
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
The Oxford College Of Pharmacy, 1st Cross, Hongasandra, Bengaluru, Karnataka 560068
Controlled and sustained drug administration has recently emerged as the norm in contemporary pharmaceutical design and a number of studies have been conducted to enhance the effectiveness, dependability, and safety of therapeutic products. One special feature of in situ gel systems is their ability to change from sol–gel in response to biological stimuli. In-situ gel is a drug delivery system where a sol is formed prior to being administered to the body and after delivery it gels in-situ. A lack of certain nutrients, such as iron, vitamins, particularly B12 and C, poor dental hygiene, infections, stress, indigestion, mechanical injury, food allergies, hormone imbalances, skin conditions, etc., are among the causes of mouth ulcers. Mouth ulcers are also known as canker sores. The primary function of polymers such as cellulose, pectin, and poloxamer in the body is to facilitate medication absorption through a variety of mechanisms. This review focused on definition and types of mouth ulcer, importance, advantages, disadvantages, mechanism and approaches of in-situ gel, polymers used, and suitable characteristics of polymers, including the method of preparation of in situ gels. Additionally, recent advances, applications, and evaluation of in situ gels were explained.
An ulcer that develops on the oral cavity's mucous membrane is known as a mouth ulcer, oral ulcer, or mucosal ulcer. These are uncomfortable round or oval mouth sores that mainly develop on the inside of the lips or cheeks. Although Mouth ulcers are a common condition and can arise from a variety of causes and in conjunction with numerous illnesses, there is typically no significant underlying cause. Nutritional deficiencies, particularly in iron and vitamins B12 and C, poor dental hygiene, infections, stress, indigestion, mechanical injury, food allergies, hormonal imbalances, skin conditions, etc., are common causes of mouth ulcers. Aphthous ulcers, another name for mouth ulcers, can hurt when you eat, drink, or wash your teeth.(1) The most common oral mucosal illness in humans, recurrent aphthous stomatitis, usually first manifests in childhood or adolescence and is also known as aphthous ulcers or canker sores. Aphthous ulcers are round or oval in shape, with a grayish yellow color that resembles a bowl encircled by mucosal inflammation. The non-keratinized oral mucosa, which includes the lips, buccal mucosa, bottom of the mouth, and therefore the ventral surface of the tongue, is where the ulcer typically develops inside the mouth.(2) One of the most prevalent conditions in the population is oral illness. They have an impact on people's quality of life and pose a significant financial and health burden. Dental cavities, tooth loss, lip and oral cancer, and periodontal illnesses including gingivitis are the most common. The efficacy of pharmacotherapy is negatively impacted by the administered dosage type and the administration method.(2)

Figure No.1: Mouth ulcer
TYPES OF MOUTH ULCER:
Herpetiform ulcers: This kind of ulcer is made up of several dozen tiny, pinhead-sized lesions.(3)

Figure No.2: Herpetiform ulcer
Traumatic Ulcers: A traumatic ulcer is the most prevalent kind of ulcer and is acute in nature. Causes of traumatic ulcers are physical, thermal, or chemical trauma to the oral mucosa, which can be brought on by routine activities like brushing or flossing, sharp edges of teeth or dentures, or self-harm by the patient while under local anesthesia during a dental procedure. Most common causes of thermal burns are hot food or beverages like pizza, coffee, or tea, or by a heated dental instrument during a dental procedure.(3)

Figure No.3: Traumatic ulcer
Primary Herpetic Gingivostomatitis: Primary herpetic gingivostomatitis is the most typical oral sign of a herpes simplex virus (HSV) infection. Over 90% of cases that happen above the waist are caused by HSV-1. Infection with HSV-2 happens below the waist. HSV-2 is frequently cultured from oral sores as a result of varying sexual practices. With a high incidence between two and three years, Usually, the age of occurrence falls between six months and five years. Prodromal symptoms include irritability, anorexia, fever, and nausea.(3)

Figure No. 4: Primary Herpetic Gingivostomatitis ulcer
Recurrent Aphthous Stomatitis (Canker sore): Hippocrates is credited with coining the term "aphthae," which comes from the Greek word "aphthi," which means "to set on fire" or "to inflame," to describe the agony associated with a common oral ailment at the time (possibly aphthous stomatitis). Common mouth ulcers have been linked to a number of etiological reasons, including immunological or endocrine disorders, bacterial and viral infections, dietary inadequacies, local damage, and hereditary factors. Some patients get recurrent aphthous stomatitis (RAS) when the cause is unclear. RAS is divided into three categories: herpetiform (10%), major (10%), and minor (> 70% of cases).These subcategories vary in their appearance, distribution, severity, and prognosis.(3)

Figure No.5: Recurrent Aphthous Stomatitis (Canker sore)
Traumatic Ulcerative Granuloma (Eosinophilic Ulcer of the Tongue) : Hippocrates is credited with coining the term "aphthae," which comes from the Greek word "aphthi," which means "to set on fire" or "to inflame," to describe the agony associated with a common oral ailment at the time (possibly aphthous stomatitis). Common mouth ulcers have been linked to a number of etiological reasons, including immunological or endocrine disorders, bacterial and viral infections, dietary inadequacies, local damage, and hereditary factors. Some patients get recurrent aphthous stomatitis (RAS) when the cause is unclear. RAS is divided into three categories: herpetiform (10%), major (10%), and minor (> 70% of cases). These subcategories vary in their appearance, distribution, severity, and prognosis.(3)

Figure No.6: Traumatic Ulcerative Granuloma
IN-SITU GEL:
The term "gel" comes from Gelu, which illustrates how liquid settles to create a semi-solid mixture. Gels consist of dispersions of tiny or large molecules in an aqueous liquid medium thickened with a gelling agent. They are transparent or translucent, non-greasy, semisolid systems. Gels may be a biphasic system or a single phase.(4)A growing number of in-situ forming systems for a range of biomedical uses, such as drug administration, cell encapsulation, and tissue repair, have been documented in the literature in recent years. These systems include of injectable fluids that can be minimally invasively injected into the body before they gel or solidify in the targeted tissue, organ, or bodily cavity.(5) The insitu gel phenomenon is based on a medication formulation in a liquid solution that is transformed into a semi-solid mucoadhesive key depot. It enables the medication to be administered as a liquid or solution.(6)
IMPORTANCE OF IN-SITU GEL:
ADVANTAGES OF IN-SITU GEL:
DISADVANTAGES OF IN-SITU GEL:
MECHANISM OF IN-SITU GEL:
Diffusion: The physical method known as Diffusion is employed in the formation of in-situ gels. This process involves the solvent from the polymer solution diffusing into the surrounding tissue, causing the polymer matrix to precipitate or solidify. N-methyl pyrrolidone (NMP) is a polymer that is frequently used to create in-situ gelling systems.(7)
Swelling: When substance absorbs water from their surroundings and expands to take up the desired space, in situ creation can also happen.(8)
Chemical reaction: Chemical reactions that can result in in situ gelation include enzymatic, photo-initiated, and precipitation of inorganic particles from supersaturated ionic liquids.
Ionic crosslinking: Phase transitions in polymers can occur when different ions are present. A subset of poly saccharides are classified as ion-sensitive. I-carrageenan primarily produces elastic gels in the presence of Ca2+, whereas k-carrageenan creates stiff, brittle gels in response to tiny amounts of K+. Commercially marketed as Gelrite, An anionic polysaccharide is gellan gum. that gels in situ when mono- and divalent cations such as Ca2+, Mg2+, K+, and Na+ are present. Divalent cations, particularly Ca2+, can induce the low-methoxy pectins to gel. Similarly, when divalent or polyvalent cations, such as Ca2+, are present, alginic acid gels because of its interaction with the guluronic acid block in alginate chains.(8)
Enzymatic cross-linking: The use of natural enzymes to catalyze in situ formation has not been thoroughly examined, but appears to have some benefits over chemical and photochemical approaches. For instance, an enzymatic process can function effectively in physiological settings without the use of potentially hazardous substances like initiators and monomers. Hydrogels with insulin-releasing capabilities have been used in intelligent stimuli-responsive administration devices. When blood glucose levels rise, cationic pH-sensitive polymers that contain immobilized insulin and glucose oxidase can swell, pulsatilely releasing the trapped insulin. The mixes can be administered prior to gel formation because varying the enzyme concentration also offers a practical way to regulate the rate of gel formation.(8)
Photo-polymerization: The in-situ gelling system is formed using electromagnetic radiation in the photo-polymerization process. Electromagnetic radiation can be utilized to create gel after injecting either a reactive macromere or monomer solution and intruder into a tissue location. The best polymers for photo polymerization are those that, when exposed to a photo initiator such as acrylate or a comparable monomer or macromer with a long wavelength (usually ultraviolet and visible), undergo dissociation by a polymerisable functional group. Due to their limited tissue penetration and potential biological injury, short wavelength ultraviolet light is not frequently used. This technique uses a ketone as the initiator for ultraviolet photo-polymerization, such as 2,2dimethoxy-2-phenyl acetophenone. In visible light systems, initiators such as camphor Quinone and ethyl eosin are employed.(8)
APPROACHES OF IN-SITU GEL:
There are some several Approaches used to obtain an in-situ gelation system.(9)
Temperature triggered in-situ gel: Temperature is the most widely used stimulus in in-situ gelling formulation for environmentally responsive polymer systems. Both in vitro and in vivo, the temperature change that is employed is simple to regulate and apply. Body warmth causes gelation in this system; external heat is not necessary. These hydrogels are liquid at normal temperature (20–25°C), but when they come into contact with bodily fluids (35–37°C), the temperature rises and causes them to gel. Three different kinds of temperature-induced systems exist. They are both positively and negatively thermosensitive, such as poly (nisopropylacrylamide) and thermally reversible polyacrylic acid. For instance, Tetronics, Plurionics, and Poloxamer. In this system, temperature-responsive or thermoresponsive polymers—which exhibit a sharp and abrupt change in their physical characteristics with temperature—are employed. There is a miscibility gap between these polymers at high and low temperatures, as well as an upper and lower critical solution temperature.(9)
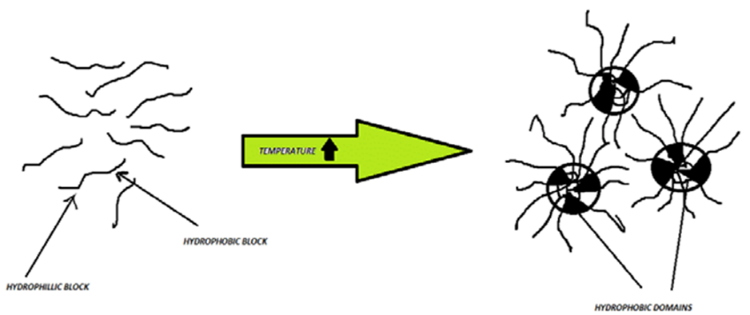
Figure No.7: Temperature Triggered in-situ gel (Adapted and modified from reference no-7
pH-Triggered in-situ gel: In this system, pH variations cause gel formation. This technique uses pH-responsive or pH-sensitive polymers. These polymers have basic or acidic groups that react to variations in the natural pH by releasing or receiving proteins, which subsequently break down and release the medication. Although polyacrylic acid (PAA)-based polymers are also useful, many pH-sensitive polymers are based on carbopol, carbomer, or variants. Polyelectrolytes are the many polymers of ionizable groups. The presence of poly electrolytes in the formulation raises the pH outside, which causes the hydrogel to enlarge and create in situ gel.(10)
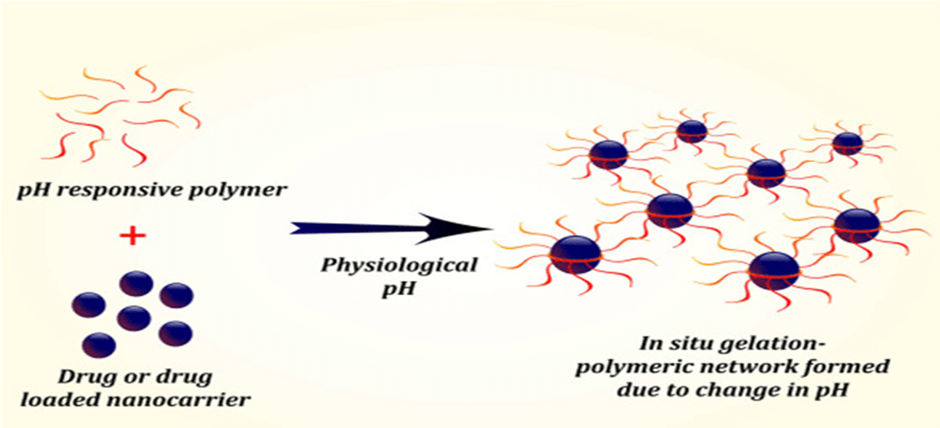
Figure No.8: pH-Triggered in-situ gel (Adapted and modified from reference no-7
Ion activated in-situ gelation: With this approach, a shift in the ionic strength causes the injected solution to gel.(11) The osmotic gradient across the gel's surface is thought to be the determining factor in the gelation rate. Gelrite or gellan gum, hyaluronic acid, alginates, and other polymers exhibit osmotically driven gelation.(12),(13) Monovalent or divalent ions like Na + and Ca+ cause the sol-gel transition process. A few other elements have an impact on the phase transition are the polysaccharide concentration, the preparation temperature, and the type and concentration of cations. Gelrite was chosen to create the in-situ gel.(14)
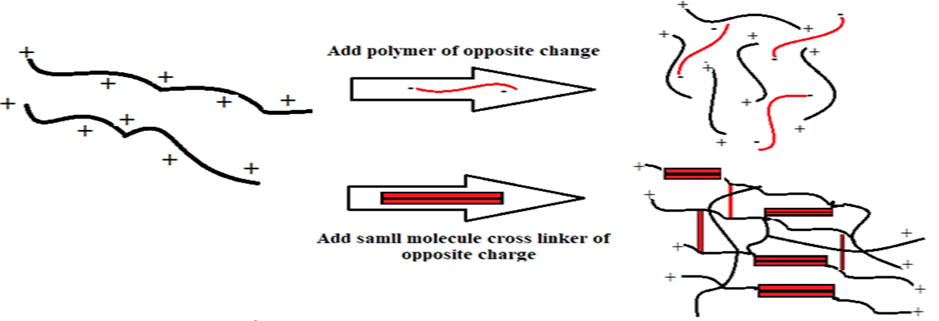
Figure No.9: Ion activated in-situ gel (Adapted and modified from reference no-7)
IDEAL CHARACTERISTICS OF POLYMERS FOR PREPARATION OF IN SITU GEL:
POLYMERS USE FOR PREPARATION OF IN SITU GEL:
Pectin, xyloglucan, and gellan gum are natural polymers utilized in in situ forming oral drug delivery systems. Pectins represent a class of polysaccharides characterized by a polymer backbone predominantly consisting of α-(1-4)-D-galacturonic acid residues. Tamarind seeds contain xyloglucan; a polysaccharide made up of a (1-4)-β-Dglucan backbone chain with (1-6) (1-2)-β-Dgalactoxylose partially substitutes the -α-D xylose branches. Pseudomonas elodea secretes gellan gum, an anionic deacetylated exocellular polysaccharide containing a tetrasaccharide repeating unit consisting of one α-L-rhamnose, one β-D-glucuronic acid, and two β-D-glucuronic acid residues. Gellan gum is commercially marketed as Gelrite TM or Kelcogel TM. It has a propensity to gel, which can be caused by cations or temperature.(17)
POLYMER USE FOR ORAL IN-STU GEL PREPARATION: (23)
Table: 1 Various natural and synthetic Polymers and their use
|
POLYMER |
USES |
|
Pectin |
Gelling agent, Thickening agent, Stabilizer |
|
Xyloglucan |
Thickening agent, Emulsifier, Texture modifier |
|
Gellan gum |
Gelling agent, Thickening agent, Stabilizer |
|
Poloxamer 188 |
Stabilizer, Surfactant, Solubilizer |
|
Poloxamer 407 |
Stabilizer, Surfactant, Solubilizer |
|
Carbopol 934P |
Stabilizer, Thickening agent, Suspension agent |
|
Carrageenan |
Gelling agent, Thickening agent, Stabilizer |
Table: 2 Polymer-Drug Combinations and Their Route of Administration
|
Drug |
Polymer used |
Route of administration |
Reference |
|
Theophylline |
Gellan gum |
Oral |
24 |
|
Doxorubicin |
Human serum albumin and tartaric acid derivative |
Parenteral |
25 |
|
Paracetamol and Ambroxo |
Pectin |
Oral |
26 |
|
Pheniramine maleate and albumin FITC |
Ploymethacrylic acid |
Parenteral |
27 |
|
Recombinant human interleukin-2 |
Physically cross-linked dextran |
Parenteral |
28 |
|
Testosterone |
Poly-lactic acid and PLGA |
Parenteral |
29 |
|
Neem and curcumin |
Carbopol P 934 and poloxamer 188 |
Oral |
30 |
METHODS USING FOR IN-SITU GEL PREPARATION:
Cold Method:
Curcumin's carbopol–poloxamer gel was made using the cold technique. Here Curcumin is active pharmaceutical ingredients. Using a magnetic stirrer, carbopol P934 (1% w/v) was first dissolved in deionized water. After the solution had completely dissolved, it was chilled in an ice bath before gradually adding 30% w/v pluronic F127 while stirring constantly. The liquid was refrigerated at 4 °C for 24 hours in order to guarantee full soaking and eliminate any trapped air bubbles. Curcumin powder, either 1% or 2% w/w, or curcumin that had been dissolved in a suitable amount of PEG400 (140 mg/ml) or ethanol (100 mg/ml) was gradually added to the prepared polymer solution while being stirred in an ice bath. After Each sample was then put into an amber bottle and kept in a refrigerator. The formulation for the in-situ gel that contained Curcumin dissolved in ethanol was placed on stirrer overnight to allow the ethanol to evaporate before being stored in a refrigerator.(31)
General Method of In-situ gel Preparation: (32)
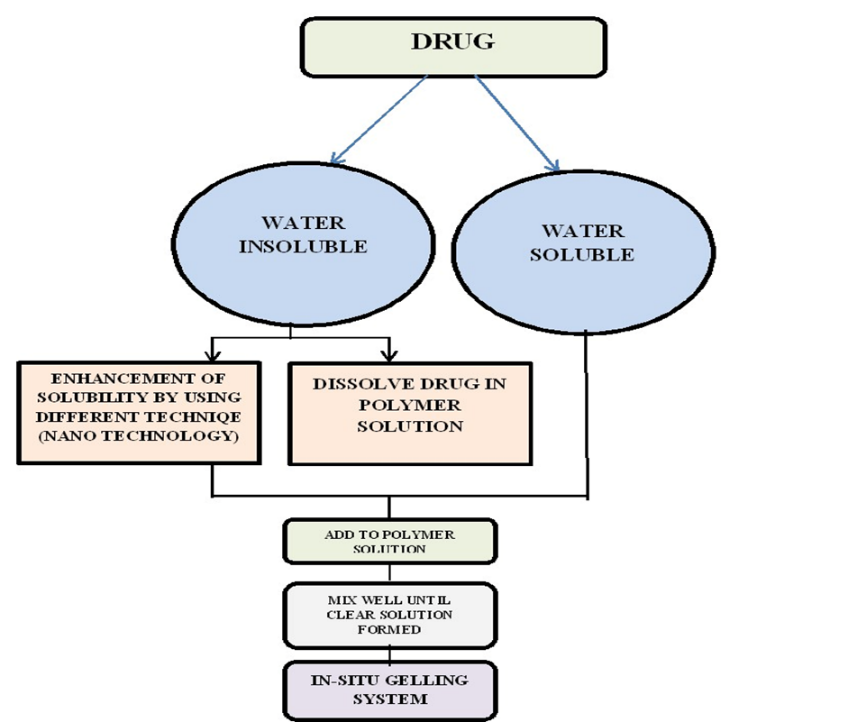
Figure 10: General Method of In-situ gel Preparation Adapted and modified from (Musmade N., et.al 2019)
EVALUATION PARAMETER:
Determination of pH:
50 grams of each gel formulation were weighed, then moved to a beaker and monitored using a digital pH meter.(33)
Viscosity:
The Brookfield viscometer DV-I-LV was used to measure each formulation's viscosity at room temperature (25±5?C). Spindleno.62 was used for the measurements, and it was run at 50 rpm. The viscometer is lowered to dip the spindle into the sample up to an immersion mark on the spindle shaft after a 400–600 ml sample in an appropriate container is placed beneath it. The viscometer monitors the resistance to rotation and outputs a viscosity value while the viscometer motor turns the spindle at a predetermined speed (in rpm) or shear rate. Three separate measurements were made.(34)
Gelation time:
A 15 ml borosilicate glass test tube containing 2 ml of the gel was used to assess the gelation period of the generated in situ gel formulation. This test tube was submerged in a water bath at 37±2 C, and the gelation duration was recorded when the test tube was inverted and the gel did not flow.(35)
Syringeability:
Every created formulation was put into a 5 ml syringe with a 20 gauge needle, keeping the volume constant at 2 ml. The terms "pass" and "fail" were used to describe the solutions that were easy and difficult to pass from the syringe, respectively.(35)
Spreadability:
When applied to the skin or another affected area, the phrase "spreadability" refers to the area over which gel distributes readily. The effectiveness of a formulation as a medication is also influenced by its spreading value. The amount of time it takes for two gel-separated slides to separate under a given stress is used to quantify spreadability.(36)
It is calculated by using the formula:
S=M. LT

------------- (Equation 1)
Where,
Antifungal Activity: The Cup-plate method was used to compare the antifungal activity of all created batches of formulation and the blank formulation, which contained gel and did not include any drug, to the commercial antifungal formulation (Zolef cream). Aspergillus aureus and Candida albicans are the two distinct bacterial cultures that were employed. The agar well diffusion method was used to conduct the antifungal test. The prepared nutrition was brought, poured into sterile petri dishes, and allowed to cool and dry. . Subsequently, a culture of bacteria was dispersed with the help of a micron wire loop. Drilling holes 4 mm deep was done using a sterile cork borer with a 6 mm diameter. Then, fill in these holes with 0.5 g of gel from each batch. After that, plates were incubated for 48 hours at 270 C. After that, the specific compound's zone of inhibition (diameter in mm) was evaluated for each fungal strength.(37)
Gelling capacity:
A vortex (VELP Scientifica, IT) was used for 10 seconds at 500 rpm after 500 µl of the methylene blue-colored sample (1 drop/1 g of sample) was added to a phosphate buffer with a pH of 6.8 that had been tempered at 37?C ± 1?C. The gel's presence was noticed right away when the sol was added, as well as 10, 20, 30, and 60 minutes later. The following indicators were applied to each sample: (-) no gelation; (+) gel forms after a few seconds and then soon disappears; (++) immediate gel formation, which vanishes in less than 20 minutes; and (+++) immediate gel formation, which vanishes after more than 20 minutes. The samples were assessed three times.(38)
Appearance:
Visual evaluations of sols and gels were conducted against a black and white backdrop.(38)
Drug content:
By transferring 1 milliliter of the generated in situ gel formulations into a 100 milliliter volumetric flask, the drug concentration was determined. 50 ml of phosphate buffer (pH 6.8) was added to this volumetric flask, and the gel was shaken continuously until it was completely dispersed, producing a clear solution. Phosphate buffer (pH 6.8) was used to bring the final volume down to 100 ml, and the solution was filtered. Using a UV-visible spectrophotometer, the concentration of the drug in the filtered solution was assessed spectrophotometrically at 257 nm.(39)
In-vitro drug release study:
The Franz diffusion cell was used to conduct an in vitro drug diffusion analysis of different formulations (Gowda et al., 2011). The diffusion membrane was a dialysis membrane with a molecular weight cut-off range of 12,000–14,000 kDa. Before the experiment, the dialysis membrane was let to soak for 24 hours in phosphate buffer (pH 6.4). A diffusion cell containing 21 milliliters of phosphate buffer (pH 6.4) was set up with the dialysis membrane on top. The donor chamber was covered with the gel that contained 10 milligrams of the medication. By using a circulating water bath, the temperature was kept between 32 and 34 °C. At various times, 1 ml samples were taken out and replaced with an equal volume of new solution. The samples were then filtered, and the amount of medication was measured using a UV visible spectrophotometer set to 226 nm.(40)
Stability Studies:
The stability of the in-situ gel was evaluated using the ICH criteria (Q1A R2). To find out if the in-situ gel formulation changed in any way while being stored, its stability was evaluated. For six months, the in-situ gel was kept at 40 ± 2 °C and 75 ± 5% relative humidity in a borosilicate glass container. Samples were collected to examine a number of parameters, including GT, G-time, rheological investigation results, ex-vivo buccalmucoadhesion strength, in-vitro drug release, and ex-vivo permeation qualities, following 0, 3, and 6 months of storage.(41)
RECENT ADVANCES:
Developing effective treatment alternatives that doctors and patients can easily accept is one of the issues facing the pharmaceutical business today. Delivery methods should also help improve therapeutic results by offering potential substitutes for medications that are now administered through other channels. Recent advancements in herbal in situ gels for the treatment of mouth ulcers have focused on enhancing therapeutic efficacy, mucoadhesion, and patient compliance. The goal of this formulation was to increase mucosal adhesion and promote healing by delivering active herbal components directly to the ulcer site. These formulations leverage natural plant extracts known for their anti-inflammatory, antimicrobial, and wound-healing properties. In situ gels are formulated using a variety of biodegradable polymers, these have several drawbacks, including manufacturing issues, challenging processability, the need for organic solvents for their production (especially for systems based on synthetic polymers), burst effect, and irreproducible drug release kinetics. Synthetic polymers are utilized because natural polymers have the qualities of an ideal polymer but are difficult to reproduce batch to batch. However, all of these matters are being dealt with on a daily basis, and in situ forming gels are quickly emerging as a key instrument for drug administration to precise sites. (42)
CONCLUSION
According to the current assessment, the "in situ gel" system has become one of the greatest innovative drug delivery methods, it facilitates the controlled and prolonged release of medications and enhances patient comfort and compliance. Oral, ophthalmic, transdermal, buccal, intraperitoneal, parenteral, injectable, rectal, and vaginal routes are among the possible uses for a variety of natural and synthetic polymers that go through in situ gel formation. Research on the in situ gel system has a lot of potential to produce cutting-edge methods for medication delivery. The use of water-soluble and biodegradable polymers in in situ gel formulations increases their acceptability and quality as a drug delivery strategy.
REFERENCES



Sourav Charan, Vikram Choudhary, In-Situ Gel: A Smart Drug Delivery System for Mouth Ulcer Pain Relief, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 2409-2422. https://doi.org/10.5281/zenodo.17432726
 10.5281/zenodo.17432726
10.5281/zenodo.17432726