Shivajirao S. Jondhle college of pharmacy, Thane, India
One of the most prevalent gynecological conditions affecting women of reproductive age is dysmenorrhea, or unpleasant menstruation. Women's physical, mental, and social well-being are greatly impacted, and it frequently results in a dependence on synthetic drugs that only offer short-term comfort. While NSAIDs and hormonal therapy are examples of conventional treatments that offer symptomatic relief, their side effects and questionable long-term safety have prompted research into herbal alternatives. By using multi-target techniques to address the underlying causes of menstruation pain, herbal therapy provides a comprehensive and natural solution. Using herbal formulations to treat dysmenorrhea is a promising way to combine traditional knowledge with contemporary pharmaceutical technologies. Both patient compliance and bioavailability can be enhanced by herbal treatments. In order to develop standardized herbal therapies for the treatment of dysmenorrhea, the study ends with suggestions for quality control, clinical validation, and sustainable sourcing. This review looks on the creation of innovative herbal dose forms intended to safely and successfully reduce menstrual pain. It highlights important medicinal plants that support reproductive health and have analgesic, anti-spasmodic, and hormone-balancing properties. The study focuses on integrative methods that incorporate safe dosage design, modern pharmacological validation, and conventional formulations. This review advances the more general objective of empowering women's health through natural therapies by promoting sustainable and evidence-based herbal innovation.
Classification of dysmenorrhea [10-18]
Patients with primary dysmenorrhea typically have normal findings. A locked uterus or decreased uterine mobility, adnexal masses, and uterosacral nodularity in endometriosis patients, mucopurulent cervical discharge in PID patients, and uterine enlargement or asymmetry in adenomyosis patients are among the findings in patients with secondary dysmenorrhea.[10] Dysmenorrhea primary: - Painful menstruation without any indication of hormonal or anatomic (pelvic) disease is known as primary dysmenorrhea. Among women of reproductive age, it is one of the most common and significant complaints [11].
The quality of life is significantly impacted by primary dysmenorrhea, which frequently leads to increased healthcare needs, decreased productivity, and absenteeism from work or school. [12] The pain typically starts a few hours prior to or immediately following menstruation and lasts for 48 to 72 hours [13]. The underlying cause of primary dysmenorrhea is not entirely understood. However, an increase in uterine tone and high-amplitude contractions have been found to be caused by an overabundance of uterine prostaglandins, specifically PGF2a and PGF2 [14]. Dysmenorrhea secondary: - Certain pelvic pathologies cause secondary dysmenorrhea. Until proven otherwise, elder women without a history of dysmenorrhea should be suspected.[15] Patients having a family history of endometriosis in first-degree relatives are more likely to have secondary dysmenorrhea; a family history may be useful in distinguishing between primary and secondary dysmenorrhea.[16] Endometriosis is the most frequent cause of secondary dysmenorrhea, which affects 10% of young adults and adolescents with dysmenorrhea [17]. Menorrhagia, intermenstrual bleeding, dyspareunia, postcoital bleeding, and infertility are among the symptoms. The most frequent cause of secondary dysmenorrhea is endometriosis. [18]
Risk Factors [19-28]
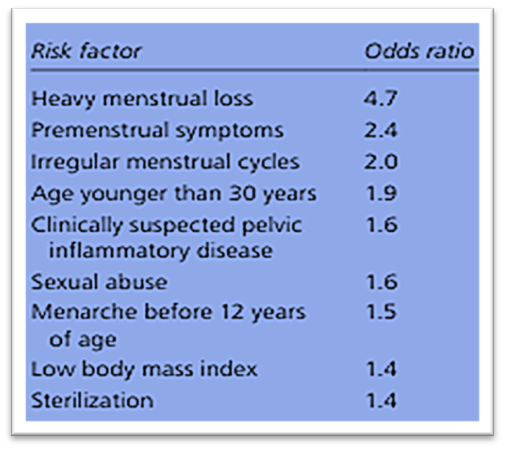
It is somewhat nonsensical to refer to dysmenorrhea as a central sensitization syndrome, as that would imply that 40–90% of women have an aberrant physiological state, even if we and others have discovered evidence linking dysmenorrhea to a higher chance of developing a chronic pelvic pain syndrome. [19, 20] Risk factors for primary dysmenorrhea can be classified as either behavioral or non-modifiable. A family history of dysmenorrhea, being under 20 (the symptoms are more noticeable throughout adolescence), menarche before age 12 (because ovulatory cycles are established earlier), menstrual flow lasting more than seven days, and nulliparity are examples of non-modifiable risk factors. [21, 22, 23, 24, 25, 26] A number of hypotheses, including reduced prostaglandin release by the endometrium following a term delivery, neuronal degeneration in the uterus following a term delivery, and decreased uterine norepinephrine during the third trimester of pregnancy, can account for the correlation between multiparity and a lower risk of dysmenorrhea.[27] Since these behavioral characteristics can be addressed, it is critical to identify them. [21, 22, 23, 24, 25, 26] Stress prevents luteinizing and follicle-stimulating hormones from being released, which impairs follicular development and changes the production and release of progesterone, which affects prostaglandin activity. Additionally, prostaglandin production and myometrial binding are influenced by stress-related chemicals such cortisol and adrenaline.[27]
Table 1 lists risk factors for the development of dysmenorrhea [28]
Differential Diagnosis of Dysmenorrhea: -
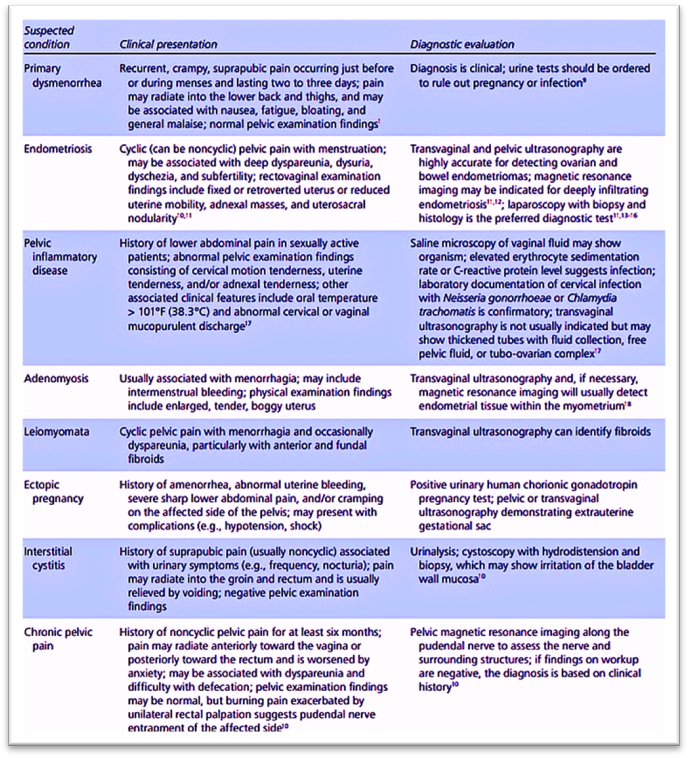
Figure 2 Information from references 30 and 39
Why Herbal[40-43]?
The term "herbal" often refers to goods that are derived from plants and utilized for therapeutic purposes. Alkaloids, polyphenols, flavonoids, terpenes, and phenols—all of which have therapeutic effects on the body—are among the bioactive molecules that make up these substances. In an effort to identify their biological uses, the disciplines of pharmacognosy, phytochemistry, and pharmacology are attempting to separate and comprehend these bioactive substances present in medicinal plants. To explore the possibilities, research is essential. including the antibacterial, antioxidant, antimicrobial, and calming effects of herbal medicine for certain medical disorders. Many civilizations have a long history of using herbal remedies to treat menstruation problems. The term "herbal" often refers to goods that are derived from plants and utilized for therapeutic purposes. Alkaloids, polyphenols, flavonoids, terpenes, and phenols—all of which have therapeutic effects on the body—are among the bioactive molecules that make up these substances. In an effort to identify their biological uses, the disciplines of pharmacognosy, phytochemistry, and pharmacology are attempting to separate and comprehend these bioactive substances present in medicinal plants. To explore the possibilities, research is essential. including the antibacterial, antioxidant, antimicrobial, and calming effects of herbal medicine for certain medical disorders. Many civilizations have a long history of using herbal remedies to treat menstruation problems. Primary dysmenorrhea may be effectively treated with herbal treatments. Finding a treatment for primary dysmenorrhea is becoming more and more important, despite the fact that many studies have been done on the analgesic effects of plant extracts.[42] and frequently include natural essential oils that improve skin penetration and provide additional therapeutic benefits like muscle relief, relaxation, and cooling.[43]
Management of dysmenorrhea
can be carried out both non-pharmacologically and pharmacologically. Analgesics, hormone therapy, prostaglandin nonsteroidal drugs, and lactical canal lactation are examples of pharmacological treatment options for menstrual pain; vitamin E supplements, acupuncture, hypnotherapy, and herbal products that have been shown to be beneficial are examples of nonpharmacological treatment options. [44] Localized heat, medicine, thiamin, vitamin E, fish oil supplements, acupuncture, and transcutaneous nerve stimulation are just a few of the techniques utilized today to treat and manage pain and symptoms. These medications, including mefenamic acid and ibuprofen, have side effects, just like many pharmacological treatments. Particularly when synthetic drugs are prescribed for a long time, the adverse effects become apparent.Nausea, stomach discomfort, ulcers, gastrointestinal issues, renal papillary necrosis, and renal blood flow are among the side effects of prostaglandin production inhibitors. The adverse effects of these drugs have drawn special attention to the use of complementary therapies, such as nutrients or herbs, in the treatment of primary dysmenorrhea or related issues. [45] The most prevalent and biologically active prostaglandin in mammals is prostaglandin E2, or dinoprostone. Prostaglandin E synthase, which has at least three physically and physiologically different variants, produces it from PGH2. The primary enzyme in the production of PGE2 appears to be microsomal prostaglandin E synthase-1 (mPGES1).
Endoperoxide F reductase can produce prostaglandin F2 directly from PGH2, although PGE 9-ketoreductase often produces it from PGE2 [46].
CONCLUSION
In conclusion, dysmenorrhea is still a very common and crippling illness that negatively affects women's productivity, education, and quality of life worldwide. While traditional therapies like NSAIDs provide comfort, their adverse effects highlight the urgent need for safer substitutes, especially when used over an extended period of time. Dysmenorrhea is still a common gynecological disorder that has a substantial negative influence on women's productivity and quality of life globally. Despite their effectiveness, conventional treatments can have unfavorable side effects and limits, which makes safer, natural options necessary. In the end, herbal therapies offer a practical and possibly less costly substitute for prescription medications. This research provides compelling evidence that herbal formulations are a practical and successful natural remedy for menstruation discomfort and related symptoms. Bioactive substances with analgesic, anti-spasmodic, and anti-inflammatory properties are frequently found in herbal remedies, which have their roots in ancient wisdom. They are a very appealing choice because of their potential to reduce symptoms and improve general wellbeing with fewer side effects. To properly incorporate certain herbal compounds into contemporary dysmenorrhea care procedures, future research must concentrate on clarifying their precise mechanisms of action and confirming their effectiveness. The creation and evaluation of innovative, necessary, and comparable items exhibits significant potential for delivering focused, practical, and efficient relief.
REFERENCES

Suyash Salve, Pooja Surve, Chetna Mayekar, Pranay Sawant, Afsana Shaikh, Taskin Shaikh, A Novel Approach on Review of Herbal Formulation to Relive Dysmenorrhea, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 3770-3777, https://doi.org/10.5281/zenodo.19281628
 10.5281/zenodo.19281628
10.5281/zenodo.19281628