KLR Pharmacy College, Telangana, India
Background: Hypertension frequently coexists with chronic comorbid conditions, necessitating tailored antihypertensive therapy to optimize clinical outcomes. In hospitalized patients, therapeutic decisions are often influenced by the presence of metabolic and cardiovascular disorders, yet prescribing patterns in such settings remain insufficiently characterized. This study aimed to evaluate the influence of comorbidities on antihypertensive drug selection and utilization, and to examine changes in blood pressure control during hospitalization. Methods: A hospital-based observational study was conducted among 298 hypertensive inpatients admitted to SCCL Main Hospital, Kothagudem. Demographic details, clinical history, lifestyle factors, comorbid conditions, laboratory findings, and antihypertensive prescriptions were systematically documented. Statistical analyses, including Chi-square test, one-way ANOVA, and Pearson’s correlation, were performed to determine associations between duration of hypertension, comorbidity burden, and prescribing patterns. Results: The mean age of participants was 58.05 ± 9.44 years, with comparable representation of both genders. A substantial proportion had longstanding hypertension (mean duration: 11.25 years) and positive family history. Telmisartan was the most frequently prescribed agent (87.2%), followed by metoprolol (40.9%) and amlodipine (18.5%). Angiotensin receptor blockers and beta-blockers were preferentially prescribed in patients with diabetes mellitus, ischemic heart disease, and chronic kidney disease (p < 0.05). Longer disease duration demonstrated a significant association with complex therapeutic regimens and inadequate blood pressure control. Hospitalization resulted in a statistically significant reduction in uncontrolled hypertension at discharge (p = 0.002). Conclusion: Antihypertensive prescribing in hospitalized patients is strongly influenced by coexisting comorbidities. Although short-term improvement in blood pressure was observed during admission, sustained outpatient strategies are essential for long-term control
INTRODUCTION
Hypertension is a major public health challenge and remains one of the leading contributors to global cardiovascular morbidity and premature mortality. Current epidemiological data estimate that over one billion adults worldwide are affected, with a steadily increasing burden in developing countries [1]. In India, the prevalence of hypertension has shown a consistent upward trend, particularly among urban populations and aging individuals [2]. Persistent elevation of blood pressure significantly increases the risk of coronary artery disease, stroke, heart failure, peripheral vascular disease, and chronic kidney disease, thereby imposing substantial clinical and economic strain on healthcare systems [3]. Effective management of hypertension requires sustained pharmacological intervention alongside lifestyle modification. However, achieving optimal blood pressure control remains difficult in real-world settings. Multiple studies have demonstrated that a considerable proportion of treated patients fail to attain target blood pressure levels despite the availability of effective antihypertensive agents [4]. Poor control may be attributed to factors such as therapeutic inertia, polypharmacy, medication non-adherence, socioeconomic barriers, and the presence of coexisting chronic illnesses [5]. The coexistence of hypertension with other chronic conditions is common, particularly in hospitalized populations. Diabetes mellitus, chronic kidney disease, ischemic heart disease, dyslipidemia, and heart failure frequently coexist and substantially alter cardiovascular risk profiles [6]. These comorbidities necessitate individualized drug selection based on organ-protective effects, pharmacodynamic considerations, contraindications, and potential drug–drug interactions [7]. For instance, angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs) are preferred in patients with diabetic nephropathy due to their renoprotective properties, whereas beta-blockers are often indicated in ischemic heart disease and post-myocardial infarction patients [8]. Guideline-directed medical therapy emphasizes tailoring antihypertensive treatment according to associated comorbidities and overall cardiovascular risk assessment [9]. International recommendations, including those from the American College of Cardiology/American Heart Association (ACC/AHA) and the European Society of Cardiology (ESC), advocate combination therapy in patients with long-standing or uncontrolled hypertension, particularly when target organ damage or metabolic disorders are present [10]. Despite these recommendations, variations in prescribing practices are frequently observed across healthcare institutions due to physician preferences, institutional protocols, and patient-specific characteristics [11]. Hospitalization provides a unique opportunity to evaluate and optimize antihypertensive therapy. During inpatient care, blood pressure is closely monitored, laboratory investigations are updated, and medication regimens are reassessed. Adjustments may be necessary to address uncontrolled hypertension, acute clinical deterioration, electrolyte imbalance, renal impairment, or adverse drug reactions [12]. However, limited published data specifically examine how comorbidities influence antihypertensive drug selection in hospitalized patients, particularly in tertiary care settings in India. Drug utilization studies are essential tools in evaluating rational prescribing patterns and assessing adherence to clinical guidelines. Such studies help identify gaps in evidence-based practice, patterns of polypharmacy, and potential areas for intervention to improve therapeutic outcomes [13]. In the context of hypertension, analyzing prescribing trends in relation to comorbidity burden can provide insights into whether therapy aligns with current recommendations and whether individualized treatment goals are being achieved [14]. Given the growing prevalence of multimorbidity and the increasing complexity of inpatient care, it is crucial to understand how coexisting conditions shape antihypertensive drug utilization. Therefore, the present observational study was designed to assess the impact of comorbidities on antihypertensive drug selection and utilization patterns among hospitalized patients, and to evaluate associations between disease duration, comorbidity burden, and blood pressure control during hospital stay.
MATERIALS AND METHODS
Study Design and Objectives
This prospective, observational, hospital-based study was designed to evaluate the influence of co-morbid conditions on the selection and utilization patterns of antihypertensive medications among hospitalized patients. The study aimed to examine how associated chronic illnesses affect clinical decision-making, assess adherence to established hypertension management guidelines, and identify patterns of rational or potentially inappropriate prescribing in the inpatient setting.
The primary objectives were to determine the prevalence of hypertension among hospitalized patients with comorbidities and to analyze antihypertensive drug utilization patterns in relation to specific coexisting conditions such as diabetes mellitus, chronic kidney disease, heart failure, ischemic heart disease, and cerebrovascular disease. Secondary objectives included evaluating concordance of prescribing practices with recognized clinical guidelines (JNC-8, ESC/ESH, ACC/AHA), identifying potential drug–drug interactions or adverse drug reactions, assessing the role of multidisciplinary care including clinical pharmacists, and formulating recommendations to improve individualized pharmacotherapy in complex hospitalized patients.
Study Setting
The study was conducted in a tertiary care teaching hospital with dedicated departments of General Medicine and Cardiology. The hospital maintains structured inpatient medical records and a functional Hospital Management System (HMS), which facilitates comprehensive and systematic data collection.
Study Duration
Data collection was carried out over a period of six months to ensure adequate representation of prescribing trends and clinical outcomes across a diverse inpatient population.
Study Population
The study population comprised hospitalized adult patients diagnosed with primary hypertension and at least one documented co-morbid condition. Eligible participants were identified through inpatient case records and physician documentation.
Inclusion Criteria
Exclusion Criteria
Data Collection Procedure
Data were collected prospectively using a standardized data collection form developed specifically for the study. Information was obtained from inpatient case records, laboratory reports, medication charts, and physician notes.
The following variables were documented:
Demographic Characteristics
Age, gender, body mass index (BMI), smoking status, alcohol consumption, and family history of hypertension.
Clinical Characteristics
Duration of hypertension, type and number of comorbid conditions, history of prior antihypertensive therapy, and concurrent medications.
Drug Utilization Patterns
Class of antihypertensive agents prescribed (ACE inhibitors, ARBs, beta-blockers, calcium channel blockers, diuretics, or combination therapy), changes in therapy during hospitalization, and rationale for drug selection in relation to comorbidity profile.
Clinical Outcomes
Blood pressure measurements at admission and discharge, occurrence of adverse drug reactions (ADRs), need for therapeutic modification, length of hospital stay, and readmissions (if applicable).
Laboratory Parameters
Serum creatinine, fasting blood glucose, lipid profile, serum electrolytes, and other relevant biochemical indicators were recorded to assess organ function and therapeutic appropriateness.
All collected data were anonymized and coded to maintain patient confidentiality.
Ethical Considerations
The study protocol was reviewed and approved by the Institutional Ethics Committee prior to initiation. Written informed consent was obtained from all participants. Confidentiality was strictly maintained by de-identifying patient information and securing data access to authorized investigators only. The study adhered to ethical principles outlined in the Declaration of Helsinki.
Statistical Analysis
Data were entered into a validated statistical software package (SPSS version XX or R software) for analysis.
A p-value less than 0.05 was considered statistically significant.
Expected Outcomes
The study was designed to generate real-world evidence regarding antihypertensive prescribing practices in hospitalized patients with multiple comorbidities. It aimed to:
RESULTS AND DISCUSSION
This section provides a detailed analytical presentation of the findings derived from the evaluation of 298 hospitalized patients diagnosed with primary hypertension. The results are systematically organized to reflect demographic characteristics, clinical profiles, comorbidity burden, and antihypertensive prescribing patterns observed within the inpatient setting. Data are presented through structured tables and graphical representations to facilitate clarity, transparency, and reproducibility of findings. The analysis specifically focuses on understanding how coexisting medical conditions—including diabetes mellitus, chronic kidney disease, ischemic heart disease, heart failure, cerebrovascular disease, and other chronic disorders—shape therapeutic decision-making in hospitalized hypertensive patients. Particular attention is given to the relationship between comorbidity profiles and the selection of antihypertensive drug classes, thereby evaluating the extent to which prescribing practices are aligned with contemporary evidence-based clinical guidelines. In addition to comorbidity-driven prescribing trends, the study examines other clinically relevant determinants such as duration of hypertension, lifestyle-related risk factors (including tobacco and alcohol use), and laboratory parameters indicative of organ function. These variables are analyzed in relation to therapeutic complexity, drug selection, and short-term blood pressure outcomes during hospitalization. The discussion integrates statistical findings with current scientific literature and international hypertension management recommendations. Emphasis is placed on identifying rational prescribing patterns, potential areas of therapeutic optimization, and implications for individualized pharmacotherapy in patients with multimorbidity. By situating the results within a broader clinical and epidemiological context, this section aims to generate meaningful insights that contribute to improved inpatient hypertension management and multidisciplinary care strategies.
Baseline Characteristics of the Study Population
Table 1. Demographic and Lifestyle Characteristics (n = 298)
|
Variable |
Category |
Frequency (n) |
Percentage (%) |
|
Age |
>60 years |
161 |
54.0 |
|
51–60 years |
85 |
28.5 |
|
|
≤50 years |
52 |
17.4 |
|
|
Mean Age |
58.05 ± 9.44 years |
||
|
Gender |
Male |
148 |
50.3 |
|
Female |
150 |
49.7 |
|
|
Smoking |
Current |
75 |
24.9 |
|
Alcohol Use |
Current |
84 |
28.2 |
|
Family History |
Positive |
169 |
56.7 |
The study cohort was predominantly elderly, with more than 80% aged 50 years or older (mean age 58.05 ± 9.44 years), Table 1. The age distribution is consistent with the epidemiological pattern of hypertension increasing with advancing age due to progressive vascular stiffness and endothelial dysfunction [15]. Gender distribution was nearly equal, minimizing sex-related sampling bias. Approximately one-quarter of patients were current smokers, and 28% reported alcohol consumption, both recognized cardiovascular risk amplifiers [16]. More than half of the cohort reported a positive family history, indicating a substantial hereditary component in disease susceptibility [17].
Prevalence of Hypertension with Associated Comorbidities
Table 2 & Figure 1 demonstrate a substantial burden of comorbidity among hospitalized hypertensive patients, with diabetes mellitus emerging as the most prevalent associated condition (81.2%). This high coexistence reflects the well-recognized pathophysiological interaction between hypertension and metabolic dysfunction. Insulin resistance, endothelial impairment, oxidative stress, and persistent activation of the renin–angiotensin–aldosterone system collectively contribute to the bidirectional relationship between these disorders [3]. The coexistence of diabetes significantly increases cardiovascular risk and accelerates microvascular and macrovascular complications, thereby necessitating intensified and individualized antihypertensive management strategies. Coronary artery disease (CAD), with or without heart failure, was observed in nearly half of the study population (49.3%). Hypertension is a principal modifiable determinant of atherosclerosis and myocardial remodeling. Chronic elevation of blood pressure promotes arterial stiffness, endothelial injury, and left ventricular hypertrophy, ultimately predisposing individuals to ischemic events and cardiac dysfunction [9,10]. The high prevalence of CAD in this cohort underscores the cumulative cardiovascular burden associated with prolonged uncontrolled hypertension.Chronic kidney disease (7.4%) and stroke (14.4%) further illustrate the systemic consequences of sustained hypertension. Hypertensive nephrosclerosis remains a major contributor to progressive renal impairment worldwide, while uncontrolled systolic hypertension is a dominant risk factor for both ischemic and hemorrhagic stroke [18,19]. Even though CKD prevalence in this cohort was comparatively lower than that of diabetes and CAD, its presence carries important therapeutic implications, particularly regarding drug selection and dosage adjustment. Chronic obstructive pulmonary disease (11.4%) was also identified, reflecting the coexistence of cardiopulmonary conditions in a subset of patients. Although COPD does not share a direct mechanistic pathway with hypertension to the same extent as metabolic disorders, systemic inflammation, endothelial dysfunction, and shared behavioural risk factors such as smoking may contribute to overlapping disease patterns [20]. Importantly, more than half of the patients (56.3%) exhibited two or more comorbidities, indicating a high degree of multimorbidity. Multimorbidity substantially complicates pharmacotherapeutic decisions, increases the risk of polypharmacy, and is associated with higher healthcare utilization and poorer long-term outcomes [21]. The presence of multiple chronic conditions necessitates a comprehensive, patient-centered approach that prioritizes risk reduction and individualized treatment planning. Overall, the findings of Table 2 confirm that hypertension in hospitalized patients rarely occurs in isolation. Instead, it is embedded within a broader cardiometabolic and systemic disease framework. The predominance of diabetes and cardiovascular conditions strongly supports a comorbidity-driven model of antihypertensive therapy, reinforcing the clinical rationale for tailored pharmacological selection in complex inpatient populations.
Table 2. Distribution of Major Comorbidities (n = 298)
|
Comorbidity |
Frequency (n) |
Percentage (%) |
|
Diabetes Mellitus |
242 |
81.2 |
|
CAD ± Heart Failure |
147 |
49.3 |
|
Chronic Kidney Disease |
22 |
7.4 |
|
Stroke |
43 |
14.4 |
|
COPD |
34 |
11.4 |
|
≥2 Comorbidities |
168 |
56.3 |
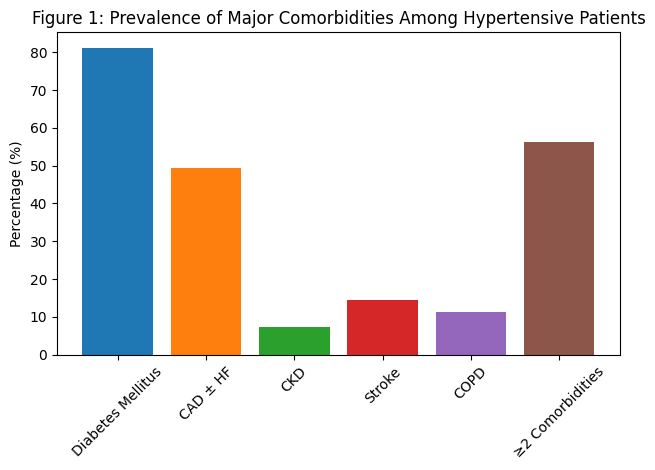
Figure 1: Prevalence of Major Comorbidities Among Hypertensive Patients
Duration of Hypertension and Treatment Complexity
The present analysis demonstrates that the mean duration of hypertension in the study population was 11.25 ± 7.86 years, indicating that a substantial proportion of patients had long-standing disease. More than half of the cohort had been hypertensive for over 10 years, reflecting chronic exposure to elevated arterial pressure and cumulative vascular stress Table 3 & Figure 2. The statistically significant association between disease duration and number of prescribed antihypertensive agents (ANOVA: F = 3.21, p = 0.014) suggests that therapeutic complexity increases with time. Patients with a hypertension history exceeding 15 years were more frequently managed with multidrug regimens. This observation aligns with the progressive nature of hypertension, wherein prolonged vascular remodeling, endothelial dysfunction, and neurohormonal activation reduce responsiveness to monotherapy, necessitating combination treatment to achieve target blood pressure levels [3]. Contemporary guidelines recommend early introduction of combination therapy in patients with persistent or resistant hypertension, particularly in those with long disease duration or target organ involvement [9,10]. The correlation analysis further strengthens this interpretation. A moderate positive correlation between duration of hypertension and systolic blood pressure (r = 0.298, p = 0.001) indicates that longer disease exposure is associated with poorer systolic control. The weaker but statistically significant correlation with diastolic blood pressure (r = 0.216, p = 0.003) suggests a similar, though less pronounced, trend. The stronger association with systolic pressure is clinically meaningful, as systolic hypertension is more strongly linked to arterial stiffness and age-related vascular changes [22]. Prolonged hypertension accelerates elastin degradation, collagen deposition, and large-artery stiffening, contributing to isolated systolic hypertension and reduced treatment responsiveness over time [23]. In addition to pathophysiological mechanisms, behavioral and therapeutic factors may also contribute to this pattern. Long-standing hypertensive patients may experience declining medication adherence, therapeutic inertia, or suboptimal dose titration in earlier disease stages, ultimately leading to more aggressive pharmacological escalation during hospitalization [5]. The observed treatment intensification in patients with extended disease duration therefore, reflects both biological progression and adaptive clinical response. Collectively, these findings confirm that hypertension is not a static disorder but a progressive condition requiring dynamic management strategies. Early diagnosis, timely therapy optimization, and regular monitoring are essential to prevent long-term vascular complications. The data emphasize that the duration of hypertension should be considered a key clinical determinant when designing individualized antihypertensive regimens in hospitalized patients.
Table 3. Duration of Hypertension
|
Duration (Years) |
Frequency |
Percentage |
|
≤5 |
70 |
23.5 |
|
6–10 |
93 |
31.2 |
|
11–15 |
62 |
20.8 |
|
16–20 |
28 |
9.4 |
|
>20 |
22 |
7.4 |
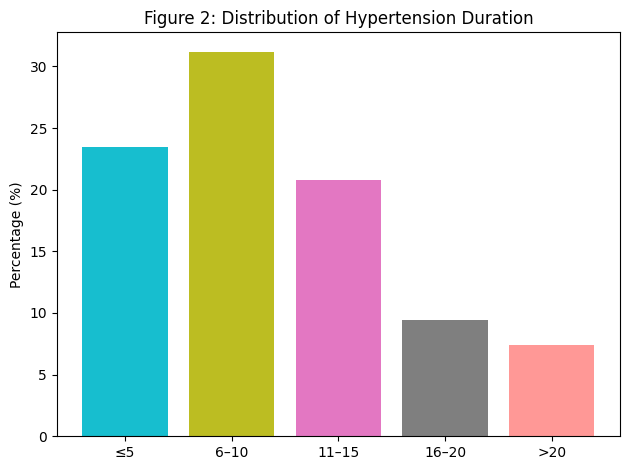
Figure 2: Distribution of Hypertension Duration
Antihypertensive Drug Utilization Patterns
The present findings demonstrate a clear predominance of angiotensin receptor blockers (ARBs), prescribed in 87.2% of patients, followed by beta blockers (40.9%) and calcium channel blockers (33.2%). The significantly higher use of ARBs suggests a strong comorbidity-driven prescribing approach rather than uniform first-line therapy across all patients. The statistically significant association between comorbidity presence and drug class selection (χ² = 30.6, p = 0.013) confirms that antihypertensive therapy was tailored according to individual clinical profiles Table 4 & Figure 3. Telmisartan emerged as the most frequently prescribed individual agent, reflecting its favorable pharmacokinetic profile, long half-life, and demonstrated cardiovascular and renal protective benefits. ARBs are widely recommended in patients with diabetes and chronic kidney disease due to their ability to reduce proteinuria, delay nephropathy progression, and provide vascular protection [24,25]. The comparatively lower use of ACE inhibitors may reflect concerns regarding tolerability, particularly cough and angioedema, leading to preference for ARBs in clinical practice [26]. Beta blockers were frequently prescribed, particularly in patients with ischemic heart disease and heart failure. Their role in reducing myocardial oxygen demand, improving survival in systolic heart failure, and preventing recurrent ischemic events justifies their substantial utilization [27]. Calcium channel blockers demonstrated moderate use, especially in patients without significant comorbidity burden, consistent with their effectiveness in controlling systolic hypertension and improving arterial compliance [28].
Table 4. Distribution of Antihypertensive Drug Classes
|
Drug Class |
Frequency (n) |
Percentage (%) |
|
ARBs |
260 |
87.2 |
|
Beta Blockers |
122 |
40.9 |
|
Calcium Channel Blockers |
99 |
33.2 |
|
Diuretics |
19 |
6.3 |
|
ACE Inhibitors |
5 |
1.7 |
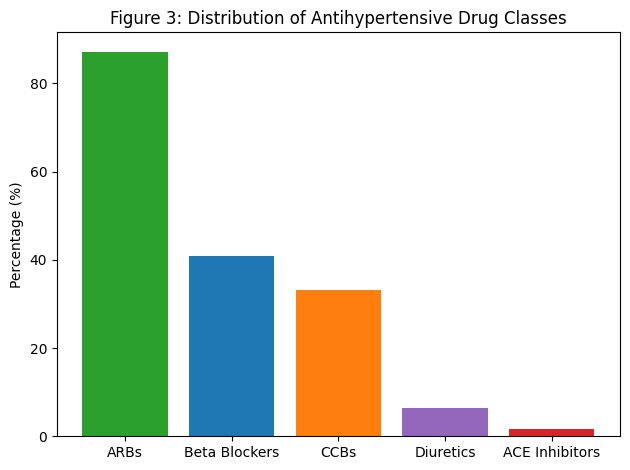
Figure 3: Distribution of Antihypertensive Drug Classes
Association Between Comorbidities and ARB Prescription
Logistic regression analysis provided robust evidence that diabetes mellitus and chronic kidney disease were the strongest independent predictors of ARB utilization. Patients with diabetes were approximately 2.5 times more likely to receive ARBs (OR 2.45), while those with CKD exhibited more than threefold increased odds (OR 3.12). Combined comorbidity states, such as CAD with CKD or CAD with diabetes and stroke, further strengthened the likelihood of ARB prescription Table 5 & Figure 4. These findings reflect adherence to contemporary evidence-based recommendations advocating RAAS blockade in patients with metabolic and renal complications [9,10]. The absence of statistically significant associations for COPD and isolated stroke suggests that ARB selection was primarily influenced by cardiovascular and renal considerations rather than respiratory comorbidity alone. This pattern reinforces the principle of individualized pharmacotherapy based on organ-specific risk profiles.
Table 5. Comorbidity as Predictor of ARB Prescription
|
Comorbidity |
χ² |
p-value |
Odds Ratio (95% CI) |
|
Diabetes Mellitus |
15.32 |
<0.001 |
2.45 (1.65–3.64) |
|
CAD + HF |
9.78 |
0.002 |
1.89 (1.22–2.93) |
|
CKD |
6.45 |
0.011 |
3.12 (1.29–7.55) |
|
DM + CAD |
12.25 |
<0.001 |
2.67 (1.70–4.20) |
|
CAD + CKD |
5.11 |
0.024 |
2.95 (1.14–7.63) |
|
CAD + DM + Stroke |
4.67 |
0.031 |
3.21 (1.11–9.29) |
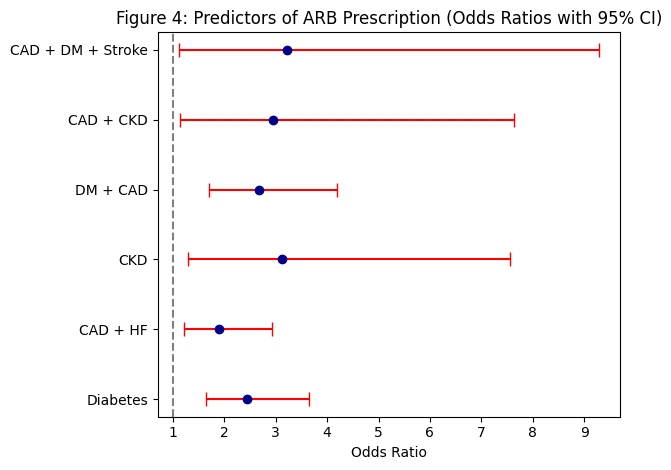
Figure 4: Prediction of ARB Prescription (Odds Ratios with 95% CI)
Guideline Concordance
The overall guideline adherence rate of 82.5% indicates substantial compliance with established hypertension management frameworks, including JNC-8, ACC/AHA 2017, and ESC/ESH 2018 guidelines. Partial concordance (11.7%) was largely attributable to dose adjustments rather than inappropriate drug class selection. Only a small proportion (5.8%) demonstrated deviation from recommended therapy Table 6. Such high concordance suggests rational prescribing behavior within the inpatient setting. Evidence-based hypertension management emphasizes comorbidity-driven drug selection and early combination therapy in high-risk patients [9,10]. The observed prescribing patterns appear consistent with these recommendations, indicating integration of guideline principles into routine clinical decision-making.
Table 6. Guideline Adherence
|
Category |
Frequency (n) |
Percentage (%) |
|
Fully Concordant |
246 |
82.5 |
|
Partially Concordant |
35 |
11.7 |
|
Non-Concordant |
17 |
5.8 |
Blood Pressure Changes from Admission to Discharge
A statistically significant improvement in blood pressure control was observed during hospitalization. The proportion of patients with uncontrolled BP (>130 mmHg) decreased from 88.0% at admission to 77.0% at discharge (p = 0.002), while those achieving near-normal BP (120–129/<80 mmHg) increased significantly (p < 0.001). Table 7 & Figure 5. These findings highlight hospitalization as an important opportunity for therapeutic optimization. Inpatient settings allow for medication titration, adherence reinforcement, and close hemodynamic monitoring, contributing to improved short-term BP stabilization [29]. The slight non-significant reduction in patients with BP <120/80 mmHg may reflect cautious avoidance of overly aggressive BP lowering, particularly in elderly or multimorbid individuals where hypotension risk must be minimized [30].
Table 7. Blood Pressure Distribution at Admission vs Discharge
|
BP Category |
Admission n (%) |
Discharge n (%) |
p-value |
|
<120/80 |
23 (7.6%) |
17 (5.6%) |
0.317 |
|
120–129/<80 |
13 (4.3%) |
52 (17.2%) |
<0.001 |
|
>130 |
265 (88.0%) |
232 (77.0%) |
0.002 |
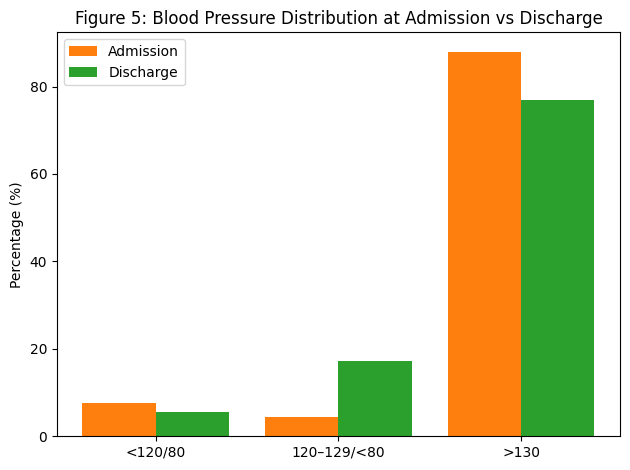
Figure 5: Blood Pressure Distribution at Admission Vs Discharge
Drug Safety and Polypharmacy
Nearly half of the cohort (48.9%) experienced polypharmacy, reflecting the high burden of multimorbidity. Polypharmacy was significantly associated with increased risk of potential drug–drug interactions (p = 0.021). However, clinically significant adverse drug reactions were documented in only 6.7% of patients, suggesting vigilant monitoring and relatively cautious prescribing practices Table 8 & Figure 6.
Multimorbid hypertensive patients are particularly vulnerable to pharmacodynamic interactions and altered drug clearance, especially when renal impairment coexists [31]. The relatively low ADR incidence in this study indicates effective clinical oversight and supports the importance of structured medication review protocols in inpatient care.
Table 8. Safety Profile
|
Variable |
Frequency |
Percentage |
|
Polypharmacy |
146 |
48.9 |
|
Potential Drug Interactions |
42 |
14.1 |
|
Clinically Significant ADRs |
20 |
6.7 |
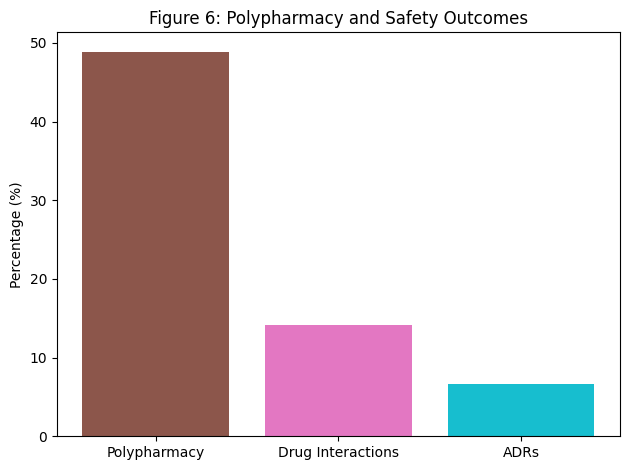
Figure 6: Polypharmacy and Safety Outcomes
Multidisciplinary Care Impact
Clinical pharmacist involvement was documented in 32% of complex cases and was associated with significantly improved blood pressure stabilization at discharge (p = 0.038). Multidisciplinary collaboration enhances medication reconciliation, optimizes dose titration, and reduces therapeutic inertia.
Evidence consistently demonstrates that team-based hypertension management improves BP control, medication adherence, and overall cardiovascular outcomes. The present findings reinforce the value of integrating pharmaceutical care services into inpatient cardiovascular management models.
CONCLUSION
This hospital-based observational study provides comprehensive insights into the influence of comorbid conditions on antihypertensive drug selection and utilization patterns among hospitalized patients. The findings demonstrate that hypertension in the inpatient setting rarely occurs in isolation and is frequently accompanied by metabolic and cardiovascular comorbidities, particularly diabetes mellitus and coronary artery disease. Antihypertensive prescribing patterns were predominantly comorbidity-driven, with angiotensin receptor blockers emerging as the most frequently utilized drug class, especially among patients with diabetes mellitus and chronic kidney disease. Logistic regression analysis confirmed that these comorbidities significantly predicted ARB prescription, indicating rational, evidence-aligned therapeutic decision-making. The high rate of guideline concordance further supports adherence to established hypertension management recommendations. The study also revealed that longer duration of hypertension was associated with greater treatment complexity and poorer systolic blood pressure control, emphasizing the progressive nature of the disease. Importantly, hospitalization served as a critical window for therapeutic optimization, resulting in statistically significant improvement in blood pressure levels at discharge. Although polypharmacy was common due to multimorbidity, the incidence of clinically significant adverse drug reactions remained relatively low, suggesting effective monitoring practices. Multidisciplinary involvement, particularly clinical pharmacist participation, was associated with improved blood pressure stabilization, highlighting the value of team-based care models in complex hypertensive populations.
Overall, the findings underscore the importance of individualized, comorbidity-oriented antihypertensive therapy, continuous monitoring, and collaborative clinical decision-making to optimize outcomes in hospitalized patients with hypertension.
ACKNOWLEDGMENT
The authors express their sincere gratitude to the management and medical staff of the participating hospital for their cooperation and support during the data collection process. Special appreciation is extended to the Department of Pharmacy Practice for providing academic guidance and facilitating access to clinical records necessary for the completion of this study. The authors also acknowledge the contributions of the clinical pharmacists and healthcare professionals whose collaboration enhanced the quality of patient care and enriched the study findings.
CONFLICT OF INTEREST
The authors declare that there are no financial, professional, or personal conflicts of interest that could have influenced the conduct, analysis, or reporting of this study. The research was carried out independently, and all interpretations are based solely on the collected data and established scientific evidence.
REFERENCES






K. Komali, P. Srikanth, A. Kavya, S. Mohana Sindu, M. Sowjanya, M. Naga Greeshma, Dr. C. R. Akila, Dr. M. Purushothaman, Impact of Co-Morbidities on Anti-Hypertensive Drug Selection and Utilization in Hospitalized Patients: An Observational Study, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 3472-3485. https://doi.org/10.5281/zenodo.18722706
 10.5281/zenodo.18722706
10.5281/zenodo.18722706
