|
|
2. |
Gender |
||
|
Male |
203 |
52.7 |
|
|
Female |
182 |
47.2 |
|
|
3. |
Length of hospital stay |
||
|
ICU |
124 |
32.2 |
|
|
Hospital ward |
261 |
67.7 |
|
|
4. |
Comorbidities |
||
|
Diabetes Mellitus |
170 |
44.16 |
|
|
Hypertension |
151 |
39.22 |
|
|
Ischaemic Heart Disease |
30 |
7.79 |
|
|
Congestive Cardiac Failure |
1 |
0.26 |
|
|
Bronchial Asthma |
12 |
3.12 |
|
|
Hypothyroidism |
10 |
2.60 |
|
|
Chronic Obstructive Pulmonary Disease (COPD) |
11 |
2.86 |
|
|
5. |
Focus of infection |
||
|
Respiratory tract |
197 |
51.2 |
|
|
Gastrointestinal tract |
32 |
8.3 |
|
|
Urinary tract |
50 |
13 |
|
|
Multiple foci |
28 |
7.3 |
|
|
Skin and Soft tissue |
19 |
4.9 |
|
|
Others |
17 |
4.4 |
|
|
Not specified |
42 |
10.9 |
|
|
Table 2. Antibiotic use |
|||
|
Sr. no. |
Class of antibiotics |
Number of prescriptions (N = 796) |
Percentage (%) |
|
|
Cephalosporins |
318 |
40 |
|
|
Macrolides |
139 |
17 |
|
|
Penicillins |
111 |
14 |
|
|
Nitroimidazoles |
63 |
8 |
|
|
Fluroquinolones |
82 |
10 |
|
|
Nitrofurantoin |
31 |
4 |
|
|
Tetracyclines |
15 |
2 |
|
|
Carbapenems |
18 |
2 |
|
|
Aminoglycosides |
13 |
2 |
|
|
Oxazolidinones |
06 |
1 |
|
Table 3. WHO AWaRe CLASSIFICATION |
||||
|
Sr. No. |
WHO AWaRe category |
Antibiotic given |
No. of antibiotic prescription (N= 796) |
Percentage (%) |
|
1. |
ACCESS |
Amoxicillin |
02 |
21.1 |
|
Amoxicillin plus Clauvulinic acid |
45 |
|||
|
Metronidazole |
60 |
|||
|
Tinidazole |
03 |
|||
|
Nitrofurantoin |
31 |
|||
|
Doxycycline |
14 |
|||
|
Amikacin |
01 |
|||
|
Gentamicin |
07 |
|||
|
Clindamycin |
05 |
|||
|
Total |
168 |
|||
|
2. |
WATCH |
Cefoperazone, sulbactam |
20 |
77.38 |
|
Ceftriaxone |
248 |
|||
|
Cefpodoxime |
03 |
|||
|
Cefixime |
31 |
|||
|
Cefodoxime, clavulanic acid |
7 |
|||
|
Cefotaxime |
4 |
|||
|
Cefuroxime |
4 |
|||
|
Azithromycin |
137 |
|||
|
Clarithromycin |
02 |
|||
|
Piperacillin, tazobactam |
64 |
|||
|
Ciprofloxacin |
40 |
|||
|
Ofloxacin |
07 |
|||
|
Norfloxacin |
31 |
|||
|
Levofloxacin |
04 |
|||
|
Meropenem |
14 |
|||
|
Total |
616 |
|||
|
3. |
RESERVE |
Ceftazidime avibactum |
01 |
1.5 |
|
Tigecycline |
01 |
|||
|
Faropenem |
04 |
|||
|
Linezolid |
06 |
|||
|
Total |
12 |
|||
|
Table 4. WHO prescribing indicators |
|||
|
Sr. no. |
Indicators |
Test value |
Reference value |
|
1. |
Average number of drugs per prescription. |
9 |
<2 |
|
2. |
Percentage of encounters with an antibiotic prescribed. |
22.27 |
<30 % |
|
3. |
Percentage of encounters with injection prescribed. |
37.77 |
<20 % |
|
4. |
Percentage of drugs prescribed by generic name. |
4.53 |
100 % |
|
5. |
Percentage of drugs prescribed from the essential drug list/formulary. |
33.49 |
100 % |
DISCUSSION
Seventy percent of the elderly screened had received antibiotics. The gender distribution was almost the same among the elderly study subjects. All of them had at least eight days of hospital stay. Most of them had respiratory tract infections and urinary tract infections in the study population. The same was observed in the study conducted by Dilip Chandrasekhar et al., in which 30% of the prescriptions had antibiotics to treat respiratory tract infections1. The elderly had diabetes mellitus and hypertension as the major comorbidities. Cephalosporins, Macrolides and penicillins were the major class of antibiotics given in the elderly population.
We observed that the elderly patient received an average of two antibiotics. The study subjects had received an average of nine drugs. “Use of more than five medications in the people who crossed 65 years old, treated as polypharmacy” as per American Geriatric Society (AGS) Beers criteria9. According to the WHO prescribing indicators, the number of drugs to be prescribed per patient is less than two. The study shows that the injections were prescribed more in number compared to the reference value, less than 20%. The reasons could be that the hospital where the study was conducted caters to a rural and mostly illiterate population which demands instant gratification and injections and the doctors often succumb to their pressure. Injections mean more expense, need for trained personnel and has a greater potential for serious side effects compared to oral medications. Health education of the public is needed so that their unfounded beliefs and attitudes can be rectified. It is very much essential to create an awareness regarding the use of Generic name and the selection of the medication from the Essential Medicine List while prescribing. But, only a third satisfied this criterion. Antibiotic prescriptions were found to be optimal, less than thirty percent, a good sign as per the WHO recommendations reflecting the efforts to promote the rational use of antibiotics in the hospital10.
Looking at the prescriptions according to WHO AWaRe classification, a tool to support monitoring of antibiotic prescribing, the ‘Watch’ group of antibiotics were the major one that were of higher resistance potential. WHO has introduced a new target, stating that by 2023 at least 60% of national antibiotic consumption should come from the ‘Access’ group which are considered as first- or second-line agents in the empiric treatment of common infectious syndromes and should therefore be widely available and affordable. A worldwide point prevalence survey of antibiotic prescribing patterns in adults as per WHO AWaRe classification was studied in 664 hospitals across 69 countries in which a higher use of ‘Watch’ antibiotics was noted particularly in lower and upper- middle- income countries. There were large differences in AwaRe prescribing at country level. ‘Watch’ group has a higher risk of developing resistance and are used as first- or second-line options for a limited number of indications. These are the antibiotics that need to be monitored and prioritized as targets for stewardship programmes11.
Our study was exhibiting the treatment patterns with the use of Amoxicillin and its combination with clavulaunic acid, Metronidazole, Doxycycline, Tinidazole, Nitrofurantoin, Amikacin, Gentamicin, Clindamycin which belong to ‘Access’ category. Also, Cefoperazone and sulbactam, Ceftriaxone, Cefpodoxime, Cefixime, Cefpodoxime and clavulanic acid, Cefotaxime, Cefuroxime, Azithromycin, Clarithromycin, Piperacillin and Tazobactam, Ciprofloxacin, Ofloxacin, Norfloxacin, Levofloxacin, Imipenem and Meropenem were used that belong to ‘Watch’ category. The treatment regimen also include Ceftazidime avibactum, Tigecycline, Faropenem, Linezolid and Aztreonam that belong to Reserve category. It alerts the healthcare professional to be more vigilant with the use of antibiotics, majority of them belong to watch category. The study suggests the practitioners to select antibiotics more of the category, Access group. Many at times, the severity of infections demands the extensive use of antibiotics that most of which fell into watch category. The findings urge the hospital authorities to strengthen the monitoring strategies and to formulate policies and procedures to combat antimicrobial resistance. It would help them to make informed choices while selecting the therapeutic regimen to treat infections12.
‘Reserve’ group, the last resort antibiotic prescribing which was highest in Argentina, India, and Brazil according to the world-wide point prevalence study13. Access-to-Watch ratio was 0.27 in our study. Most of the countries had an Access-to-Watch ratio lower than 1. The lowest ratio (0.1) was observed in Armenia and Jordan, whereas Guinea had the highest Access-to-Watch ratio (2.1), followed by South Africa (1.6), Togo (1.5) and the UK (1.5). Ideally, ‘Access’ antibiotic use should be greater than ‘Watch’ group and the ratio should be more than one12.
The above findings show that the prescribing practices for antibiotics in our study is far from recommended. The reasons could be the inadequate training of junior and senior residents on the best practices regarding antibiotic use and lack of awareness of the recently formulated local antibiotic policy. Another point noted is that doctors’ training during the Corona Virus Infectious Disease (COVID-19) pandemic suffered a setback due to obvious reasons. There is a tendency to start antibiotics for every ill or unstable patient without a systematic approach. Starting antibiotics in a sick patient without trying to find the cause gives a false sense of security and should be discouraged. In a significant segment, no likely focus of infection was documented. This group had culture sent in one, severe sepsis was documented in one and serum procalcitonin test was not sent in any. Often no attempt is made to determine if there is an infection at all and if so, what is the likely focus, the most likely bug and whether the prescribed antibiotic is appropriate and will reach the site in sufficient concentration. New doctors set a trend and changing these wrong practices is far from easy. Teaching hospitals should set standards for rational prescribing. Training of prescribers, strict monitoring of appropriateness of prescriptions and health education of rural population about the misuse/overuse of antibiotics is essential.
Pharmacokinetic and Pharmacodynamic changes are quite evident with the advancement of age. Hence, we need to be cautious with the choice of medications in the elderly. Practices contrary to guidelines noted were use of Nitrofurantoin (a potentially inappropriate medication in elderly according to Beers criteria) in urinary tract infection including those with renal failure, Nitrofurantoin was administered in our study for urinary tract infection and possess an unfavorable side effect profile such as pulmonary toxicity, hepatotoxicity and peripheral neuropathy9,14. Also, it does not reach adequate concentration in the urinary tract in the presence of renal failure and should be avoided in elderly. Baclet et al., says that there are definitions for the various types of potentially inappropriate antibiotic prescriptions among elderly. These findings require an external validation to use it in our practice. Examples of inappropriate prescriptions are nitrofurantoin for urinary tract infection (UTI), amoxicillin-clavulanic acid as empirical therapy for UTI, ceftriaxone for pneumococcal community acquired pneumonia (CAP), macrolide for CAP except legionellosis, fluoroquinolone as first line treatment of pneumonia and upper respiratory tract infection, treatment of diarrhea with antibiotics, amoxicillin-clavulanic acid for nosocomial gastrointestinal infections, piperacillin-tazobactam for community acquired infections, combining amoxicillin-clavulanic acid with metronidazole, giving antibiotics for more than 7 days for pneumonia and prescribing antibiotics for viral infections14.
Other common practices contrary to guidelines noted were treating asymptomatic urinary infections in elderly, using intravenous fluoroquinolones although they have good oral bioavailability, treating all COPD acute exacerbations with antibiotics, treating every acute diarrhoeal illness with fluoroquinolone and metronidazole and systemic antibiotics for skin infections without systemic manifestations and these must be emphasized during education of prescribers.
It was difficult to make out whether the cultures were sent for the patients. In case of sending culture test, we were unable to make out whether it was done before initiating antibiotics. Starting antibiotics upfront before obtaining reports may be required only in unstable patients like those with severe sepsis. There was a general reluctance to deescalate antibiotics if no obvious indication was identified. Deprescribing can be encouraged to prevent polypharmacy. The reason for starting or stopping or changing an antibiotic in the case file needs to be emphasized for better patient care. Documentation of focus of infection, basis for diagnosing sepsis, culture and chest radiographs were often absent or unclear from the records. Incomplete documentation was a major hurdle as it was a retrospective study. Also, it could lead to exaggeration of the findings.
CONCLUSION
Rational prescribing results in the reduction of cost, adverse events, and antimicrobial resistance. It is recommended to have judicious use of antibiotics while treating infections in the elderly. The older adults are highly sensitive and develop tolerance to the medications with the advancement of the age. The prescribers need to be cautious while treating the elderly to avoid drug toxicity because of age related changes in the pharmacokinetic and pharmacodynamic parameters. Cognitive impairment leads to medication non adherence in them. It is very much essential to strengthen the hospital surveillance methods such as antimicrobial stewardship programme to regulate the use of antibiotics and the emergence of antimicrobial resistant strains. Educational interventions can be implemented in the hospital to raise awareness regarding polypharmacy and optimal use of antibiotics. Continuing Medical Education (CME) programme can be conducted to encourage the doctors to prescribe antibiotics of Access category as per WHO AWaRe classification. It would help practitioners to make informed choices while selecting the therapeutic regimen to treat infections. Further studies are required to measure the extent of polypharmacy in the hospital settings. Strategies like the restriction of hospital formulary can be devised to alert the doctors during the selection of the antibiotic. It helps in strengthening the facets of the pharmaceutical care.
LIMITATION
Being a retrospective observational study, direct patient interview and clarification of the data collected were not possible. The sample size was small and does not exhibit generalizability of the result. The study can be extrapolated to other medical departments in special population to assess the safe prescribing patterns of antibiotics. Further studies can be done to evaluate the patterns of polypharmacy and Drug Related Problem (DRP).
LIST OF ABBREVIATIONS
DECLARATION
This retrospective observational study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Institutional Ethics Committee (IEC) of the hospital, Dr. Chandramma Dayananda Sagar Institute of Medical Education and Research (CDSIMER) before initiating the study. (IEC No.: CDSIMER/MR/0075/IEC/2023).
Informed consent: The need for informed consent was waived off by the Institutional Ethics Committee (IEC) of the hospital, Dr. Chandramma Dayananda Sagar Institute of Medical Education and Research (CDSIMER) as it is a retrospective observational study.
The authors have no relevant financial or non-financial interests to disclose.
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by [Betsy Mathew], [Mamata Gurupad Kanchugar], [Prithvika Wagle], [Tayeeb Ahmed] and [Lita Susan Thomas]. The first draft of the manuscript was written by [Lita Susan Thomas] and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
The authors would like to express their heartfelt gratitude to all the healthcare and non- healthcare professionals for the smooth conduct and co-operation throughout the study.
Studies involving plants must include a statement specifying the local, national, or international guidelines and legislation and the required or appropriate permissions and/or licenses for the study: Not Applicable.
REFERENCES





Betsy Mathew, Mamata Gurupad Kanchugar, Prithvika Wagle, Tayeeb Ahmed, Lita Susan Thomas, Geriatric Antibiotic Use in the Medical Wards of a Tertiary Care Hospital, India: A Retrospective Observational Study, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 2410-2421. https://doi.org/10.5281/zenodo.19594915
 10.5281/zenodo.19594915
10.5281/zenodo.19594915
