Inotropes and vasopressors are essential pharmacological agents in the management of critically ill patients, particularly those experiencing shock. This review updates the use of these vasoactive medications in intensive care unit (ICU) settings, addressing their pharmacology, indications, and clinical efficacy. It covers commonly utilized inotropes such as dopamine, dobutamine, and milrinone, along with vasopressors like norepinephrine and vasopressin. The article discusses factors influencing the choice of therapy, including patient-specific variables, the underlying cause of shock, and real-time hemodynamic monitoring. Special emphasis is placed on the titration of doses to achieve optimal outcomes, minimize adverse effects, and avoid complications associated with prolonged use. Recent advancements in monitoring technologies and evolving evidence from randomized controlled trials are incorporated to provide a comprehensive overview of current practices and emerging strategies for vasoactive therapy in critical care. The review concludes with recommendations for personalized approaches to inotropic and vasopressor management in critically ill patients. This review aims to explore the role of inotropes and vasopressors in critical care, focusing on their mechanisms of action, therapeutic applications, and relevance in managing different forms of shock. Additionally, it highlights the importance of tailoring therapy to individual patient needs, discusses challenges associated with optimizing drug use, and examines emerging advancements in this field. By synthesizing current evidence, the article aims to provide healthcare professionals with valuable insights to enhance patient care in ICU settings.
Inotropes and vasopressors are vital medications for treating circulatory failure and shock in critically ill patients. Inotropes enhance the heart's ability to contract, thereby boosting cardiac output. Commonly used inotropes include dobutamine, dopamine, and milrinone. Vasopressors, on the other hand, primarily work by increasing vascular resistance, leading to higher blood pressure and improved delivery of blood to essential organs. Examples of vasopressors include norepinephrine, vasopressin, and phenylephrine. These drugs are integral to resuscitative measures aimed at stabilizing hemodynamic status in emergencies.
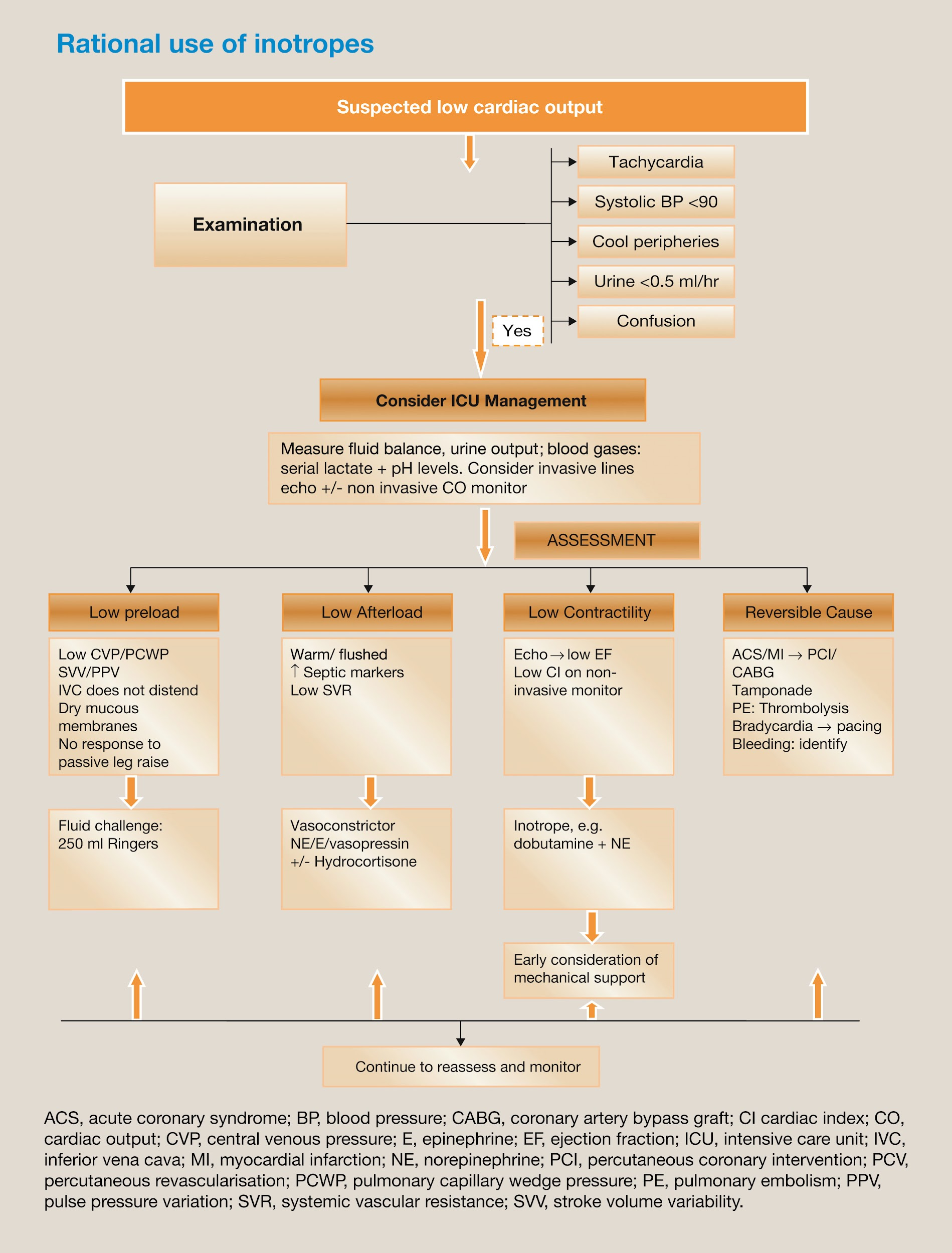
Fig no: 1
Overview of Shock Types and Clinical Relevance
Shock is a critical condition where the body’s tissues receive insufficient oxygen and nutrients, leading to cellular and organ dysfunction. It is classified into several types:
Septesemic This severe form of sepsis arises from widespread inflammation and profound metabolic disturbances, often accompanied by low blood pressure and high mortality risk. Norepinephrine is typically the first-choice vasopressor to restore adequate mean arterial pressure (MAP).
Cardiogenic Shock Resulting from the heart’s inability to pump effectively, this condition is frequently caused by acute myocardial infarction or advanced heart failure. Inotropic agents like dobutamine and mechanical circulatory devices play a crucial role in improving cardiac output and perfusion.
Hypovolemic Shock This occurs due to significant fluid loss from bleeding, dehydration, or severe burns. The priority in managing hypovolemic shock is replenishing intravascular volume, with vasopressors used as a supportive measure only after adequate fluid resuscitation.
Each type of shock has unique mechanisms that require specific therapeutic approaches to achieve the best clinical outcomes and reduce mortality.
Importance of Personalized Therapy in ICU Settings
In critical care, the administration of inotropes and vasopressors must be tailored to the patient’s individual needs. Factors such as preexisting health conditions, specific hemodynamic goals, and real-time assessments of organ function guide the selection and dosing of these agents. Personalized therapy is essential to balance the benefits of improved perfusion against potential risks, such as arrhythmias or ischemic complications. A dynamic and patient-centered approach ensures effective treatment while minimizing adverse outcomes.
Pharmacological Overview
Mechanism of Action
Inotropes:
Dobutamine: Stimulates β1-adrenergic receptors, increasing cAMP levels. This enhances calcium influx, improving heart muscle contraction. Minor β2 stimulation leads to vasodilation, helping to reduce afterload.
Milrinone: Inhibits phosphodiesterase-3, which prevents the degradation of cAMP. This promotes calcium availability in cardiac cells, enhancing contractility and causing vasodilation. It also lowers pulmonary vascular resistance, aiding conditions like right heart failure.
Vasopressors:
Norepinephrine: Primarily activates α1 receptors, inducing vasoconstriction, with secondary β1 effects enhancing cardiac contractility. This raises vascular resistance and blood pressure.
Vasopressin: Targets V1 receptors on vascular smooth muscle to cause vasoconstriction without relying on adrenergic pathways. It also acts on V2 receptors in the kidneys to retain water.
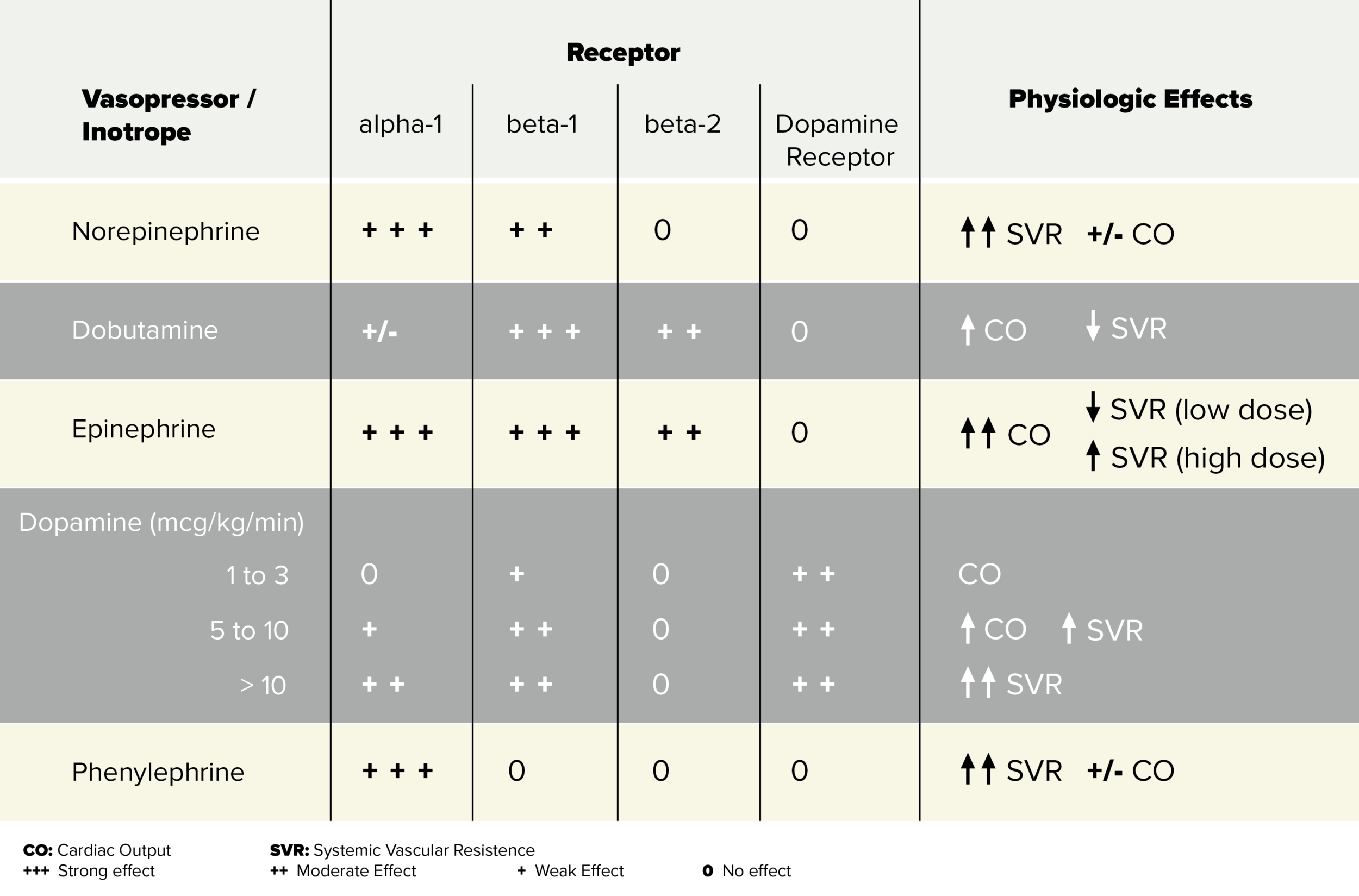
Fig no:- 2
Classification
Adrenergic Agents:
Dopamine: Exhibits dose-dependent receptor activation: low doses target dopamine receptors, moderate doses activate β1 receptors, and high doses stimulate α1 receptors, leading to vasoconstriction.
Norepinephrine: A potent α1 agonist with moderate β1 activity, widely used in septic shock.
Epinephrine: A broad adrenergic agonist (α1, β1, β2), effective in life-threatening conditions like anaphylaxis or cardiac arrest.
Non-Adrenergic Agents:
Vasopressin: Acts independently of adrenergic systems, reducing the likelihood of desensitization seen with catecholamines.
Angiotensin II: Binds to AT1 receptors, leading to vasoconstriction and sodium retention, which helps to restore blood pressure.
Calcium Sensitizers:
Levosimendan: Enhances the sensitivity of the contractile protein troponin C to calcium, improving myocardial contractility without raising intracellular calcium. Additionally, it dilates blood vessels by activating potassium channels.
Key Differences Between Inotropes and Vasopressors
Feature
Inotropes
Vasopressors
Primary Action
Improve heart contractility
Increase vascular resistance
Impact on SVR
Decreases (due to vasodilation)
Increases (due to vasoconstriction)
Use Cases
Heart failure, cardiogenic shock
Hypotension, septic shock
Examples
Dobutamine, Milrinone
Norepinephrine, Vasopressin
Applications in Clinical Practice
Inotropes: Used to boost cardiac output in heart failure or cardiogenic shock.
Vasopressors: Help maintain blood pressure in critically low-perfusion states like septic shock, often combined with inotropes in mixed shock scenarios.
This review delves into the mechanisms of action of vasopressors and inotropes, specifically norepinephrine, vasopressin, and others, with a focus on their role in managing septic shock
Clinical Indications for Inotropes and Vasopressors in Shock
Inotropes and vasopressors are essential in the management of shock, a condition that impairs tissue perfusion and oxygenation. Their use is crucial to stabilize hemodynamics and restore organ function, and the choice of agent depends on the type of shock and the patient's condition. The following outlines the clinical indications for their use in various types of shock:
1. Septic Shock: Norepinephrine as First-Line Therapy
Septic shock is characterized by severe vasodilation, leading to hypotension and poor tissue perfusion despite adequate fluid resuscitation. Norepinephrine is the vasopressor of choice, as it acts on α-adrenergic receptors to constrict blood vessels, increasing blood pressure and enhancing perfusion to vital organs. It is supported by guidelines, including the Surviving Sepsis Campaign.
2. Cardiogenic Shock: Role of Dobutamine and Mechanical Support
In cardiogenic shock, the heart cannot pump enough blood due to conditions like myocardial infarction or heart failure. Dobutamine, an inotropic agent, is commonly used to increase cardiac output by stimulating β1-adrenergic receptors, thus enhancing heart contractility. In severe cases, mechanical circulatory support such as intra-aortic balloon pumps (IABP) may be required.
3. Hypovolemic Shock: Fluid Resuscitation Before Vasopressors
Hypovolemic shock results from significant fluid loss (e.g., due to haemorrhage or dehydration), causing decreased blood volume and inadequate tissue perfusion. The first priority in treatment is fluid resuscitation using crystalloids or colloids to restore intravascular volume. Vasopressors, such as norepinephrine, are used only if hypotension persists after adequate fluid replacement.
4. Indications for Combined Therapy (e.g., Norepinephrine + Dobutamine)
In certain cases, a combination of inotropes and vasopressors may be needed to manage both hypotension and low cardiac output. For example:
Norepinephrine + Dobutamine: In cardiogenic shock, norepinephrine provides necessary vasoconstriction to support blood pressure, while dobutamine increases myocardial contractility to improve cardiac output.
Norepinephrine + Vasopressin: In refractory septic shock, vasopressin can be added to norepinephrine to improve perfusion without the adverse effects of high doses of norepinephrine.
Summary of Key Points:
Septic shock: Norepinephrine is the first-line vasopressor.
Cardiogenic shock: Dobutamine is used to enhance cardiac output, and mechanical support may be required in severe cases.
Hypovolemic shock: Fluid resuscitation is the primary treatment, with vasopressors used only if hypotension persists.
Combined therapy: Norepinephrine, when combined with inotropes or vasopressin, helps optimize hemodynamic in refractory shock cases.
Monitoring and Outcome Assessment in Shock Management
Effective monitoring is vital for the management of shock, providing insights into a patient’s hemodynamic status and guiding treatment decisions. Both invasive and non-invasive monitoring techniques, along with biomarkers, are key tools for evaluating therapeutic effectiveness and improving outcomes in critically ill patients.
Hemodynamic Monitoring
Invasive Techniques:
Arterial Line (A-line): Provides continuous and accurate blood pressure measurements, allowing immediate adjustments of medications such as vasopressors and inotropes. It is particularly valuable in patients with severe hypotension, enabling rapid interventions based on real-time data.
Pulmonary Artery Catheter (PAC): Measures key parameters, including pulmonary artery pressure, cardiac output, and mixed venous oxygen saturation (SvO2). PAC offers comprehensive data about circulatory function, which is particularly beneficial in conditions like cardiogenic shock, where detailed monitoring of cardiac performance and fluid status is required.
Non-Invasive Techniques:
Echocardiography: This imaging technique evaluates heart function, including cardiac output, ejection fraction, and fluid status. It is crucial in assessing myocardial performance, particularly in patients with cardiogenic shock, and helps guide the use of inotropes and fluid management.
Bioimpedance: This portable, non-invasive method estimates cardiac output and stroke volume. Though not as detailed as invasive techniques, it offers continuous monitoring, especially useful for less critically ill patients or for ongoing assessment in stable shock cases.
Biomarkers for Therapy Effectiveness
Lactate Clearance: Elevated lactate levels often indicate poor tissue perfusion. Monitoring lactate levels and their clearance over time is a key strategy for evaluating the effectiveness of resuscitation and shock management.
Procalcitonin (PCT): PCT is a biomarker for bacterial infections, and its levels can help guide antibiotic therapy. In septic shock, measuring PCT can aid in assessing infection severity and tailoring treatment accordingly.
ScvO2: This measure of mixed venous oxygen saturation provides insight into the balance between oxygen delivery and consumption. Monitoring ScvO2 helps ensure adequate tissue oxygenation, guiding interventions to improve perfusion.
Emerging Trends and Controversies in Inotrope and Vasopressor Use
1. New Agents in Critical Care
Angiotensin II:
Mechanism: A potent vasoconstrictor that activates AT1 receptors, increasing systemic vascular resistance (SVR) and blood pressure. It's increasingly used in refractory septic shock, particularly when patients fail to respond to traditional vasopressors like norepinephrine.
Clinical Evidence: Studies such as the ATHOS-3 trial show that angiotensin II can improve blood pressure in vasodilatory shock, particularly in patients with persistent hypotension despite high-dose vasopressor therapy.
Applications: Particularly useful in septic shock where standard vasopressors are ineffective or in cases where catecholamine use needs to be minimized.
Mechanism: These agents selectively stimulate β2-adrenergic receptors, leading to vasodilation, and β1 receptors, increasing heart rate and contractility. They are being investigated for their role in improving cardiac output in specific shock states like low-output syndrome or heart failure.
Clinical Evidence: Early studies suggest that selective β2-agonists may help in conditions with predominant vasodilation (like septic shock), although their widespread clinical use is still being explored.
2. Debate on the Optimal First-Line Vasopressor
Norepinephrine:
Current Standard: Norepinephrine remains the first-line choice in septic and distributive shock due to its effectiveness in increasing systemic vascular resistance (SVR) through α1 receptor activation and providing some inotropic support via β1 activity.
Controversy: The primary issue lies in its use in patients with compromised myocardial function, as β1 stimulation can worsen heart failure or trigger arrhythmias. Some studies debate whether norepinephrine is always the best choice, especially in mixed shock states or when myocardial function is already impaired.
Alternative Vasopressors:
Vasopressin and Angiotensin II are increasingly being used as adjuncts or alternatives to norepinephrine, particularly in cases where norepinephrine is insufficient or patients develop tachyphylaxis.
Proposed Guidelines: While dopamine remains a consideration in specific populations, such as those with bradycardic shock, norepinephrine is generally preferred due to its safety and efficacy profile.
3. Role of Levosimendan in Refractory Cases
Mechanism: Levosimendan is a calcium sensitizer that improves myocardial contractility by enhancing the sensitivity of troponin C to calcium without increasing intracellular calcium levels. It also promotes vasodilation.
Clinical Evidence: Levosimendan has shown promise in patients with refractory heart failure, particularly those unresponsive to traditional inotropes like dobutamine. It may offer the additional benefit of reducing arrhythmia risks and improving cardiac function in acute decompensated heart failure (ADHF).
Controversy: Despite its potential, the use of levosimendan remains controversial. Some studies suggest that it might not provide significant benefits in all patient populations, particularly in those with concurrent sepsis and heart failure.
4. Strategies for Reducing Inotrope and Vasopressor Dependency
Goal-Directed Therapy (GDT):
Mechanism: GDT involves fluid resuscitation and targeted hemodynamic therapy to optimize preload, afterload, and myocardial contractility early in treatment. This approach aims to minimize reliance on pharmacological support over time.
Evolving Practices: Techniques such as early use of inodilators (e.g., milrinone) and blood pressure-targeted therapies are being explored as methods to reduce high-dose vasopressor and inotrope use.
Pharmacological Alternatives:
Angiotensin II and Vasopressin have been considered as alternatives to traditional vasopressors to reduce dependency on catecholamines. Additionally, non-pharmacological strategies like extracorporeal life support (ECLS) and intra-aortic balloon pump (IABP) are being studied for severe shock cases.
Weaning Protocols:
Gradual weaning from inotropes and vasopressors, with close monitoring of hemodynamics, is a key strategy for reducing dependency. Protocols that minimize drug doses and transition to oral therapies have shown promising results in improving recovery in critical care patients.
Challenges and Limitations
The use of inotropes and vasopressors in critical care settings, particularly for prolonged periods, presents several challenges and limitations:
Tachyphylaxis and Organ Damage: Prolonged use of drugs like dobutamine can lead to tachyphylaxis, where the body becomes less responsive to the medication due to β-receptor downregulation. Additionally, these drugs increase myocardial oxygen consumption, which can exacerbate myocardial ischemia, potentially leading to arrhythmias and higher mortality, especially in critically ill patients. Similarly, vasopressors such as norepinephrine can cause direct toxic effects on cardiac myocytes, potentially triggering cell death via mechanisms like protein kinase A activation and elevated intracellular calcium levels?
Challenges in Interpreting Clinical Trials: Many clinical trials on inotropes and vasopressors include heterogeneous patient populations, which complicates the generalization of results. In critically ill patients, individual variations—such as comorbidities or underlying pathophysiology—can significantly influence how patients respond to these drugs, making it difficult to determine a one-size-fits-all approach?
Guidelines and Individualized Therapy: Although existing guidelines recommend standard therapies (e.g., norepinephrine for septic shock), they do not always account for individual variations in patient responses. As a result, there is an increasing shift toward personalized treatment plans, where factors like comorbidities, hemodynamic profiles, and responses to prior treatments should guide the choice and dosing of inotropes and vasopressors?.
Future Directions
Innovations in Drug Delivery: Closed-loop infusion systems are emerging as a significant advancement in critical care. These systems adjust drug infusion rates in real-time based on patient data, improving the precision of inotrope and vasopressor administration, and reducing human error. Such systems are designed to optimize hemodynamic support while ensuring more personalized and effective treatment?.
Combination Therapies: There is growing interest in combining different agents, such as inotropes with vasodilators, to address multiple factors simultaneously. For example, combining agents that improve cardiac output with those that manage vascular resistance could offer a more balanced and effective approach for managing critical patients, while potentially minimizing side effects compared to monotherapy?.
Inotropes and vasopressors are fundamental in managing critically ill patients in ICU settings, particularly for stabilizing blood pressure and improving cardiac output during shock states. These therapies are essential for maintaining adequate circulation and preventing further organ damage in patients with compromised hemodynamic status.
CONCLUSION
Optimal use of these agents, however, demands careful consideration of each patient’s specific condition. The increasing recognition of the need for individualized treatment strategies, aided by dynamic monitoring tools, is crucial in maximizing their effectiveness while minimizing risks like organ injury or tachyphylaxis. Adjusting dosages based on real-time responses allows clinicians to optimize patient care more precisely.
Looking ahead, further research is needed to assess the long-term outcomes associated with inotropes and vasopressors, focusing on potential risks such as myocardial injury and multi-organ dysfunction. Moreover, the development of innovative drug delivery systems (e.g., closed-loop systems), along with combination therapies and personalized dosing approaches, offers exciting prospects for improving the safety and efficacy of critical care management. Continued exploration of these strategies will be crucial for enhancing the overall outcomes of critically ill patients.
Future research should aim to refine existing guidelines, explore the long-term effects of inotrope and vasopressor use on survival and organ function, and establish best practices to reduce dependency on these agents in ICU care. This ongoing innovation in critical care treatment holds promise for improving both short- and long-term patient outcomes.
REFERENCES
Perner, A., Haase, N., & Guttormsen, A. B. (2016). Inotropes and Vasopressors in the Intensive Care Unit: An Update on Their Use and Efficacy. Lancet, 388(10058), 1016-1025. https://doi.org/10.1016/S0140-6736(16)30714-1
Morris, L. L., & Collier, J. A. (2020). Pharmacotherapy in Critical Care: A Review of Inotropes and Vasopressors. Journal of Intensive Care Medicine, 35(8), 727-734. https://doi.org/10.1177/0885066619873432
Vincent, J. L., & Russell, J. A. (2019). Inotropes and Vasopressors in Septic Shock: Efficacy and Safety. Current Opinion in Critical Care, 25(6), 534-542. https://doi.org/10.1097/MCC.0000000000000631
Maharaj, R. et al. (2018). Inotropes and Vasopressors: A Review of Mechanisms of Action and Clinical Use in Critical Care. Journal of Critical Care, 48, 1-10.
Annane, D., & Aupérin, A. (2015). Vasopressors and Inotropes in Sepsis: Mechanisms and Clinical Applications. British Journal of Anaesthesia, 115(3), 289-297
Rivers, E., Nguyen, B., Havens, P., et al. (2001). Early Goal-Directed Therapy in the Treatment of Severe Sepsis and Septic Shock. New England Journal of Medicine, 345(19), 1368-1377. https://doi.org/10.1056/NEJMoa010307
Vincent, J.-L., & De Backer, D. (2013). Circulatory shock. New England Journal of Medicine, 369(18), 1726-1734. https://doi.org/10.1056/NEJMra1208943
Perner, A., Haase, N., & Guttormsen, A. B. (2016). Inotropes and Vasopressors in the Intensive Care Unit: An Update on Their Use and Efficacy. Lancet, 388(10058), 1016-1025. https://doi.org/10.1016/S0140-6736(16)30714-1
Morris, L. L., & Collier, J. A. (2020). Pharmacotherapy in Critical Care: A Review of Inotropes and Vasopressors. Journal of Intensive Care Medicine, 35(8), 727-734. https://doi.org/10.1177/0885066619873432
Vincent, J. L., & Russell, J. A. (2019). Inotropes and Vasopressors in Septic Shock: Efficacy and Safety. Current Opinion in Critical Care, 25(6), 534-542. https://doi.org/10.1097/MCC.0000000000000631
Maharaj, R. et al. (2018). Inotropes and Vasopressors: A Review of Mechanisms of Action and Clinical Use in Critical Care. Journal of Critical Care, 48, 1-10.
Annane, D., & Aupérin, A. (2015). Vasopressors and Inotropes in Sepsis: Mechanisms and Clinical Applications. British Journal of Anaesthesia, 115(3), 289-297
Rivers, E., Nguyen, B., Havens, P., et al. (2001). Early Goal-Directed Therapy in the Treatment of Severe Sepsis and Septic Shock. New England Journal of Medicine, 345(19), 1368-1377. https://doi.org/10.1056/NEJMoa010307
Vincent, J.-L., & De Backer, D. (2013). Circulatory shock. New England Journal of Medicine, 369(18), 1726-1734. https://doi.org/10.1056/NEJMra1208943
Pharmacy practice department, Shivalingeshwar college of pharmacy, almala, Tq ausa, dist latur, 413520.
Bhise Pranjali
Co-author
Pharmacy practice department, Shivalingeshwar college of pharmacy, almala, Tq ausa, dist latur, 413520.
Dhakne Ganesh
Co-author
Pharmacy practice department, Shivalingeshwar college of pharmacy, almala, Tq ausa, dist latur, 413520.
Dr. Bhambre Akshay
Co-author
Pharmacy practice department, Shivalingeshwar college of pharmacy, almala, Tq ausa, dist latur, 413520.
Gawali Pravin, Bhise Pranjali, Dhakne Ganesh, Dr. Bhambre Akshay, Inotropes and Vasopressors: An Update on Use in ICU Settings, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 1374-1383. https://doi.org/10.5281/zenodo.15613269



 10.5281/zenodo.15613269
10.5281/zenodo.15613269