1,2,4,5 Department of Pharmacy Practice, St Joseph’s College of Pharmacy, Cherthala, Kerala, India
3Department Of Cardiology, VPS Lakeshore Hospital, Kochi, Kerala, India
Dual antiplatelet therapy (DAPT) with an oral P2Y12 antagonist and Aspirin is a key therapeutic approach in patients with post-angioplasty for acute myocardial infarction. DAPT provides more significant platelet inhibition, leading to a gradual decrease in the risk of major adverse cardiac events, particularly recurrent ischemic events such as myocardial infarction, including stent thrombosis, ischemic stroke, or death from cardiac cause. Although intracerebral hemorrhage (ICH) is a hidden negative side of Antiplatelet therapy (APT), its incidence is relatively low. Here, we present a case of a patient with hypertension (HTN) post-percutaneous coronary intervention (PCI) with a drug-eluting stent for acute myocardial infarction who developed ICH after the initiation of DAPT. On further evaluation, the condition was attributed to DAPT and hypertension.
In patients who have undergone angioplasty for acute myocardial infarction, Dual antiplatelet therapy (DAPT) with aspirin and a P2Y12 antagonist is an established therapy. Post-angioplasty, the therapeutic benefit of DAPT in reducing ischemic events is partially offset by its associated bleeding risk, with intracerebral hemorrhage (ICH) being the most serious complication, necessitating a careful risk-benefit assessment in clinical decision-making.1 ICH corresponds to any bleeding within the brain parenchyma leading to accumulation of blood in the surrounding spaces, with the potential to cause significant neurological deficits, identified and confirmed through computed tomography (CT) scan and Magnetic resonance imaging. Diabetes, hypertension, antiplatelet and anticoagulant drugs, dyslipidemia, smoking, age, and alcohol consumption are recognized risk factors of ICH. Hypertension and dual antiplatelet therapy are the most important risk factors. 2,3 In patients receiving Antiplatelet therapy (APT), ICH is an uncommon adverse drug reaction (ADR), and even a “minor” head injury can be attributed to an elevated risk of developing ICH.3,4 In the initial days after an ICH, progressive metabolic changes, neuronal injury, and apoptotic processes in the perihematomal region contribute to secondary damage, which is believed to cause more widespread consequences than the immediate effect of the hematoma itself.5 Although ICH is not associated with a high mortality rate, it can result in long-term disabilities, including cognitive impairments, motor dysfunction, and other neurological complications that can lead to significant reductions in quality of life. These long-term disabilities often require extensive rehabilitation and ongoing care, which can place a significant burden on the patient, their family, and the healthcare system. Discontinuing DAPT urgently in such cases is essential because continuing the therapy can worsen the hemorrhage and lead to more severe brain damage, increasing the likelihood of long-term disability.3,5 But it may predispose the patient to an increased risk of stent thrombosis. Thus, it is crucial to address the potential ischemic risk and bleeding in the management of ICH patients who were on APT.
CASE PRESENTATION:
A 47-year-old female patient with a history of hypertension and diabetes mellitus was recently diagnosed with acute non-ST-elevation myocardial infarction and coronary artery disease with triple vessel involvement. She underwent percutaneous coronary intervention (PCI) with the placement of a drug-eluting stent and was on Dual antiplatelet therapy (DAPT). She was on following the medications for her disease management: Tab. Aspirin 75mg OD, Tab. Ticagrelor 90 mg BD, Tab. Atorvastatin 40 mg OD, T. Metoprolol 50 mg BD, Tab. Telmisartan 40 mg OD, Tab. Dapagliflozin 10 mg OD, Tab. Sitagliptin 50mg + Metformin 500 mg BD, Inj. Insulin Aspart, Inj. Insulin glargine, Tab. Pantoprazole 40 mg. One week after the initiation of DAPT therapy, she presented to the emergency department with complaints of giddiness, cervical tenderness, loss of consciousness, and a fall-associated trauma to the head. She reported experiencing headaches for a few days after the initiation of DAPT, even before the head injury. Neurological examination suggested a moderate head injury and computed tomography (CT) of the brain and whole spine revealed acute intraparenchymal hematoma measuring 1.5×1.4×1.2 cm in the left superior cerebellar hemisphere and a slightly higher troponin I (Trop I) level and a lower serum sodium concentration were observed in laboratory tests. Based on the findings, she was diagnosed with ICH and was initiated with Inj. Levetiracetam for seizure prophylaxis and Inj. Citicoline a neuroprotectant. In view of the acute event of ICH, antiplatelet therapy was withheld, and the CT scan was repeated. Follow-up CT scan showed reduced hematoma size. Considering the timing of her symptom presentation with regard to initiation of DAPT, despite uncontrolled hypertension and minor trauma, clinical assessment, along with lab investigation and scan reports, indicated that ICH may be attributed to antiplatelet therapy and hypertension. Serial CT scans of the brain show resolving intraparenchymal bleed in the left superior cerebellar hemisphere:
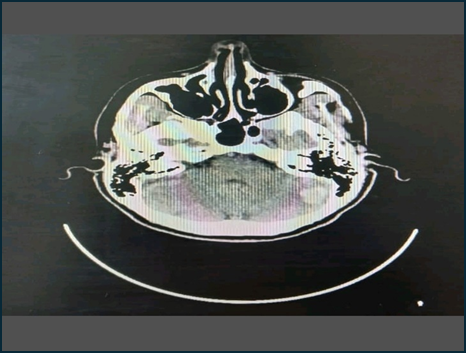
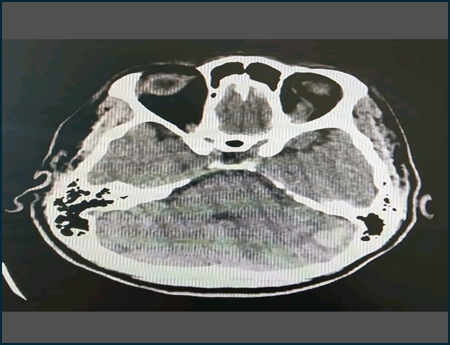
Fig.1, Day 1 of IC bleed. Fig.2, Day 2 of IC bleed.
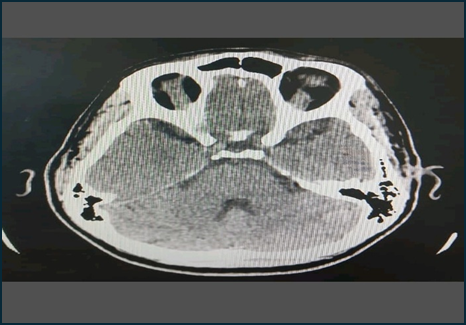
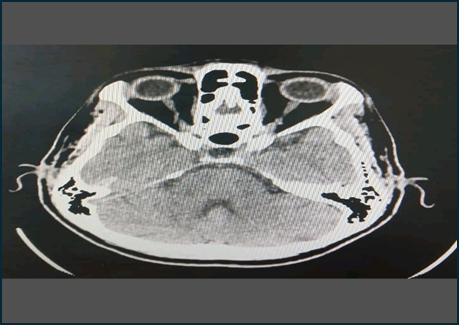
Fig.3, Day 6 of IC bleed. Fig.4, Day 30 of IC bleed.
Ecosprin 75 mg was restarted on Day 5, and Clopilet 37.5 mg was restarted on Day 15. Further, the dose of Clopidogrel was escalated to 75 mg made on Day 22, and Ecosprin 150 mg was made on Day 37. The day after the fall, considering her cardiovascular risk, a single antiplatelet therapy was started. Following the subsequent CT scan, the patient was switched to DAPT (Aspirin 75 mg, clopidogrel 37.5 mg) since her likelihood of a cardiovascular event was higher than the stabilized ICH. The risk of stent thrombosis is greater in the first month following PCI. Hence, there is a need to restart the dual antiplatelet at the earliest, in spite of having an IC bleed. The risk vs. benefit was discussed with the neurosurgeon and patient, and the antiplatelet was gradually restarted. Meanwhile, Ticagrelor was replaced with clopidogrel due to its potential bleeding risk.
DISCUSSION
When we examine studies on the use of ticagrelor and aspirin [Dual antiplatelet therapy] given in diabetic patients with stable heart disease and a history of percutaneous coronary intervention (PCI), adding ticagrelor to aspirin reduced the risk of heart attack, stroke, and cardiovascular death. However, research has indicated that combining antiplatelet drugs increases the risk of intracranial hemorrhage (ICH) compared to using a single antiplatelet medication. Despite the bleeding concerns, patients on ticagrelor showed generally improved clinical results, particularly those with a history of PCI.6,7 In contrast, antiplatelet medications appear to contribute to the immediate clinical deterioration of intracerebral hemorrhage and can lead to the enlargement of the hematoma.8 When we consider aspirin and its risk, it might slightly increase the risk of hemorrhagic stroke but not subarachnoid hemorrhage.9 Comparative studies on ticagrelor versus clopidogrel found a clear increase in bleeding events (defined by PLATO criteria) in patients receiving ticagrelor compared to clopidogrel when both were used for medical management. The PLATO trial demonstrated an increased incidence of major hemorrhagic events associated with ticagrelor, independent of Coronary Artery Bypass Graft related bleeding, indicating an increased risk of major bleeding complications with its use.10 Another study by Tomek et al. demonstrated that patients on ticagrelor experienced a significantly higher rate of major and minor bleeding episodes requiring medical attention compared to those on clopidogrel. This was largely driven by a greater incidence of spontaneous bleeds. Within these spontaneous bleeds, ticagrelor was associated with increased risks of both major gastrointestinal and intracranial hemorrhages, the two most frequent types of spontaneous major bleeds observed in the PLATO trial. Additionally, the study found that ticagrelor use carried a higher risk of intracranial hemorrhage, death from intracranial hemorrhage, and hemorrhagic stroke compared to clopidogrel. It concluded that clopidogrel presents a safer profile than ticagrelor with regard to the bleeding risk.11
CONCLUSION
In this case, it is rational to use dual antiplatelet therapy (aspirin with either clopidogrel or ticagrelor) for the patient due to her increased cardiovascular risk. However, studies suggest ticagrelor is associated with a higher risk of major bleeding, particularly intracranial hemorrhage. As she had an ICH event, taking into account the uncommon ADR of ticagrelor, adding ticagrelor might contribute to the deterioration of the patient’s condition. Thus, clopidogrel was preferred over ticagrelor in view of its lower bleeding risk, and continued DAPT was used along with aspirin. A limitation of this case report is that the intracranial hemorrhage (ICH) could be attributed to either dual antiplatelet therapy (DAPT) or underlying hypertension, which complicates the determination of the primary cause.
ACKNOWLEDGEMENT
We sincerely thank Siby Joseph, HOD Pharmacy practice, St. Joseph’s College of Pharmacy, for the invaluable guidance and support while preparing this case report.
REFERENCES

Cijy John, Akash Jose Kollanassery*, Venkateshwaran S, Blessy Cherian, Aiswarya Wilson, Intracerebral Hemorrhage Complicating Post-Angioplasty in a Hypertensive Patient on Dual Antiplatelet Therapy: A Case Report, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 3260-3064. https://doi.org/10.5281/zenodo.15464705
 10.5281/zenodo.15464705
10.5281/zenodo.15464705
