Department of Pharmaceutics, Sankaralingam Bhuvaneswari College of Pharmacy, Sivakasi, Tamil Nadu, India. (Affiliated to The Tamil Nadu Dr. M. G.R. Medical University, Chennai).
Skin issues usually get better when liver disease improves or goes into remission, and there isn't a specific treatment for these skin problems. Looking into the skin issues linked to liver disease helps with early diagnosis and treatment, which can lead to better outcomes for patients. Chronic liver disease is a leading cause of illness and death. The most common health issues outside the liver are related to the skin. This review examines various physical and biological connections between psoriasis and non-alcoholic fatty liver disease (NAFLD), highlighting the latest scientific findings. It stresses the need for a team approach in treating patients with psoriasis and discusses treatment options for those dealing with both psoriasis and NAFLD, weighing the benefits and risks of both biologic and non-biologic therapies. Exploring skin problems related to liver disease aids in early diagnosis and treatment, which may enhance patient outcomes. Invasomal carriers present many challenges but also open up new opportunities for research and the development of better therapies in the future.
Many signs of liver disease can be seen on the skin. The liver is the second most important organ in the human body after the skin. Some skin issues may be linked to liver disease, including jaundice (yellowing of the skin), itching (pruritus), spider nevi (spider-like blood vessels on the skin), and changes in skin colour or texture. Other skin problems such as acne, eczema, and psoriasis can also get worse due to liver dysfunction. There are several skin disorders outside the liver that are connected with autoimmune hepatitis (AIH). The most common include a maculopapular rash, psoriasis, vitiligo, impetigo, lichen planus, erythema nodosum, pyoderma gangrenosum, and vasculitis. Eosinophilic annular erythema (EAE) is a type of rash that has been linked to some chronic illnesses and cancers. The study aimed to look at how hepatitis C virus infection (HCV) affects the skin.[1-8] Various skin changes are associated with HCV infection and often do not show symptoms. Like other conditions outside the liver, skin changes frequently occur in chronic Hepatitis C Virus infections. Commonly associated skin diseases with HCV include cutaneous vasculitis, porphyria cutanea, and oral lichen planus; however, other issues like itching, hives, and Raynaud’s phenomenon may also relate to HCV. Both acute and chronic liver diseases can show signs on the skin. These signs can range from subtle changes like early finger clubbing to more noticeable ones such as jaundice. Recognizing these changes early can help lead to quick diagnosis and treatment of the underlying issue. In this pictorial review, we will showcase the skin manifestations of specific liver conditions with suitable images.
Invasomes
Invasomes are tiny liposomal vesicles that contain small amounts of ethanol and terpenes or mixtures of terpenes. These vesicles can help carry substances through the skin more effectively. They penetrate the skin better than liposomes and ethasomes. Invasomes have several benefits, such as making drugs work better and increasing patient comfort and adherence to treatment.
Comparison Of Invasomes In Other Vesicles:
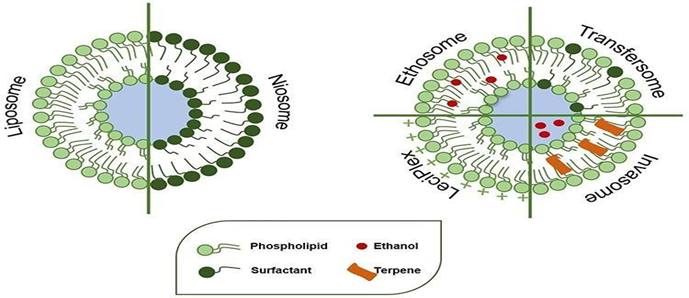
Figure1: Comparisons of Invasomes
ADVANTAGES:
DISADVANTAGES:
Structure And Composition Of Invasomes
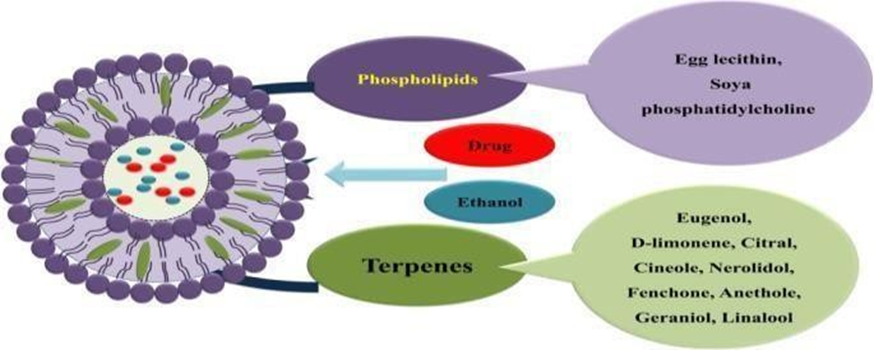
Figure 2: Composition of Invasomes
Applications :
Skin Anatomy
The skin serves as the body's main defence against harmful invaders, making it the largest and most important organ. The stratum corneum (SC), which is the toughest layer for drugs to penetrate, consists of many layers of keratinocytes and is usually 20–30 micrometers thick. This layer helps keep water in the deeper skin layers and prevents harmful substances from reaching the dermis. The papillary and reticular layers of the dermis are made up of collagen and elastin. Additionally, this layer contains sebaceous (oil) glands and sweat glands. The hypodermis connects the dermis to muscles or bones through a network of connective tissue in the fatty layer beneath the skin. Knowing how the skin is structured and functions is important for creating transdermal drug delivery systems (TDDS).[7,8]
General skin findings in liver disease
Chronic liver disease of any origin can cause typical skin findings.

Figure 3: Skin sign that reveal in Liver
Jaundice
Essential to diagnosing jaundice is recognizing whether the bilirubin is conjugated or unconjugated, which helps pinpoint the primary source as pre hepatic, intra hepatic, or post hepatic. Notably, jaundice aids as a prominent indicator of liver disease and requires careful evaluation to address the impaired excretion or block causing bilirubin build-up[9].
Pruritus
The most common skin issue related to chronic liver disease is known as pruritus. It usually starts on the palms and soles, but can spread to the back, abdomen, and front of the legs.[10] The condition tends to have both intermittent and ongoing patterns, often worsening in the evening.[11] Scratching can lead to additional skin problems like sores and thickened skin. For many patients with liver disease, itching is the most frequent and bothersome symptom, especially for those with conditions related to cholestasis, such as primary biliary cholangitis and benign or malignant obstructive jaundice[12]. It is described as an uncomfortable feeling that makes people want to scratch, caused by different substances acting on nerve endings in the skin. This sensation is particularly affected by the buildup of bile acids, natural opioids, lysophosphatidic acid (LPA), and autotoxin (ATX) activity.
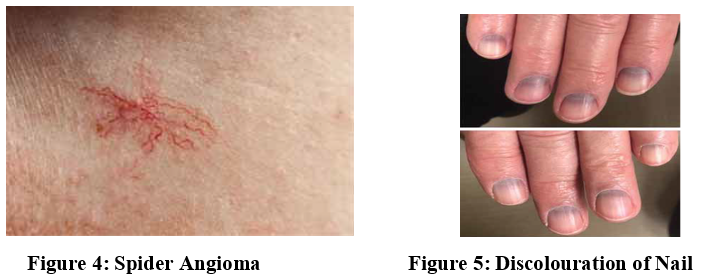
Spider Angioma
Spider angiomas, also called spider nevi or spider telangiectasia, have a central arteriole with tiny vessels spreading out from it. They occur in about 10% of people. Fifteen percent of healthy kids have these issues, and interestingly, 33% of patients with liver cirrhosis do as well.[13] These vascular lesions are usually between 1 to 10 mm in size and mostly show up in places where blood drains into the superior vena cava, such as the face, neck, and upper body. While they are uncommon in mucous membranes, there have been reports of serious cases that involve bleeding or many lesions at once.[14].
Caput medusa
Severe portal hypertension can cause the formation of alternative blood flow routes, resulting in noticeable, twisted veins in the abdomen that extend from the belly button upwards to connect with the body’s main circulation. This condition is called caput medusa (Figure 7) because it resembles the hair of Medusa, which is depicted as being made of snakes. In contrast to what happens with inferior vena cava obstruction, where blood flows towards the head, in caput medusae, blood actually moves toward the legs.[15]

Head of Medusa
Portal hypertension can lead to the development of collateral circulation, causing varies in the oesophagus, stomach, abdomen, and rectum. In cases of portal hypertension, the umbilical vein, which is typically obliterated in initial childhood, may recanalize. Blood from the portal venous system is diverted through the periumbilical veins to the umbilical vein and subsequently to the veins of the abdominal wall, making them prominent [16].
Terry’s Nails
Terry's nails show a clear sign of leukonychia that covers more than 80% of the nail surface, which points to an overgrowth of connective tissue. These nails have a noticeable band at the tip that is pink or brown, ranging from 0.5 to 3 mm wide, indicating expanded blood vessels and tiny dilated veins. Additionally, the lunula is not present. The nails also have a unique ground-glass look due to extra connective tissue in the nail bed.[17]
Muehrcke’s Lines
These are thin, curved, white lines that run parallel to the lunula on the nails. When you press on them, they disappear and are known as apparent leukonychia. You can see them best on the second, third, and fourth fingernails. [18]These lines are linked to nephrotic syndrome and can indicate issues like malnutrition and liver disease. They are also connected to low albumin levels (when albumin concentration is below 2.2 g/dL). However, the exact cause of this condition is still not fully understood. It is thought that swelling in the nail bed raises pressure on the blood vessels in that area, which prevents a normal red colour from showing through the nail. Fortunately, these lines go away once albumin levels return to normal.[18]
Clubbing:
These are convex nails (watch-glass nails), resulting from an increase in both the transverse and longitudinal curvatures of the nail. There are clinical criteria for differentiating between clubbing and pseudo-clubbing. Notably, in clubbing, the Lovibond angle is greater than 180°.
Onycholysis:
Onycholysis is when the nail bed separates from the nail plate. This usually starts at the tip of the nail and appears whitish due to air getting trapped in the gap.[18] There are several reasons for this condition, such as excessive sweating, infections, overall health issues, and certain medications like tetracyclines, capecitabine, 5-fluorouracil, olanzapine, griseofulvin, and birth control pills. If multiple nails are affected, it may indicate a larger health problem. In adults, hyperthyroidism is the most common reason for onycholysis; other possible causes include psoriasis, scleroderma, sarcoidosis, and systemic lupus erythematous. Moreover, research shows a strong link between liver cirrhosis and onycholysis.
Paper Money Skin:
Paper money skin is linked to spider angiomas and shows thin, spread-out capillary spots, usually starting on the person's trunk. This condition has many tiny blood vessels scattered across the skin, which become easier to see during a special examination called diascopy.[19] It is especially found in patients with liver cirrhosis. In these cases, the blood vessels and spider angiomas form a pattern on the upper trunk that looks like the design of paper money, which is how it got its name.[20]
Hair changes:
Changes in hair due to liver disease often show that there are problems with hormones. This can appear as less or thinner hair in the underarms and pubic areas, or men may start to have hair patterns more typical of women. These changes often come with other signs of hormonal shifts, like breast enlargement in men and shrinking testicles. Long-term alcohol abuse is connected to visible signs on the skin, including changes in hair, showing a link between liver issues and big changes in body hair.[21] It can also be a sign of poor nutrition caused by drinking too much alcohol.
Nail change :
Nail changes in liver disease contain clubbing (Figure 9), thickening, longitudinal ridging, the presence of white bands known as Muehrcke’s lines, and brittleness. Terry’s nails, a condition characterised by a white, ground glass appearance of the nail plate with a dark band at the tip, are mainly associated with liver cirrhosis but also with systemic diseases like type 2 diabetes, heart failure and chronic renal failure[22,23]. The absence of the lunula and bluish discolouration of the lunulae, the latter known as Azure lunulae (Figures 6 and 7) in Wilson’s disease, along with splinter haemorrhages and hypertrophic osteopathy, are among other nail changes.
Skin Lesions by Zinc Deficiency in Liver Disease:
Patients with ALD and other forms of liver disease are predisposed to advance the skin lesions of zinc deficiency because of marginal underlying total body zinc stores. Several cases of acrodermatitis also have been reported in alcoholics with or without liver disease who were not receiving zinc in their hyperalimentation solutions or who had inadequate dietary intake of zinc.
Skin Manifestations of Specific Liver Diseases
Hemochromatosis:
Hemochromatosis is a disorder associated with deposits of excess iron that can cause multiple organ dysfunction, usually called ‘bronze diabetes’ due to the discolouration of the skin and related impairment of the pancreas. Primary hemochromatosis is an autosomal recessive hereditary iron overload disorder which predominantly affects males and is among the most common genetic conditions in white populations. Hereditary hemochromatosis occurs in homo-zygotes with a mutation of the hemochromatosis gene (HFE) protein. It may current itself with distinct symptoms such as skin pigmentation, diabetes, cirrhosis, and cardiac failure [24].
Alcohol related liver disease
Dupuytren’s contracture was first explained by the French surgeon Guillaume Dupuytren in the 1830s. While there are various reasons for this condition, it often indicates problems with alcohol use and related liver harm (see Figure 10). There are treatment options besides surgery, such as simvastatin, radiation, and N-acetyl-L-cysteine. Additionally, facial lipodystrophy frequently appears when alcohol takes over most of a person's calorie intake in severe cases of alcoholism[25].
Porphyria cutanea tarda (PCT) is the commonest of the porphyrias and results from deficiency of the enzyme uroporphyrinogen decarboxylase (UROD).The words porphyrin and porphyria come from a Greek term that means purple. A blistering rash forms in areas that are exposed to sunlight, and over time, more hair may grow in those spots. Alcohol is the main trigger for this condition, especially in patients who also have HCV infection, so it’s best to avoid alcohol completely.
Viral hepatitis
One third of patients with chronic HCV infection may have extrahepatic issues, which usually happen in the later stages of the illness. The common skin problems linked to chronic HCV include cryoglobulinemia, polyarteritis nodosa, leucocytoclastic vasculitis, urticaria, and porphyria cutanea tarda. These skin issues are less often seen in HBV infections.
Viral Hepatitis B
Hepatitis B virus (HBV) infections can show a wide variety of skin symptoms. These can include serum sickness-like disease, which affects about 20–30% of people with acute HBV, and polyarteritis nodosa (PAN), seen in 7–8% of cases.[26] Typically, these symptoms appear before any liver problems start, and the serum sickness-like symptoms go away as the HBV antigens are eliminated from the body. HBV-related PAN is marked by immune complexes collecting in the body and can lead to issues in the gastrointestinal tract. The main treatments for this condition include steroids, antiviral medications, and plasma exchange.

Figure 8 : Skin rash in Viral Hepatitis B
Primary Biliary Cirrhosis (PBC)
Xanthelasmas are clusters of fat-filled cells found in the upper and lower eyelids. They can be quite noticeable and usually appear without a known cause. There is a strong link between primary biliary cholangitis (PBC) and high cholesterol levels, which may explain why patients often develop both xanthelasmas and skin bumps called cutaneous xanthomas (5%). Other skin issues related to this disease, though not as common, include dry eyes (sicca syndrome) and vitiligo. Cases of skin darkening (melanosis) and dry skin (xeroderma) have also been reported. In rare instances, PBC can show up with skin inflammation (cutaneous vasculitis).[27]
Nonspecific skin changes:
Cirrhosis, no matter the cause, can lead to various skin issues like itching, yellowing of the skin (jaundice), dry skin, changes in nails, blood vessel changes, and hormonal shifts. The imbalance between oestrogen and androgen due to cirrhosis is thought to cause symptoms like red palms (palmar erythema), spider veins (spider nevi), enlarged breast tissue in men (gynecomastia), shrinkage of testicles, and loss of body hair in males. Fluid buildup in the abdomen (ascites) can result in stretch marks and umbilical hernias. Here are some common skin signs related to cirrhosis.[28]
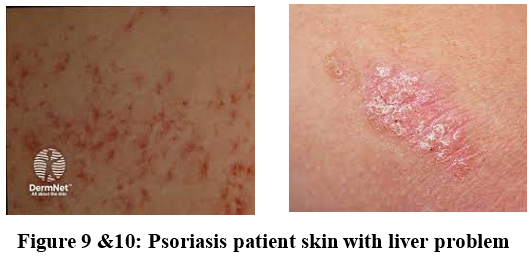
NAFLD And Psoriasis
NAFLD, or Non-Alcoholic Fatty Liver Disease, includes a range of liver problems that go from simple fatty liver (called steatosis) to a more serious condition known as steatohepatitis (NASH). This can eventually lead to cirrhosis and liver cancer. People with psoriasis have a higher chance of developing NAFLD compared to those without the skin condition. Psoriasis is seen as a systemic disease, meaning it affects the whole body and is linked to other health issues like metabolic syndrome. NAFLD is considered the liver's response to metabolic syndrome.Thus, psoriatic patients showed a higher prevalence and incidence of obesity directly correlated to the severity of psoriasis itself. It is known that the increasing prevalence of NAFLD parallels the rise of obesity and its complication. Thus, psoriasis and NAFLD could be linked by obesity itself, as psoriasis and NAFLD, obesity is considered a persistent and low-grade inflammatory process. The adipose tissue accumulation seems to lead to adipocyte hypertrophy and hyperplasia with a sort of local ischemia; subsequently an inflammatory process and the release of pro-inflammatory chemokines start, attracting macrophages which amplify and spread the inflammatory process in neigh boring adipocytes. Furthermore, a recent meta-analysis has documented that patient with PsA and patients with moderate to severe psoriasis showed a significantly greater risk of NAFLD compared with those with mild psoriasis. Psoriasis and psoriasis-related comorbidities significantly impact on patient’s health and quality of life and negatively interfere in physical-psychic well-being with important repercussion in working daily life. As a multi-organ pathology, psoriasis needs a multidisciplinary approach and clinicians should evaluate this holistic vision in order to promptly identify and manage psoriasis related comorbidities influencing patients’ morbidity and mortality [29,30]. Therefore, the therapeutic strategy for psoriasis should be multifaceted and should specifically tailor outcome tools and disease-related items by a patient based evaluation and by selectively verifying the risk/ benefit of each single therapeutic option.
CONCLUSION
In summary, liver diseases can show up as various changes in the skin, either from cirrhosis or specific liver problems. Doctors need to identify these signs and symptoms because skin changes can be an early indication of a hidden liver issue. One method that shows promise is the creation of invasomes, which may be an effective way to deliver medication through the skin and can allow for better absorption than liposomes. Invasomes have been used to hold both water-loving and water-repelling drugs. Therefore, they present new challenges and chances for developing better treatments.
REFERENCES

K. Shobana*, Dr. M. Rajesh, R. Pandimeenal, M. Rajeswaran, P. Sri Ragavi, B. Vel Ramar, Invasomes – A Novel Carrier to Combat Dermatological Manifestation in Patients with Hepatic Disease, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 5775-5785. https://doi.org/10.5281/zenodo.15771290
 10.5281/zenodo.15771290
10.5281/zenodo.15771290
