
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Dr. Shivajirao Kadam College of Pharmacy, Kasbe Digraj, Sangli, India
Metabolic disorders like diabetes mellitus and dyslipidemia are emerging as major health problems across the globe, which often occur concurrently, giving rise to cardiovascular complications. The standard pharmacological treatment using statins, fibric-acid derivatives, and oral hypoglycemic drugs has been quite successful but can cause severe side effects on continued use. So, the demand for herbal drugs having potential anti-diabetic and hypocholesteremic activities has gained quite an impetus. The present review highlights the various herbal drugs having dual potentials along with Gymnema sylvestre, Momordica charantia, Trigonella foenum-graecum, Curcuma longa, Allium sativum, Phyllanthus emblica, and Terminalia arjuna. These plants work on the principle of carbohydrate and lipid metabolism, enzyme inhibition (?-amylase, ?-glucosidase, and HMG-CoA reductase), potentiating the effect of insulin, and antioxidant activity. There are appreciable results in clinical and laboratory investigations demonstrating their potential use in modifying lipid and glucose level abnormalities.
Diabetes Mellitus (DM) and Dyslipidemia are two of the most prevalent Non-communicable Diseases, making a major contribution to morbidity and mortality worldwide. According to the International Diabetes Federation, an estimated 537 million adults were living with diabetes in 2021, and it is expected to rise to 783 million by 2045 [4]. Also, an increased level of Total Cholesterol, Triglycerides, and Low-Density Lipoprotein Cholesterol (LDL-C), with decreased concentration of High-Density Lipoprotein Cholesterol (HDL-C), defines Dyslipidemia, often found to co-exist with Diabetes Mellitus, posing an increased risk of Cardiovascular Diseases [5].
Although certain breakthroughs have been attained in drug therapy, the long-term control of these conditions continues to pose a problem. The available allopathic agents like statins, fibres, metformin, and sulphonylureas, which have been found effective in controlling these conditions, are known to exhibit certain side effects like liver impairment, gastrointestinal disturbances, and hypoglycemia, among others [6–8].
Herbal medicine, which has been an integral part of ancient healing practices like Ayurveda, Traditional Chinese Medicine (TCM), and Unani medicine for centuries, holds great promise because of its multi-targeted and more holistic approach. Herbal plants are known to possess varied biological compounds like alkaloids, flavonoids, terpenoids, glycosides, and saponins, many of which affect the metabolism of carbohydrates and lipids [9-10].Biologically active compounds in herbal plants.
There are a large number of biologically active compounds present in herbal plants. These include:
Plants such as Momordica charantia (bitter melon) trigger AMP-activated protein kinase (AMPK) activation, thereby imitating insulin activity and lowering lipid levels [11]. Trigonella foenum-graecum (fenugreek) sensities cells to insulin and normalizes cholesterol levels through its saponin component [12]. Allium sativum (garlic) has hypolipidemic properties that involve HMG-CoA reductase inhibition and increased cholesterol secretion [13]. Similarly, Curcuma longa (turmeric) has strong antioxidant properties that involve NF-κB/PPAR activation [14-15].
With the rising incidence of metabolic disorders, where modern treatments have shown limitations, there is a prospect for exploring an alternate approach for the management of diabetes and lipid disorders using herbs. The main objective of this review is to discuss the prevailing scientific knowledge available on herbs with dual capabilities in lowering lipids as well as in treating diabetes, based on their molecular mechanisms, phytoconstituent, and significance[1, 3].
Diabetes Mellitus and Dyslipidemia
Diabetes Mellitus is closely linked with Dyslipidemia, and both conditions share similar etiological pathways, including Insulin Resistance, Oxidative Stress, and Inflammation. Recognizing this association is critical to appreciating the dual utility of Herbal Medicines.
2.1 Diabetes Mellitus: A Metabolic Overview
Diabetes mellitus is a chronic metabolic disorder characterized by hyperglycemia resulting from defects in insulin secretion, insulin action, or both. The persistent hyperglycemia then leads to disturbances in metabolism in carbohydrates, fats, and proteins.
Insulin resistance includes impaired glucose uptake in muscles and adipose tissue and enhanced hepatic production of glucose. High levels of FFAs and pro-inflammatory cytokines such as TNF-α and IL-6 enhance insulin signaling defects. Activation of stress pathways leading to NF-κB and JNK contributes to apoptosis of β-cells and progression of metabolic dysfunction [16].
2.2 Dyslipidemia: Lipid Metabolism and Abnormalities
Dyslipidemia is an imbalance of lipid components and generally defined by an elevated total cholesterol, LDL-C, triglycerides (TG), and reduced HDL-C levels. It is considered to be both a cause and consequence of insulin resistance.
In insulin-resistant states, LPL activity is reduced, resulting in diminished clearance of triglyceride-rich lipoproteins. Paralleling these events, increased HSL activity within WAT promotes lipolysis, increasing plasma FFAs. These FFAs are subsequently taken up by the liver, promoting VLDL overproduction and hepatic steatosis.
Moreover, insulin resistance suppresses the degradation of ApoB100, which results in an increase in the synthesis of LDL particles and the promotion of atherogenesis [17–19].
2.3 The Interrelationship Between Diabetes and Dyslipidemia
Diabetes and dyslipidemia are mutually potentiating conditions. Hyperglycemia accelerates the glycation of LDL, thereby rendering it highly atherogenic, and dyslipidemia further potentiates insulin resistance by inhibiting insulin receptor function through accumulation of Diacylglycerol and activation of protein kinase C
The general molecular pathways that underpin both conditions include:
These overlapping properties account for the effectiveness of herbs that possess antioxidant, anti-inflammatory, and insulin-sensitizing properties within the management of both diseases [20-21].
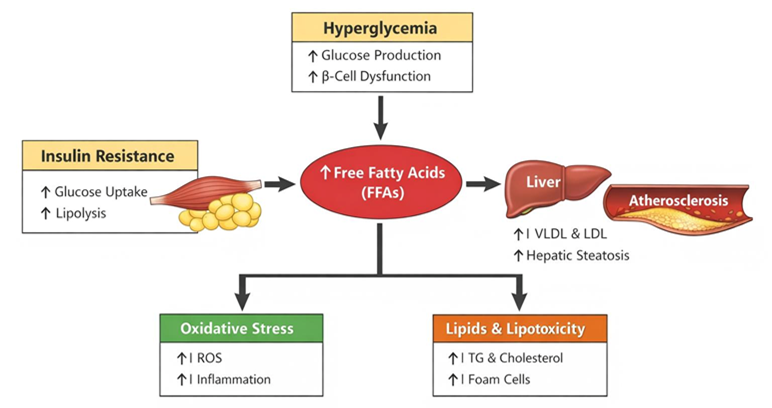
Figure 1. Mechanistic link between insulin resistance, hyperglycemia, and dyslipidemia,
Herbal drugs have hypolipidemic and anti-diabetic effects through diverse mechanisms, which involve several biochemical processes like carbohydrate metabolism, glucose transport, lipid biosynthesis, and modulation of oxidative stress. In contrast to conventional drugs, which mainly interact with a single target, herbal combinations interact with multiple targets, thereby improving overall metabolism.
3.1 Enzyme Inhibition and Glucose Regulation
Many plants medicinal plants act by inhibiting critical carbohydrate-hydrolyzing enzymes, such as α-amylase and α-glucosidase, to slow down the digestion process and reduce postprandial glucose elevation. Gymnemic acids from Gymnema sylvestre, charantin from Momordica charantia, and trigonelline from Trigonella foenum-graecum have competitive inhibition on these enzymes [22].
Some herbs also inhibit glucose-6-phosphatase and fructose-1,6-bisphosphatase, inhibiting hepatic gluconeogenesis [23]. Camellia sinensis (green tea) and Phyllanthus emblica (amla) polyphenols also facilitate GLUT-4 translocation in skeletal muscles, leading to increased peripheral glucose uptake [24].
3.2 HMG-CoA Reductase Inhibition and Lipid Regulation
Among the major targets of hypolipidemic drugs, 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase has emerged as one of the important pivotal enzymes in the synthesis of cholesterol. Natural compounds such as guggulsterone from Commiphora mukul, curcumin from Curcuma longa, and allicin from Allium sativum have been shown to inhibit the biosynthesis of cholesterol
In addition, saponins derived from Trigonella foenum-graecum and Terminalia arjuna induce insolubility in complexes with bile acids, thereby enhancing cholesterol secretion, thereby lowering LDL-C concentrations [28].
3.3 Antioxidant and Anti-Inflammatory Pathways
Oxidative stress plays a pivotal role in both diabetes and dyslipidemia by impairing insulin signaling and oxidizing LDL particles. Herbal extracts rich in flavonoids, tannins, and phenolic acids neutralize reactive oxygen species (ROS), upregulate superoxide dismutase (SOD), glutathione peroxidase (GPx), and catalase, thereby restoring redox balance [29–30].
Furthermore, compounds such as curcumin, quercetin, and resveratrol downregulate inflammatory mediators like TNF-α, IL-6, and NF-κB, protecting pancreatic β-cells and improving endothelial function [31–32].
3.4 Insulin Sensitization and Signaling Enhancement
Several plant-derived compounds enhance insulin sensitivity via activation of the AMP-activated protein kinase (AMPK) and PPAR-γ pathways, both of which are crucial in glucose and lipid metabolism.
For example:
3.5 Modulation of Gut Microbiota and Metabolome
Recent studies highlight the role of the gut microbiome in regulating metabolic health. Polyphenols and fibers in herbal remedies serve as prebiotics, promoting beneficial bacteria like Bifidobacterium and Akkermansia, which improve glucose and lipid metabolism.
Herbal components such as gallic acid, ellagic acid, and catechins modulate bile acid metabolism and short-chain fatty acid (SCFA) production, influencing insulin sensitivity and lipid utilization [36–38].
Table 1. Key Mechanisms of Herbal Remedies with Dual Hypolipidemic and Anti-Diabetic Activities
|
Mechanism |
Molecular Target |
Representative Herbs |
Key Phytochemicals |
Therapeutic Outcome |
|
Enzyme inhibition |
Α-Amylase, α-Glucosidase |
Gymnema sylvestre, Trigonella foenum-graecum |
Gymnemic acid, Trigonelline |
↓ Postprandial glucose |
|
HMG-CoA reductase inhibition |
HMG-CoA reductase |
Allium sativum, Commiphora mukul |
Allicin, Guggulsterone |
↓ LDL-C, ↑ HDL-C |
|
Antioxidant activity |
ROS, NF-κB |
Curcuma longa, Phyllanthus emblica |
Curcumin, Ascorbic acid |
↓ Oxidative stress |
|
Insulin sensitization |
AMPK, PPAR-γ |
Momordica charantia, Berberis aristata |
Charantin, Berberine |
↑ Glucose uptake |
|
Gut microbiota modulation |
SCFA, bile acid |
Camellia sinensis, Terminalia arjuna |
Catechins, Tannins |
Improved lipid metabolism |
Plants with dual hypolipidemic and anti-diabetic activities exhibit their effects through diverse mechanisms including modulation of glucose metabolism, lipid regulation, and enhancement of antioxidant defense. Below are key herbal agents widely validated through pharmacological and clinical studies.
4.1 Gymnema sylvestre (Gurmar)
Gymnema sylvestre is a traditional antidiabetic herb from Ayurveda, known as the “sugar destroyer.” Its bioactive gymnemic acids suppress intestinal glucose absorption by competitively binding to taste and intestinal glucose receptors.
It enhances pancreatic β-cell regeneration, increases insulin secretion, and improves glycogen storage. Moreover, Gymnema exhibits mild hypolipidemic activity by inhibiting HMG-CoA reductase and lowering triglycerides and LDL cholesterol.
Major Phytoconstituents: Gymnemic acids, gurmarin, flavones.
Mechanisms: Inhibition of glucose absorption, insulin secretion stimulation, lipid modulation.
Outcomes: ↓ Blood glucose, ↓ TG, ↓ LDL, ↑ HDL.
4.2 Momordica charantia (Bitter Melon)
Momordica charantia is rich in insulin-like peptides (polypeptide-p), charantin, and vicine, which mimic insulin action. It activates AMPK and enhances glucose uptake in skeletal muscles.
Animal studies and human trials report significant decreases in fasting blood glucose and HbA1c levels.
In dyslipidemia, M. Charantia reduces plasma triglycerides and total cholesterol by upregulating PPAR-α, promoting fatty acid oxidation.
Major Phytoconstituents: Charantin, vicine, polypeptide-p.
Mechanisms: Insulin mimetic activity, AMPK activation, lipid oxidation.
Outcomes: ↓ Fasting glucose, ↓ TC, ↓ TG.
4.3 Trigonella foenum-graecum (Fenugreek)
Fenugreek seeds contain high levels of soluble fiber and saponins, which delay gastric emptying and reduce intestinal glucose uptake. Its alkaloid trigonelline and amino acid 4-hydroxyisoleucine stimulate insulin secretion from pancreatic β-cells.
Additionally, fenugreek decreases cholesterol absorption and enhances bile acid excretion, leading to improved lipid profiles.
Major Phytoconstituents: Trigonelline, diosgenin, 4-hydroxyisoleucine.
Mechanisms: Insulin secretion, glucose uptake, bile acid binding.
Outcomes: ↓ FPG, ↓ TC, ↓ LDL, ↑ HDL.
4.4 Curcuma longa (Turmeric)
Curcumin, the principal polyphenol in turmeric, exhibits potent antioxidant, anti-inflammatory, and hypolipidemic actions. It modulates NF-κB, AMPK, and PPAR-γ pathways to enhance insulin sensitivity and suppress hepatic gluconeogenesis.
Curcumin also prevents LDL oxidation and reduces hepatic lipid accumulation.
Major Phytoconstituents: Curcumin, demethoxycurcumin, bisdemethoxycurcumin.
Mechanisms: Antioxidant defense, AMPK activation, lipid regulation.
Outcomes: ↓ Glucose, ↓ LDL, ↓ TG, ↑ HDL.
4.5 Allium sativum (Garlic)
Garlic’s hypolipidemic and antidiabetic properties are attributed to sulfur-containing compounds such as allicin and S-allyl cysteine. These compounds enhance insulin sensitivity, improve endothelial function, and reduce hepatic cholesterol synthesis by inhibiting HMG-CoA reductase.
Clinical studies demonstrate significant reductions in fasting glucose, LDL-C, and triglycerides with regular garlic supplementation.
Major Phytoconstituents: Allicin, S-allyl cysteine, ajoene.
Mechanisms: HMG-CoA inhibition, insulin sensitization, antioxidant activity.
Outcomes: ↓ LDL, ↓ TG, ↓ FPG.
4.6 Phyllanthus emblica (Indian Gooseberry / Amla)
Amla is a potent antioxidant and rejuvenating herb used in traditional formulations. Its vitamin C and polyphenol content enhance β-cell protection and insulin secretion.
It modulates lipid metabolism via upregulation of LPL and downregulation of HMG-CoA reductase, resulting in reduced serum triglycerides and cholesterol levels.
Major Phytoconstituents: Ascorbic acid, ellagic acid, gallic acid, emblicanin A & B.
Mechanisms: Antioxidant action, enzyme modulation, β-cell protection.
Outcomes: ↓ TC, ↓ LDL, ↑ HDL, improved glycemic control.
4.7 Terminalia arjuna
Terminalia arjuna bark extract is known for cardioprotective and lipid-lowering effects. Its triterpenoids and flavonoids enhance antioxidant enzyme activity, reduce LDL oxidation, and inhibit cholesterol biosynthesis.
It is also shown to improve insulin sensitivity and vascular function, making it useful in diabetes-related dyslipidemia.
Major Phytoconstituents: Arjunolic acid, tannins, flavones.
Mechanisms: HMG-CoA reductase inhibition, antioxidant, PPAR activation.
Outcomes: ↓ LDL, ↓ TG, improved insulin function.
4.8 Berberis aristata (Tree Turmeric)
The alkaloid berberine is one of the most studied plant-derived compounds for diabetes and lipid control. It activates AMPK, increases glucose uptake, and reduces hepatic gluconeogenesis.
Berberine also stabilizes LDL receptors, enhancing cholesterol clearance.
Major Phytoconstituents: Berberine, palmatine, berbamine.
Mechanisms: AMPK activation, LDL receptor upregulation, insulin sensitization.
Outcomes: ↓ HbA1c, ↓ LDL, ↓ TG, improved insulin resistance.
4.9 Camellia sinensis (Green Tea)
Green tea catechins improve glucose tolerance, inhibit α-amylase, and modulate lipid absorption. They also upregulate adiponectin, enhance insulin sensitivity, and reduce oxidative stress.
Major Phytoconstituents: Epigallocatechin gallate (EGCG), catechins, theanine.
Mechanisms: Antioxidant, enzyme inhibition, adiponectin modulation.
Outcomes: ↓ Glucose, ↓ LDL, ↓ TG, improved antioxidant status.
Table 2. Summary of Major Herbal Remedies with Dual Anti-Diabetic and Hypolipidemic Activities
|
Herb |
Key Phytochemicals |
Primary Mechanisms |
Therapeutic Outcomes |
|
Gymnema sylvestre
|
Gymnemic acids |
Glucose absorption inhibition, β-cell regeneration |
↓ Glucose, ↓ LDL |
|
Momordica charantia |
Charantin, polypeptide-p |
Insulin mimetic, AMPK activation |
↓ FPG, ↓ TG |
|
Trigonella foenum-graecum |
Trigonelline, diosgenin |
Insulin secretion, bile acid binding |
↓ TC, ↑ HDL |
|
Curcuma longa |
Curcumin |
NF-κB inhibition, PPAR activation |
↓ LDL, ↓ HbA1c |
|
Allium sativum |
Allicin, S-allyl cysteine |
HMG-CoA inhibition |
↓ LDL, ↓ TG |
|
Phyllanthus emblica
|
Ellagic acid, emblicanin A/B |
Antioxidant, β-cell protection |
↓ LDL, ↑ HDL |
|
Terminalia arjuna |
Arjunolic acid |
HMG-CoA inhibition, antioxidant |
↓ LDL, improved insulin |
|
Berberis aristata |
Berberine |
AMPK activation, insulin sensitization |
↓ HbA1c, ↓ TG |
|
Camellia sinensis
|
EGCG, catechins |
Enzyme inhibition, antioxidant |
↓ Glucose, ↓ TG |

Figure 2: Mechanistic Overview of Herbal Bioactives
A large body of evidence from clinical studies supports the efficacy of several herbal agents and formulations in improving glycemic control and lipid metabolism. Clinical validation is essential for translating preclinical findings into evidence-based therapeutics.
5.1 Clinical Evidence on Individual Herbs
5.1.1 Gymnema sylvestre
A double-blind, placebo-controlled study involving Type 2 diabetes patients showed that supplementation with Gymnema sylvestre leaf extract (400 mg/day) for 18–20 weeks significantly reduced fasting blood glucose, HbA1c, and LDL levels while increasing serum insulin and HDL [39]. Another trial indicated partial regeneration of pancreatic β-cells, corroborating its insulinotropic action [40].
5.1.2 Momordica charantia (Bitter Melon)
A randomized trial with 100 T2DM patients receiving 2,000 mg/day of M. Charantia fruit extract for 4 months demonstrated significant reductions in fasting glucose, HbA1c, and triglyceride levels compared with baseline values [41].
In another multicenter study, bitter melon extract improved oral glucose tolerance and decreased hepatic lipid accumulation, indicating its dual hypoglycemic and lipid-lowering effect [42].
5.1.3 Trigonella foenum-graecum (Fenugreek)
Fenugreek seed powder (10 g/day) administered for 8 weeks in diabetic patients produced marked decreases in fasting glucose, total cholesterol, and triglycerides, with improved HDL levels [43].
A clinical crossover study showed fenugreek’s ability to reduce postprandial glucose and HbA1c, attributed to its soluble fiber and 4-hydroxyisoleucine content [44].
5.1.4 Curcuma longa (Turmeric)
A 12-week randomized placebo-controlled study found that curcumin supplementation (500 mg twice daily) significantly lowered fasting glucose, HbA1c, LDL-C, and triglyceride levels in T2DM patients [45].
Another trial involving subjects with metabolic syndrome demonstrated that curcumin enhanced HDL and adiponectin levels while reducing oxidative stress markers like MDA (malondialdehyde) [46].
5.1.5 Allium sativum (Garlic)
A meta-analysis of 26 clinical studies confirmed that garlic supplementation (600–1,500 mg/day) significantly reduced fasting glucose, total cholesterol, and LDL-C while increasing HDL-C [47].
A separate study reported a notable improvement in insulin sensitivity and reduction in HbA1c after 12 weeks of garlic extract administration [48].
5.1.6 Phyllanthus emblica (Amla)
Amla extract (500 mg twice daily) significantly reduced fasting glucose, HbA1c, total cholesterol, and LDL-C in T2DM patients after 12 weeks, along with increased antioxidant enzyme activity (SOD, catalase) [49].
In hyperlipidemic subjects, 1 g/day amla powder for 45 days led to a 17% reduction in total cholesterol and a 21% drop in LDL [50].
5.1.7 Berberis aristata (Berberine Source)
Clinical studies comparing berberine (500 mg thrice daily) with metformin (500 mg thrice daily) in Type 2 diabetics showed comparable efficacy in reducing fasting glucose, HbA1c, and triglycerides [51].
Furthermore, berberine reduced total cholesterol and LDL-C through upregulation of LDL receptors [52].
5.1.8 Terminalia arjuna
Patients receiving T. Arjuna bark extract (500 mg twice daily for 12 weeks) showed reduced total cholesterol, LDL-C, and serum triglycerides, along with improved antioxidant capacity and endothelial function [53].
Another study reported improvement in fasting glucose and insulin sensitivity indices in diabetic subjects [54].
5.1.9 Camellia sinensis (Green Tea)
A clinical trial in 60 patients with metabolic syndrome demonstrated that daily consumption of green tea catechins (600 mg/day) reduced body weight, LDL-C, and fasting glucose levels [55].
A meta-analysis further validated significant improvements in total cholesterol and HbA1c among habitual green tea drinkers [56].
5.2 Polyherbal Formulations and Synergistic Clinical Effects
The combination of multiple herbs in formulations enhances efficacy via synergistic mechanisms:
Triphala (mixture of Terminalia chebula, Terminalia bellerica, Phyllanthus emblica) improved lipid and glucose levels through antioxidant and AMPK-mediated effects [57].
Diasulin (formulation containing Gymnema sylvestre, Momordica charantia, Syzygium cumini, Trigonella foenum-graecum) showed significant reductions in FPG, HbA1c, and triglycerides in human studies [58].
Herbal combinations with Curcuma longa and Allium sativum demonstrated additive effects in reducing LDL-C and oxidative stress [59].
These findings underline the multi-targeted and synergistic therapeutic potential of herbal formulations in managing diabetes and dyslipidemia simultaneously.
Table 3. Summary of Key Clinical Trials on Herbal Remedies
|
Herb/ Formulation |
Sample Size / Duration |
Dose / Extract Used |
Major Findings |
Clinical Outcome |
|
Gymnema sylvestre |
60 / 20 weeks |
400 mg/day extract |
↓ FPG, HbA1c, LDL |
Improved glycemic control |
|
Momordica charantia |
100 / 16 weeks
|
2,000 mg/day extract |
↓ FPG, TG, HbA1c |
Enhanced lipid & glucose profile |
|
Trigonella foenum-graecum |
80 / 8 weeks
|
10 g/day seed powder |
↓ TC, TG, HbA1c |
Hypolipidemic & hypoglycemic |
|
Curcuma longa |
100 / 12 weeks |
500 mg BID |
↓ FPG, LDL, MDA |
Improved insulin sensitivity |
|
Allium sativum |
Meta-analysis (26 trials) |
600–1,500 mg/day |
↓ FPG, LDL, ↑ HDL |
Consistent lipid & glucose lowering |
|
Phyllanthus emblica |
60 / 12 weeks |
500 mg BID |
↓ FPG, TC, LDL, ↑ SOD |
Dual effect validated |
|
Berberis aristata |
100 / 12 weeks
|
500 mg TID |
↓ TG, LDL, HbA1c |
Comparable to metformin |
|
Terminalia arjuna |
50 / 12 weeks |
500 mg BI |
↓ LDL, ↓ TG |
Improved vascular function |
|
Camellia sinensis |
60 / 8 weeks
|
600 mg/day catechins |
↓ FPG, ↓ LDL |
Metabolic improvement |
|
Polyherbal (Diasulin) |
120 / 12 weeks |
2 capsules/day |
↓ HbA1c, ↓ TG |
Synergistic activity |
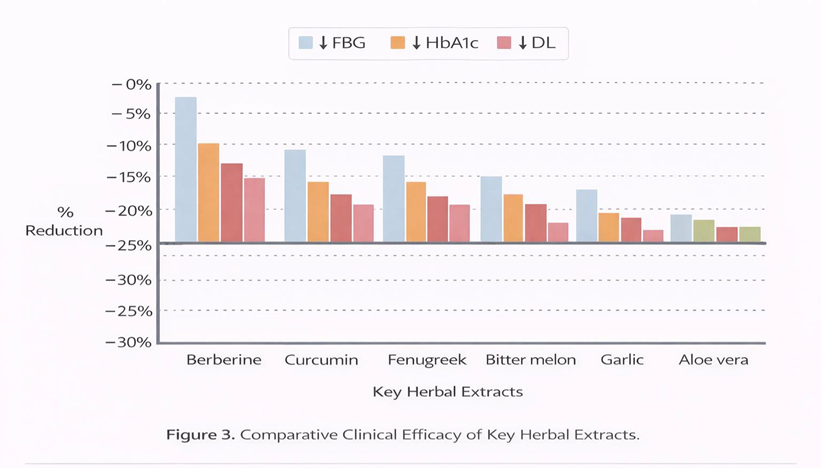
Figure 3: Comparative Clinical Efficiency of Key Herbal Extracts
6. Herbal Formulations and Synergistic Effects
Herbal medicine often relies on the synergistic action of multiple phytoconstituents that complement each other’s therapeutic targets. This synergy is crucial in the management of complex metabolic disorders such as diabetes and dyslipidemia, where multi-organ regulation is required.
6.1 Concept of Synergy in Herbal Therapeutics
Synergy in herbal medicine can occur through several mechanisms:
6.2 Traditional Polyherbal Formulations with Dual Actions
6.2.1 Diasulin
A well-known Ayurvedic formulation containing Gymnema sylvestre, Momordica charantia, Syzygium cumini, and Trigonella foenum-graecum.
Clinical studies show it significantly reduces HbA1c, FPG, TG, and LDL, while increasing HDL and improving antioxidant enzyme activity [63].
Mechanisms: α-glucosidase inhibition, AMPK activation, pancreatic β-cell regeneration, and oxidative stress reduction.
6.2.2 Triphala
Triphala is a classical polyherbal formulation comprising Terminalia chebula, Terminalia bellerica, and Phyllanthus emblica.
It exhibits strong antioxidant and hypolipidemic properties, reducing total cholesterol and triglycerides, and improving insulin sensitivity in obese and diabetic subjects [64].
Mechanisms: ROS scavenging, lipid metabolism modulation, and PPAR-γ activation.
6.2.3 Dihar and Glymin
Both are modern formulations combining herbs like Momordica charantia, Trigonella foenum-graecum, Gymnema sylvestre, and Pterocarpus marsupium.
Clinical data indicate improved glycemic control, lipid reduction, and enhanced insulin sensitivity when used adjunctively with oral antidiabetic drugs [65].
Mechanisms: Enzyme inhibition, GLUT4 translocation, and AMPK activation.
6.3 Herb–Drug Combinations
Several studies indicate that herbal agents can enhance or complement conventional drugs:
This highlights the emerging concept of integrative therapy, combining phytochemicals with standard pharmacotherapy for improved efficacy and reduced side effects.
6.4 Nanotechnology-Based Herbal Delivery Systems
One limitation of herbal therapeutics is poor bioavailability of active constituents due to low solubility and rapid metabolism. Recent research focuses on nanoformulations, which improve stability, targeted delivery, and pharmacological potency.
Examples of Nanocarriers in Herbal Hypolipidemic and Anti-Diabetic Agents:
|
Herbal Compound |
Nanoformulation Type |
Advantages |
Therapeutic Outcome |
|
Curcumin (Curcuma longa) |
Liposomes, polymeric nanoparticles |
↑ Bioavailability, controlled release |
Enhanced glucose and lipid reduction |
|
Berberine (Berberis aristata) |
Solid lipid nanoparticles |
↑ Cellular uptake, ↓ GI degradation |
Improved AMPK activation |
|
Gymnemic acid (Gymnema sylvestre) |
Nanomicelles |
↑ Intestinal absorption |
Improved hypoglycemic efficacy |
|
EGCG (Camellia sinensis) |
Nanoliposomes |
Stabilized antioxidant activity |
↓ LDL oxidation, ↓ FPG |
|
Trigonelline (Trigonella foenum-graecum) |
Chitosan nanoparticles |
Enhanced intestinal residence time |
↓ HbA1c, ↓ LDL-C |
Such innovations provide opportunities to translate traditional herbal medicines into scientifically validated, pharmacologically optimized therapeutics.
6.5 Synergistic Mechanistic Overview
Polyherbal formulations act through multiple converging pathways:
The result is restored metabolic homeostasis, improving both glucose and lipid profiles simultaneously.
While herbal remedies offer safer alternatives to synthetic agents, safety evaluation and standardization are essential to ensure therapeutic consistency and minimize adverse reactions.
7.1 Safety Profile of Key Herbal Agents
Extensive toxicological evaluations have shown that most hypolipidemic and anti-diabetic herbs are safe within therapeutic ranges. Acute and chronic toxicity studies generally report no mortality, organ damage, or mutagenic effects at recommended doses.
Table 4: Safety Profile of Key Herbal Agents.
|
Herbs |
Toxicity Findings (Animal/ Human Studies) |
Safe Dose Range |
Reported Adverse Effects |
|
Gymnema sylvestre
|
Non-toxic up to 1 g/kg (rat); no hepatic or renal toxicity [69] |
400–800 mg/day |
Mild gastric discomfort |
|
Momordica charantia
|
Safe up to 2 g/day; rare hypoglycemia at high doses [70] |
500–2000 mg/day |
Bitter taste, mild GI upset |
|
Trigonella foenum-graecum |
LD?? > 5 g/kg; mild bloating reported [71] |
5–10 g/day |
Flatulence, mild diarrhea |
|
Curcuma longa |
Non-toxic up to 8 g/day; well tolerated [72] |
500–2000 mg/day |
None significant |
|
Allium sativum |
Mild GI irritation at >2 g/day; safe for chronic use [73] |
600–1500 mg/day |
Odor, gastric irritation |
|
Phyllanthus emblica |
Safe up to 2 g/day; no hepatic or renal toxicity [74] |
500–1000 mg/day |
None significant |
|
Berberis aristata |
Mild constipation at high doses (>1.5 g/day) [75] |
500–1000 mg/day |
GI discomfort |
|
Terminalia arjuna |
Safe up to 1 g/day; cardioprotective profile [76] |
250–500 mg/day |
None reported |
Overall, toxicity indices (LD?? > 5 g/kg in most cases) and absence of mutagenic or genotoxic potential confirm high safety margins for most herbal agents used in metabolic disorders.
7.2 Herb–Drug Interactions
Some herbal compounds may interact with conventional drugs, altering pharmacokinetics or pharmacodynamics.
Berberine can inhibit CYP3A4 and P-glycoprotein, potentially affecting the metabolism of statins and metformin [77].
Curcumin and Piperine enhance bioavailability of co-administered drugs, sometimes requiring dose adjustment [78].
Allium sativum may potentiate antiplatelet and anticoagulant effects of aspirin or warfarin [79].
Gymnema sylvestre and Momordica charantia may cause additive hypoglycemia when combined with insulin or sulfonylureas [80].
Therefore, concurrent use with allopathic medications should be under pharmacist and clinician supervision, especially in polypharmacy cases.
7.3 Standardization and Quality Control
Quality assurance of herbal preparations is critical due to the variability in phytochemical content, influenced by geographical, seasonal, and processing factors.
The WHO and various pharmacopoeias recommend standardized quality parameters:
Adherence to Good Agricultural and Collection Practices (GACP) and Good Manufacturing Practices (GMP) ensures reproducibility, safety, and therapeutic efficacy [81–82].
7.4 Regulatory Aspects of Herbal Medicines
Global frameworks governing herbal product approval vary but share the goal of ensuring safety, efficacy, and quality.
|
Region |
Regulatory Agency / Guideline |
Framework Focus |
|
India |
Ministry of AYUSH, Drugs and Cosmetics Act 1940 |
Licensing, GMP certification, pharmacovigilance |
|
USA |
FDA (Dietary Supplement Health and Education Act, DSHEA 1994) |
Labeling, safety, post-market surveillance |
|
China |
EMA (Committee on Herbal Medicinal Products, HMPC) |
Traditional use registration, quality dossier |
|
Europe |
National Medical Products Administration (NMPA) |
Integration of TCM and modern drug evaluation |
|
WHO |
WHO Guidelines for the Assessment of Herbal Medicines (2000) |
Global safety, quality, and efficacy standards |
The increasing number of pharmacovigilance programs and quality audits worldwide reflects growing recognition of herbal medicines as legitimate therapeutic options in metabolic disorders [83].
7.5 Toxicological Risk Mitigation Strategies
To ensure patient safety:
Integration of these practices can help bridge traditional knowledge with modern pharmacological safety standards.
8. Future Prospects, Challenges, and Research Gaps
8.1 Current Challenges in Herbal Therapeutics
Despite strong traditional and clinical support, the integration of herbal remedies into mainstream therapy faces multiple challenges:
Variability in phytochemical composition due to different geographical, harvesting, and extraction conditions limits reproducibility [84].
Absorption, distribution, metabolism, and excretion (ADME) profiles of many active phytochemicals (e.g., gymnemic acids, saponins) remain poorly characterized [85].
Contamination with heavy metals, microbial toxins, or substitution with incorrect plant species can compromise safety [86].
Many studies have short durations (<3 months) and small sample sizes, restricting generalizability [87].
Polyherbal and combined therapies need systematic evaluation of potential adverse interactions [88].
8.2 Emerging Research Trends
8.2.1 Omics-Based Phytopharmacology
The use of genomics, proteomics, and metabolomics enables identification of novel targets and biomarkers for herbal efficacy and toxicity.
Systems biology approaches can map multi-target networks of phytochemicals, helping elucidate complex pharmacodynamics [89].
8.2.2 Molecular Docking and Computational Modeling
In silico screening allows virtual identification of phytochemicals that can bind with metabolic targets like AMPK, PPAR-γ, α-glucosidase, and HMG-CoA reductase.
This aids in prioritizing compounds for in vitro and in vivo studies, saving both time and resources [90].
8.2.3 Nano-Phytomedicine and Targeted Delivery
Nanocarriers (liposomes, nanoparticles, nanoemulsions) enhance bioavailability and target-site specificity of poorly soluble compounds like curcumin and berberine [91].
This strategy ensures sustained release, better tissue distribution, and improved patient compliance.
8.2.4 Synergistic and Multi-Omic Polyherbal Design
Future research is shifting toward rational design of synergistic formulations based on computational synergy mapping and network pharmacology models.
Machine learning algorithms can predict optimal herbal combinations for dual glucose–lipid regulation [92].
8.2.5 Gut Microbiota Modulation as a Therapeutic Axis
Emerging evidence suggests herbal polyphenols modulate gut flora composition, enhancing SCFA production and improving insulin sensitivity.
Targeting the gut–liver–pancreas axis may represent a novel therapeutic pathway for combined metabolic management [93].
8.3 Regulatory and Industrial Perspectives
Globalization of herbal medicines demands harmonized regulatory frameworks.
The integration of Ayurveda and modern pharmacology under evidence-based guidelines is accelerating.
International collaborations between research institutions and industries are enabling clinical translation and formulation innovation.
The phytopharmaceutical category under Indian regulations (2015) now allows the marketing of standardized herbal drugs with modern data packages [94].
Industrial research focuses on:
8.4 Research Gaps and Future Directions
|
Research Area |
Current Gap |
Future Direction |
|
Standardization |
Lack of universal reference markers |
Develop global phytochemical fingerprint databases |
|
Pharmacokinetics |
Limited ADME data |
Conduct in vivo and PBPK modeling for major phytochemicals |
|
Mechanistic Understanding |
Focus on single pathways |
Expand to multi-omics and systems pharmacology approaches |
|
Clinical Evidence |
Small-scale, short-duration trials |
Long-term, multi-center RCTs with larger cohorts |
|
Herb–Drug Interactions |
Insufficient pharmacovigilance data |
Develop herbal–drug interaction databases |
|
Formulation Science |
Low bioavailability |
Implement nanoformulation and transdermal technologies |
|
Regulatory Policy |
Inconsistent global standards |
Harmonize WHO, EMA, FDA, and AYUSH frameworks |
8.5 Vision for the Future
The future of herbal anti-diabetic and hypolipidemic therapy lies in integrative, evidence-based medicine, combining:
Such a holistic approach can revolutionize metabolic disorder management, providing safer, multi-targeted, and sustainable therapeutic options.
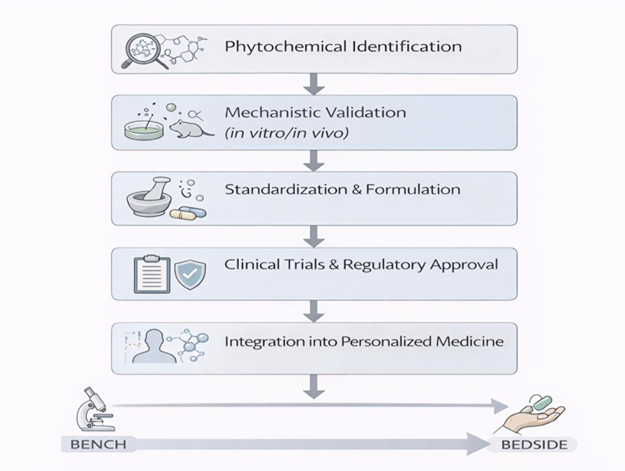
Figure 4: Roadmap for Future Research and Innovation in Herbal Hypolipidemic and Anti-Diabetic Therapy.
Herbal medicines represent a promising and sustainable alternative for managing diabetes mellitus and dyslipidemia, two interlinked metabolic disorders driven by insulin resistance, oxidative stress, and inflammation. A diverse range of plant species—such as Gymnema sylvestre, Trigonella foenum-graecum, Momordica charantia, Curcuma longa, and Berberis aristata—have demonstrated multi-targeted therapeutic effects, combining hypoglycemic, hypolipidemic, antioxidant, and anti-inflammatory mechanisms.
9.1 Integrated Mechanistic Insights
The collective evidence supports that herbal bioactives modulate multiple metabolic pathways simultaneously:
Such pleiotropic actions make herbal interventions more holistic compared to single-target synthetic agents [95–96].
9.2 Clinical and Translational Relevance
Multiple human clinical trials have validated the efficacy of herbal agents in lowering HbA1c, fasting glucose, triglycerides, and LDL-C while raising HDL-C.
Standardized extracts of Berberis aristata (berberine), Curcuma longa (curcumin), and Momordica charantia have shown comparable or synergistic benefits alongside conventional therapies like metformin and statins.
However, the clinical translation of these findings requires:
9.3 Industrial and Pharmaceutical Implications
With the global shift toward green therapeutics and natural product drug discovery, phytopharmaceuticals are being recognized under national drug policies (e.g., India’s AYUSH Phytopharmaceutical Regulations 2015 and EMA’s Traditional Use Registration Scheme).
This opens new opportunities for:
These innovations are paving the way for the next generation of herbal-based metabolic modulators [99].
9.4 Future Perspective
The convergence of traditional knowledge and modern technology—including omics, AI-driven synergy mapping, and targeted nanodelivery—is expected to reshape the therapeutic landscape of metabolic disorders.
By addressing key research gaps in standardization, quality control, and clinical validation, herbal remedies could soon form a cornerstone of integrative medicine.
The ideal therapeutic paradigm will blend:
9.5 Concluding Statement
Herbal remedies with hypolipidemic and anti-diabetic activities embody the essence of holistic, multi-targeted, and biocompatible medicine. Their ability to simultaneously modulate lipid and glucose metabolism through diverse molecular pathways underscores their clinical potential in the global fight against metabolic syndrome.
Future research integrating phytochemistry, nanotechnology, and clinical pharmacology will be crucial to unlocking the full therapeutic promise of these botanical agents.
REFERENCES

Ritesh Dhas, Vivek Desai, Harshal Wale, Swapnil Sande, Aniket Malekar, Herbal Remedies with Hypolipidemic and Anti-Diabetic Activities: Mechanisms and Clinical Evidence, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 1871-1890. https://doi.org/10.5281/zenodo.18301718
 10.5281/zenodo.18301718
10.5281/zenodo.18301718