
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Sigma Institute of Pharmacy, Ajwa Nimeta Road Bakrol, Vadodara- 390019, Gujarat, India
Liquid biopsy has emerged as a transformative tool in oncology, offering a minimally invasive method for detecting, monitoring, and understanding cancer through biomarkers circulating in body fluids, such as blood, urine, and saliva. Unlike traditional tissue biopsies, which are invasive, risky, and often limited by sampling errors, liquid biopsy enables dynamic and real-time insights into tumour evolution. This review comprehensively explores the biological basis, technological innovations, and clinical applications of liquid biopsy, with a focus on circulating tumour DNA (ctDNA), circulating tumour cells (CTCs), and exosomes. We also highlight emerging analytes, such as tumour-educated platelets and cell-free RNA. The human dimension of liquid biopsy is emphasised, underscoring its potential to reduce the patient burden, democratize access to diagnostics, and align science with compassion. Finally, we discuss challenges, ethical considerations, and future directions, envisioning a healthcare landscape in which a simple blood draw could replace invasive procedures and transform patient outcomes.
According to the World Health Organization (WHO), cancer remains a global health challenge, accounting for nearly 10 million deaths in 2020. [1] Despite advances in molecular oncology, the ability to diagnose cancer early, monitor its evolution, and guide treatment remains limited by reliance on traditional tissue biopsy and imaging. Tissue biopsy, although considered the “gold standard,” has significant limitations. It is invasive, carries risks of complications, such as bleeding and infection, and often fails to capture the spatial and temporal heterogeneity of tumors. [2] Imaging techniques, which are less invasive, are restricted by resolution thresholds and cannot provide real-time molecular information.
Liquid biopsy - the analysis of tumor-derived material in body fluids such as blood, urine, or saliva–has emerged as a powerful complement to these traditional methods. [3] First conceptualized in the 1990s, the field has advanced rapidly with the discovery that tumor DNA fragments circulate in plasma and that intact tumor cells and extracellular vesicles can be isolated from the blood. [4] Unlike tissue biopsy, liquid biopsy allows for serial sampling, capturing the evolving genomic landscape of tumors and enabling real-time monitoring of the disease. [5]
In addition to its technical advantages, liquid biopsy embodies a more human-like approach to cancer care. For patients, it reduces the physical and psychological burdens associated with repeated invasive procedures. Clinicians can identify dynamic biomarkers that can guide treatment adjustments with greater precision. Health systems hold the promise of cost-effective cancer surveillance programs, especially as technologies become more affordable and scalable. [6, 7, 8]
2. BIOLOGICAL BASIS OF LIQUID BIOPSY
2.1 Circulating Tumour DNA (ctDNA)
Circulating tumor DNA consists of short DNA fragments (typically 150–200 bp) released into the bloodstream from apoptotic, necrotic, or actively secreting tumor cells. [9] ctDNA harbor the same genetic and epigenetic alterations as tumors of origin, including point mutations, copy number variations, structural rearrangements, and methylation changes. The proportion of ctDNA within the pool of cell-free DNA (cfDNA) varies from <0.1% in early stage cancers to >90% in advanced diseases. [10] Detection of ctDNA requires highly sensitive technologies capable of distinguishing rare mutant alleles from a vast background of normal cfDNA. Methods include digital PCR, droplet digital PCR, and next-generation sequencing (NGS) with error-correction algorithms.[11] Methylation-based assays further enhance sensitivity and tissue-of-origin prediction.[12] Clinically, ctDNA has been employed for early detection (e.g., Galleri multi-cancer test), minimal residual disease (MRD) monitoring in colorectal and lung cancers, and detection of resistance mutations such as EGFR T790M in non-small-cell lung cancer (NSCLC).[13, 14, 15]

Figure 1 ctDNA (Circulating Tumour DNA)
2.2 Circulating Tumour Cells (CTCs)
CTCs are intact tumor cells that are shed into the bloodstream from primary or metastatic sites. Their rarity (as few as 1 CTC per billion blood cells) makes their detection challenging but also highly specific. [16] Isolation strategies rely on physical properties (size, density, and deformability) or biological markers, such as EpCAM expression.[17] The CellSearch® system remains the only FDA-approved CTC detection platform and has been validated for prognostication of metastatic breast, colorectal, and prostate cancers. [18]
CTCs provide insights beyond DNA mutations and offer opportunities for transcriptomic, proteomic, and functional analyses at the single-cell level. Studies have demonstrated their utility in predicting metastasis, guiding therapeutic selection, and understanding the mechanisms of drug resistance. [19, 20, 21]

Figure 2 CTCs (Circulating tumour cells)
2.3 Exosomes and Extracellular Vesicles
Exosomes are small extracellular vesicles (30–150 nm) secreted by tumour and stromal cells. They carry proteins, lipids, RNA, and DNA, reflecting the molecular composition of the tumour microenvironment. [22] Exosomal cargoes, such as miR-21 and glypican-1, have shown diagnostic potential in pancreatic, breast, and lung cancers. [23, 24] The isolation techniques include ultracentrifugation, immunoaffinity capture, and microfluidic platforms. [25] The stability of exosomes in circulation makes them particularly attractive for biomarker discovery. Beyond diagnosis, exosomes play active roles in tumour progression, including angiogenesis, immune evasion, and the preparation of pre-metastatic niches.[26, 27]
Table 1. Key biomarkers used in liquid biopsy.
|
Biomarker |
Source |
Clinical Relevance |
Detection Methods |
|
Circulating tumour DNA (ctDNA) |
Plasma, serum |
Early detection, monitoring, minimal residual disease |
ddPCR, NGS, methylation assays |
|
Circulating tumour cells (CTCs) |
Blood |
Prognosis, therapy resistance, metastatic spread |
CellSearch, microfluidics, imaging |
|
Exosomes |
Plasma, serum, urine |
Cancer diagnosis, intercellular signalling, therapy response |
Ultracentrifugation, immunocapture, NTA |
|
Circulating RNA (miRNA, lncRNA) |
Blood, urine |
Non-invasive biomarkers for tumour subtype and progression |
qRT-PCR, NGS |
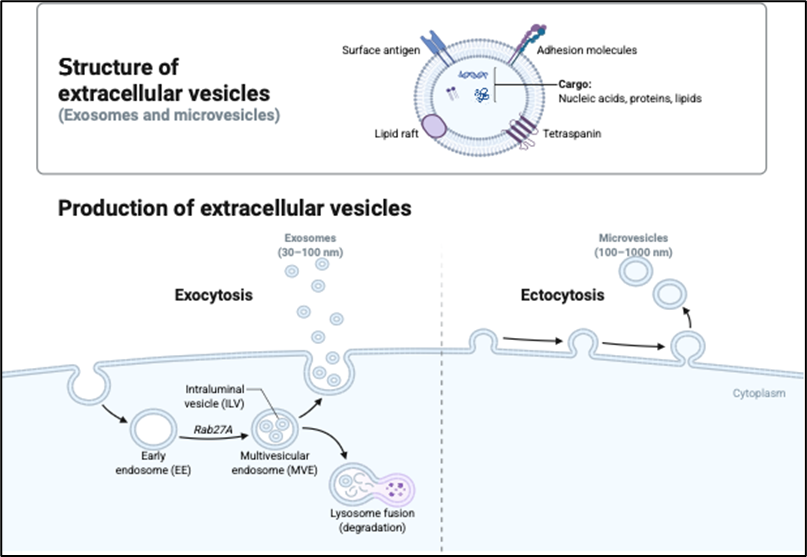
Figure 3 Extracellular Vesicles
2.4 Emerging Analytes
Recent studies have expanded the repertoire of liquid biopsy analytes. Tumor-educated platelets (TEPs) undergo RNA splicing changes in response to tumor-derived signals, offering diagnostic signatures across multiple cancer types. [28] Circulating RNAs (including microRNAs, long non-coding RNAs, and circular RNAs) serve as stable biomarkers with the potential for early detection. [29] Extrachromosomal circular DNA (eccDNA) reflects oncogene amplification and heterogeneity [30] while circulating mitochondrial DNA correlates with tumor burden and prognosis.[31] Non-blood sources, such as urine (for bladder and kidney cancers) and saliva (for oral cancers), are also gaining attention as needle-free alternatives.[32]
3. DETECTION TECHNOLOGIES
The clinical potential of liquid biopsy is inseparable from the analytical methods used to capture, enrich, and characterize tumor-derived materials. Because circulating biomarkers are typically rare and exist in a background of abundant non-tumor components, detection technologies require extraordinary sensitivity and specificity. Over the past two decades, significant advances have been made in molecular biology, sequencing, and microfluidics, enabling the detection of circulating tumor DNA (ctDNA), circulating tumor cells (CTCs), and extracellular vesicles at clinically actionable levels.
3.1 Polymerase Chain Reaction (PCR)-based methods
Polymerase chain reaction (PCR) is one of the foundational technologies in molecular oncology. Techniques such as allele-specific PCR and real-time quantitative PCR (qPCR) allow the detection of known hotspot mutations in ctDNA with sensitivities as low as ~1% mutant allele fraction (MAF). [33] However, qPCR is limited when the mutation profiles are complex or unknown. Digital PCR (dPCR) and its more advanced form, droplet digital PCR (ddPCR), have revolutionised ctDNA analysis. By partitioning the samples into thousands of microdroplets, ddPCR allowed the absolute quantification of rare mutant alleles against a wild-type background. [34] Sensitivity reaches ~0.01% MAF, making it suitable for minimal residual disease monitoring in leukaemia and early-stage solid tumours. [35] ddPCR is relatively inexpensive and rapid, but is restricted to interrogating a limited number of genomic loci per assay. [36] Another innovation is BEAMing (Beads, Emulsion, Amplification, Magnetics), which combines emulsion PCR with flow cytometry. BEAMing has demonstrated robust performance in detecting KRAS and PIK3CA mutations in colorectal cancer. [37]

Figure 4 Identification techniques PCR (Polymerase Chain Reaction)
3.2 Next-Generation Sequencing (NGS)
NGS has transformed liquid biopsies by enabling the comprehensive genomic profiling of ctDNA. These approaches include targeted sequencing panels, whole-exome sequencing (WES), and whole-genome sequencing (WGS).
Targeted NGS panels, such as Guardant360 and FoundationOne Liquid, focus on cancer-relevant genes and balance breadth with the depth of sequencing. [38] Deep coverage (>10,000×) allows the detection of rare variants with allele frequencies as low as 0.1%. Hybrid-capture enrichment strategies improve coverage uniformity across loci.
Error-corrected NGS methods further enhance sensitivity by using unique molecular identifiers (UMIs) to distinguish true variants from PCR/sequencing artifacts. [39] Duplex sequencing, which requires concordant variant calls from both DNA strands, has a sensitivity approaching 1 in 10? DNA molecules. [40]
In addition to single-nucleotide variants, NGS enables the detection of copy number alterations, structural variants, and methylation patterns. Methylation-based multi-cancer detection assays, such as the Galleri test (GRAIL) and PanSeer, have shown promise for the early detection of multiple cancer types from a single blood draw. [41, 42]
The limitations of NGS include high cost, complex bioinformatics requirements, and relatively long turnaround times. Furthermore, distinguishing tumour-derived mutations from clonal hematopoiesis of indeterminate potential (CHIP) remains a challenge. [43]
3.3 Methylation and Epigenetic Assays
DNA methylation patterns are tissue- and cancer-specific, making them powerful biomarkers for both detection and tissue of origin prediction. [44] Techniques such as bisulfite sequencing, methylated DNA immunoprecipitation sequencing (MeDIP-seq), and cfMeDIP-seq have been adapted for ctDNA analysis. [45]
Large consortia efforts, including the Circulating Cell-free Genome Atlas (CCGA), have validated methylation-based classifiers for pan-cancer detection. For instance, Liu et al. demonstrated >90% specificity across >50 cancer types by using cfDNA methylation signatures. [46]
Epigenetic assays are also being developed to include nucleosome positioning and histone modification patterns. These chromatin features, detected from cfDNA fragmentation profiles, provide additional layers of biological insight and may help resolve tumor tissues of origin in ambiguous cases. [47]
3.4 Technologies for Circulating Tumour Cells
Detection of CTCs presents unique technological hurdles owing to their extreme rarity in the blood. Platforms can be broadly categorized as biological property-based and physical property-based. The CellSearch® system, based on the immunomagnetic capture of EpCAM-positive cells, is the only FDA-cleared technology for CTC detection.[48] It has demonstrated prognostic value in breast, prostate, and colorectal cancer. However, reliance on EpCAM expression excludes mesenchymal-like CTCs that downregulate epithelial markers during epithelial-to-mesenchymal transition (EMT). [49]
Alternative approaches include size-based filtration devices (e.g., ISET, ScreenCell) that exploit the larger diameter of CTCs than leukocytes. [50] Microfluidic devices, such as the CTC-iChip, combine hydrodynamic sorting with magnetic separation, allowing high-throughput enrichment with minimal cell loss. [51]
Downstream analysis of CTCs extends beyond enumeration to single-cell RNA sequencing, proteomic profiling, and functional assays. This enables the exploration of intra-patient heterogeneity, metastatic competence, and mechanisms of therapeutic resistance. [52, 53]

Figure 5 Cell Search System
Table 2. Technologies for liquid biopsy analysis.
|
Technology |
Description |
Advantages |
Limitations |
|
ddPCR |
Partitioned PCR allowing absolute quantification |
High sensitivity |
Limited multiplexing |
|
NGS |
High-throughput sequencing of ctDNA |
Detects broad spectrum of mutations |
Expensive, bioinformatic burden |
|
BEAMing |
Beads, Emulsion, Amplification, Magnetics |
Highly sensitive detection of rare alleles |
Technically complex |
|
Methylation profiling |
Detects epigenetic signatures |
Enables multi-cancer detection |
Still in validation stage |
3.5 Exosome and Extracellular Vesicle Platforms
The isolation of exosomes is technically demanding because of their small size and overlap with other vesicle populations. Ultracentrifugation remains the gold standard; however, it is labour-intensive and unsuitable for clinical workflows. [54] Emerging alternatives include:
Once isolated, exosomes can be characterised by RNA sequencing, mass spectrometry, or digital ELISA. Several studies have demonstrated that exosomal RNA signatures are predictive of pancreatic cancer and glioblastoma. [56, 57]
Exosome analysis remains less standardised than ctDNA or CTC assays, and inter-laboratory variability is significant. However, technological innovations such as the ExoDx Prostate (IntelliScore), an exosomal RNA test for prostate cancer risk assessment, are moving into the clinic. [58]
3.6 Multi-omic and Integrative Approaches
No single analyte captures the full complexity of tumor biology. Thus, multi-omic strategies are increasingly employed. For example, combining ctDNA mutation detection with methylation profiling enhances the sensitivity and specificity for early detection. [59] Integrating exosomal RNA and protein analysis with ctDNA further refines tissue-of-origin prediction.
Artificial intelligence (AI) and machine learning (ML) tools are critical for analyzing high-dimensional liquid biopsy data. Deep learning models have been trained on cfDNA fragmentation patterns, methylation profiles, and multiomic inputs, achieving unprecedented performance in cancer classification. [60] These integrative approaches represent the future of precision oncology diagnosis.
3.7 Technical Challenges and Standardisation
Despite remarkable progress, several technical challenges remain:
To address these issues, international consortia such as BloodPAC and the European Liquid Biopsy Society (ELBS) are developing consensus standards for assay design, validation, and reporting. [64] Regulatory frameworks are also evolving, with increasing numbers of liquid biopsy tests receiving FDA breakthrough designation.
4. CLINICAL APPLICATIONS OF LIQUID BIOPSY
Liquid biopsy has advanced beyond experimental proof-of-concept to become a valuable clinical tool in oncology. Its applications extend across the entire cancer continuum, from early detection to treatment monitoring and surveillance of minimal residual disease (MRD). In this section, we systematically explore the clinical settings in which liquid biopsy is currently used or being evaluated, highlighting strengths, limitations, and representative studies.
4.1 Early Detection and Screening
The promise of liquid biopsy is perhaps the most transformative in early cancer detection, when conventional diagnostic methods often fail. Most cancers are diagnosed at advanced stages when the prognosis is poor.
Detecting malignancy at an asymptomatic or preclinical stage can dramatically reduce mortality. ctDNA analysis has shown the potential for identifying cancer before imaging or clinical symptoms. The Galleri test, which is based on cfDNA methylation profiling, demonstrated the ability to detect >50 cancer types with high specificity (>99%). [65]
In a study of 6,689 participants, the test achieved a positive predictive value of 44% for detecting cancer signals and, importantly, could predict tissue-of-origin in 93% of cases where cancer was confirmed. [66]
Similarly, the PanSeer assay, which profiles methylation patterns of cfDNA, detected cancers up to four years before conventional diagnosis in a large cohort study. [67] Other approaches, such as CancerSEEK, integrate ctDNA mutation analysis with protein biomarkers, achieving sensitivities ranging from 69% for stage II cancers to 43% for stage I.[68]
Population-wide screening presents logistical challenges, including cost, false positives, and the risk of overdiagnosis. However, focused use in high-risk groups, such as individuals with hereditary cancer syndromes (e.g., BRCA1/2 and Lynch syndrome), is already being trialled. [69]
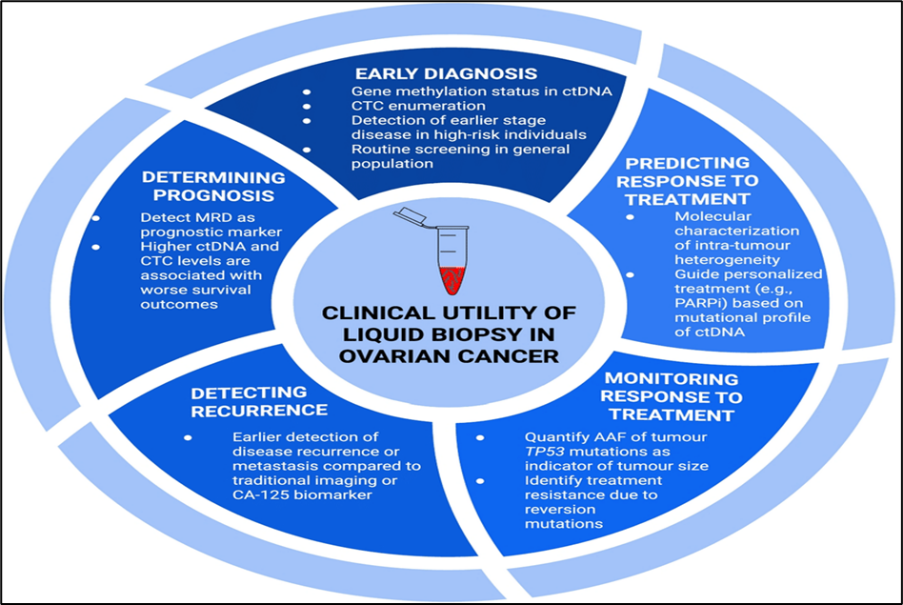
Figure 6 Applications Of Liquid Biopsy
4.2 Prognostication
Liquid biopsy provides prognostic information by quantifying tumour burden and monitoring dynamics over time. In metastatic breast cancer, elevated CTC counts (>5 cells per 7.5 mL blood) measured by CellSearch® correlated strongly with reduced overall survival. [70] ctDNA levels in advanced colorectal cancer correlate with tumor volume and predict progression-free survival more accurately than carcinoembryonic antigen (CEA). [71] Moreover, dynamic changes in ctDNA levels can provide prognostic information. In lung cancer, patients with rapid ctDNA clearance following targeted therapy exhibit significantly improved progression-free and overall survival compared to those with persistent ctDNA clearance. [72]
4.3 Minimal Residual Disease (MRD)
Detecting MRD, residual cancer cells that remain after treatment and may cause relapse, is a critical application of liquid biopsy. Tissue biopsies and imaging lack the sensitivity to detect MRD at a very low disease burden, but ctDNA assays can identify mutant alleles present at <0.01% MAF. [73] In colorectal cancer, the DYNAMIC trial demonstrated that ctDNA-guided adjuvant therapy decision-making was non-inferior to standard clinicopathological risk stratification. Patients with a ctDNA-negative status can safely avoid chemotherapy without compromising outcomes. [74] In non-small-cell lung cancer, postsurgical ctDNA positivity strongly predicts relapse months before radiographic evidence. One prospective study showed that ctDNA detection preceded imaging-confirmed recurrence by a median of 5.2 months. [75] Leukaemias are particularly well-suited for ctDNA-based MRD monitoring, complementing flow cytometry and other molecular techniques. Ultra-sensitive assays now permit longitudinal monitoring of therapeutic effectiveness and risk of relapse. [76]
4.4 Monitoring Treatment Response
Liquid biopsy enables the real-time assessment of therapeutic efficacy. Traditional imaging methods often require months before changes in the tumour burden are visible, whereas ctDNA levels reflect treatment effects within days to weeks. For instance, in NSCLC treated with EGFR inhibitors, rapid declines in ctDNA levels within two weeks of therapy initiation predict a clinical response. [77] Similar results have been reported in melanoma patients treated with immune checkpoint inhibitors; declining ctDNA levels correlate with improved outcomes, whereas rising levels often precede radiographic progression. [78] CTCs can also provide functional information regarding treatment response. In prostate cancer, changes in CTC counts have been validated as surrogate endpoints for overall survival in clinical trials. [79] Exosomal RNA signatures have been shown to reflect early responses to chemotherapy in breast and ovarian cancer. [80]
4.5 Detection of Therapeutic Resistance
Resistance to therapy remains a challenge in oncology. Liquid biopsy enables the early identification of resistance mutations, often before radiographic or clinical progression.
In NSCLC, ctDNA testing for EGFR T790M mutation has become routine, guiding the switch to osimertinib in patients with acquired resistance to first- and second-generation EGFR inhibitors. [81]
Detection of ALK and ROS1 resistance mutations in ctDNA similarly informs targeted therapy adjustments. [82]
In colorectal cancer, KRAS mutations detected in ctDNA predict resistance to anti-EGFR therapy months before clinical relapse.[83]
Similarly, androgen receptor splice variants detected in CTCs predict resistance to enzalutamide and abiraterone in prostate cancer. [84]
Monitoring resistance dynamics allows adaptive therapeutic strategies, such as drug rechallenge, when resistant clones decay after treatment withdrawal. This “real-time” oncology represents a paradigm shift in treatment individualisation. [85]
4.6 Applications in Immuno-oncology
Immunotherapy has transformed cancer care, but benefits only a subset of patients. Liquid biopsy offers biomarkers for predicting response and monitoring efficacy. Tumor mutational burden (TMB) derived from ctDNA correlates with immunotherapy response in NSCLC and melanoma. [86] Dynamic ctDNA levels reflect the response to checkpoint inhibitors more rapidly than imaging does, particularly in cases of pseudoprogression. [87]
Exosomal PD-L1 levels have been proposed as predictors of response to PD-1/PD-L1 blockade. [88] Additionally, circulating T-cell receptor (TCR) repertoire profiling from cfDNA may provide insights into immune dynamics. [89]
4.7 Paediatric and Rare Cancers
Paediatric cancers often present unique challenges, including limited tissue availability and ethical concerns regarding invasive biopsies. Liquid biopsy provides a less burdensome alternative. In paediatric medulloblastoma, ctDNA detection in cerebrospinal fluid (CSF) has been shown to reflect disease burden and predict relapse.[90] Similarly, in diffuse midline glioma, CSF ctDNA analysis captures H3K27M mutations for diagnosis and monitoring.[91] Rare cancers such as sarcomas, which lack reliable biomarkers, may benefit from liquid biopsy-guided surveillance. Exosomal microRNAs have shown promise in detecting osteosarcoma relapse.[92]
4.8 Cancers in “Hard-to-Biopsy” Sites
Certain cancers, including brain tumours and lung lesions, are difficult or risky to biopsy. Liquid biopsy offers a safer alternative for molecular profiling. In glioblastoma, CSF ctDNA analysis provides insights into tumour genomics when surgical biopsy is infeasible.[93] For lung cancer patients unable to undergo invasive biopsies, plasma ctDNA assays now serve as clinically validated substitutes for genotyping.[94]
4.9 Population Screening and Surveillance
The ultimate vision of liquid biopsy is population-wide cancer screening through routine blood draws. Several large-scale studies are underway. The UK’s Galleri trial, involving 140,000 participants, is testing multi-cancer early detection in asymptomatic individuals.[95] Parallel efforts in the US (PATHFINDER trial) and China (PanSeer expansion studies) aim to establish real-world utility.[96] Surveillance of cancer survivors also benefits from liquid biopsy. For example, ctDNA detection after curative therapy in colorectal and breast cancer patients provides early warning of relapse and informs surveillance intensity.[97, 98]
4.10 Integration into Clinical Decision-Making
Clinical guidelines increasingly incorporate liquid biopsy. The National Comprehensive Cancer Network (NCCN) endorses ctDNA testing for EGFR mutations in NSCLC when tissue is insufficient.[99] The European Society for Medical Oncology (ESMO) has similarly issued recommendations on liquid biopsy use for actionable mutations.[100]
Integration into multidisciplinary tumour boards ensures liquid biopsy results are contextualised with imaging, histopathology, and clinical presentation. The paradigm shift lies in moving from a static “one biopsy, one decision” approach to dynamic, serial monitoring that informs adaptive treatment strategies.
Table 3. Clinical applications of liquid biopsy.
|
Application |
Cancer Types |
Clinical Impact |
|
Early detection |
Colorectal, lung, breast, pancreatic |
Improves survival by identifying cancers earlier |
|
Prognosis |
Breast, lung, prostate |
Stratifies patients for tailored therapy |
|
Therapy monitoring |
NSCLC, colorectal, melanoma |
Tracks resistance mutations (EGFR, KRAS, BRAF) |
|
Minimal residual disease |
Colorectal, breast |
Predicts relapse before imaging detects it |
5. LIMITATIONS AND CHALLENGES OF LIQUID BIOPSY
Despite its transformative potential, liquid biopsy is not without limitations. Widespread clinical adoption requires careful consideration of technical, biological, economic, and ethical challenges. Understanding these constraints is critical for contextualising liquid biopsy results in patient care and guiding future research.
5.1 Sensitivity and Specificity
One of the foremost limitations of liquid biopsy lies in sensitivity. Early-stage cancers shed very small amounts of ctDNA or CTCs into circulation. In some cases, ctDNA levels may be as low as one mutant copy per millilitre of plasma. [101] Even highly sensitive assays such as ddPCR and duplex sequencing struggle to achieve reliable detection at these levels. Consequently, false negatives remain a major concern in screening and MRD settings. Specificity is equally important. False positives may arise from benign conditions, inflammatory processes, or clonal haematopoiesis of indeterminate potential (CHIP). [102] CHIP is particularly problematic in older populations, where age-related somatic mutations in haematopoietic stem cells mimic tumour-derived mutations. Distinguishing CHIP from true tumour mutations requires orthogonal testing or integration of additional biomarkers. [103]
5.2 Biological and Pre-analytical Variability
Liquid biopsy analytes are subject to biological variability. ctDNA half-life in circulation is only 1–2 hours, meaning levels fluctuate rapidly with tumour activity and treatment. [104] CTC shedding may be intermittent, influenced by tumour vascularisation and microenvironment dynamics. Pre-analytical variables further complicate interpretation. Blood collection tubes, time to plasma separation, and storage conditions significantly impact cfDNA integrity. [105] For exosome studies, different isolation methods yield heterogeneous vesicle populations, hindering reproducibility. [106] Without standardisation, inter-laboratory variability undermines comparability of results.
5.3 Incomplete Capture of Tumour Heterogeneity
While liquid biopsy provides a more comprehensive snapshot of tumour heterogeneity than a single tissue biopsy, it may still fail to capture all subclones. Some tumours shed more DNA or cells into circulation than others, depending on anatomical location, vascularisation, and biological behaviour. [107] For example, brain tumours are partly protected by the blood–brain barrier, which limits the release of ctDNA into plasma. In such cases, cerebrospinal fluid (CSF) may be a more informative medium. [108]
5.4 Cost and Accessibility
High costs remain a barrier to widespread implementation. Commercial ctDNA assays such as Guardant360 and FoundationOne Liquid can cost several thousand US dollars per test. [109] While prices are expected to decline with technological advances, affordability in low- and middle-income countries remains a major concern. Reimbursement policies are inconsistent. Some health systems cover specific liquid biopsy tests (e.g., EGFR mutation testing in NSCLC), but broad coverage for early detection or MRD monitoring is rare. [110] Without clear demonstration of cost-effectiveness and survival benefit in prospective trials, payers may be reluctant to adopt liquid biopsy at scale.
5.5 Regulatory and Standardisation Barriers
Regulatory approval of liquid biopsy assays requires robust analytical validation and clinical utility demonstration. Yet, most assays remain laboratory-developed tests (LDTs) with variable performance characteristics. [111] Regulatory frameworks differ globally; while the US FDA has cleared certain assays (e.g., Cobas EGFR Mutation Test v2), Europe has multiple CE-IVD labelled platforms, but harmonisation is lacking. [112]
Standardisation efforts are underway through initiatives such as BloodPAC and European Liquid Biopsy Society, which aim to establish consensus protocols for sample handling, assay validation, and data reporting. [113] Until universally accepted standards are implemented, inter-trial comparisons and meta-analyses will remain challenging.
5.6 Clinical Interpretation and Integration
Liquid biopsy results must be interpreted in clinical context. Detection of ctDNA mutations may not always indicate clinically actionable disease. For example, a detected mutation might represent clonal haematopoiesis rather than tumour progression. [114] Conversely, absence of ctDNA does not guarantee absence of disease, particularly in low-shedding cancers.
Integrating liquid biopsy into existing diagnostic pathways requires careful planning. Over-reliance on liquid biopsy without confirmatory imaging or histology could lead to mismanagement. Conversely, under-utilisation risks missing opportunities for early intervention. Multidisciplinary tumour boards play a critical role in contextualising results alongside radiological, histopathological, and clinical data. [115]
5.7 Ethical Considerations
Liquid biopsy introduces ethical dilemmas around incidental findings and overdiagnosis. Population-wide screening may detect indolent tumours that would never have become clinically significant, leading to overtreatment and psychological distress. [116] Similarly, identifying genetic alterations without available therapies could generate anxiety without clinical benefit. Genomic privacy is another concern. Liquid biopsy generates large datasets, including germline information, raising questions about data security, consent, and secondary use by insurers or employers. [117] Clear regulatory frameworks and transparent communication with patients are essential.
5.8 Equity and Global Health Challenges
While liquid biopsy promises democratisation of cancer diagnostics, current implementation risks widening global health disparities. High costs, limited infrastructure, and dependence on advanced sequencing platforms restrict access in resource-constrained settings. [118]MDeveloping simplified, low-cost platforms (e.g., PCR-based assays, microfluidic chips) could extend benefits to underserved populations. However, ensuring equitable access will require not only technological innovation but also policy initiatives and international collaboration.[119]
6. FUTURE PERSPECTIVES IN LIQUID BIOPSY
Liquid biopsy is already reshaping cancer diagnostics, yet its future potential extends far beyond current clinical use. With rapid advances in multi-omics, artificial intelligence (AI), and novel biomarker discovery, liquid biopsy could soon become a routine tool for cancer screening, monitoring, and personalised therapy worldwide. This section explores emerging directions that are likely to define the next decade of innovation.
6.1 Multi-omics Integration
Most current liquid biopsy assays focus on a single analyte — typically ctDNA. However, cancer biology is far too complex to be captured by one molecular layer alone. Integrating multi-omic data — including genomics, epigenomics, transcriptomics, proteomics, and metabolomics — promises a more comprehensive view of tumour biology.[120] For example, combining ctDNA mutation analysis with cfDNA methylation profiles improves both sensitivity and tissue-of-origin prediction. Integrating exosomal RNA with plasma proteomics enhances classification accuracy in pancreatic and ovarian cancers. [121] Similarly, CTC analysis provides functional insights, while ctDNA reflects genomic alterations. A truly multi-omic liquid biopsy would capture complementary signals, reducing false negatives and maximising diagnostic yield. Large consortia such as the Cancer Moonshot Initiative and European Liquid Biopsy Society are investing in multi-omic studies to validate these approaches at scale. [122]
6.2 Artificial Intelligence and Machine Learning
The explosion of high-dimensional data from liquid biopsy requires advanced computational approaches. AI and machine learning (ML) have emerged as indispensable tools for pattern recognition and predictive modelling. Deep learning algorithms trained on cfDNA fragmentation profiles can distinguish cancer patients from healthy controls with >95% accuracy. [123] ML models integrating methylation, fragmentation, and mutation data outperform single-modality assays in multi-cancer detection. [124] AI also enables longitudinal tracking of patients, predicting relapse based on subtle ctDNA changes undetectable by standard thresholds. [125] In the future, AI-driven decision-support tools may provide clinicians with real-time interpretations of liquid biopsy data integrated with imaging and electronic health records.
6.3 Point-of-care and Portable Platforms
For liquid biopsy to reach its full potential, especially in resource-limited settings, assays must move from centralised laboratories to point-of-care (POC) platforms. Advances in microfluidics, lab-on-a-chip devices, and nanopore sequencing make this increasingly feasible. [126] Handheld nanopore sequencers can already perform targeted sequencing in near real-time, and portable PCR-based assays can detect known mutations at low cost. [127] Integration of smartphone-based imaging with microfluidic chips enables on-site CTC enumeration without specialised infrastructure. [128] The development of affordable, portable liquid biopsy platforms could democratise access to advanced diagnostics, extending benefits beyond tertiary centres to rural and low-income regions.
6.4 Emerging Biomarkers
While ctDNA, CTCs, and exosomes dominate current liquid biopsy research, several emerging biomarkers hold promise for the future.
Expanding the biomarker repertoire will enhance sensitivity, particularly for cancers with low ctDNA shedding.
6.5 Liquid Biopsy in Cancer Prevention and Interception
Future applications of liquid biopsy may extend beyond detection to prevention and interception. Identifying pre-malignant lesions or high-risk clonal expansions before cancer develops could open avenues for early intervention.
For instance, CHIP mutations detected in plasma may signal increased risk for haematological malignancies and cardiovascular disease.[133] Monitoring such signals could enable targeted surveillance or prophylactic therapies. Similarly, detecting high-risk adenomas via ctDNA methylation may support early intervention before progression to colorectal cancer.[134]
6.6 Integration with Personalised Therapies
Liquid biopsy is poised to play a central role in personalised oncology. Serial sampling allows real-time adjustment of therapy based on evolving tumour profiles. In the future, this could support adaptive trial designs where therapies are modified dynamically according to liquid biopsy readouts.[135] Integration with personalised cancer vaccines and cell therapies is also anticipated. For example, neoantigens identified from ctDNA could guide vaccine design, while CTC phenotyping could inform CAR-T cell target selection.[136]
6.7 Global Implementation and Health Equity
For liquid biopsy to fulfil its promise globally, implementation strategies must address disparities in access. Simplified, low-cost assays are essential for resource-constrained environments. Partnerships between governments, academia, and industry will be required to ensure equitable distribution.[137] Capacity-building in bioinformatics, laboratory infrastructure, and clinician training is equally important. Without deliberate equity-focused strategies, the technology risks exacerbating existing healthcare inequalities.
6.8 Regulatory Evolution and Standardisation
As technologies evolve, so too must regulatory frameworks. The future will likely see harmonised international standards for assay validation, reporting, and clinical utility assessment. Adaptive regulatory pathways — similar to those employed during the COVID-19 pandemic for diagnostics — may accelerate clinical translation while maintaining safety.[138]
6.9 Vision of the Next Decade
Looking ahead, the ideal cancer diagnostic pathway may begin with a simple blood test performed annually during routine health checks. Results would be integrated with AI-driven risk stratification models to guide follow-up imaging or preventive interventions. Cancer detection would thus become proactive rather than reactive, shifting the paradigm of oncology towards prevention and interception.
7. ETHICAL AND HUMAN CONSIDERATIONS
While technological advances dominate the liquid biopsy discourse, the ethical and human dimensions are equally critical. As with all innovations in oncology, implementation must prioritise patient welfare, autonomy, and justice. Liquid biopsy brings unique ethical challenges due to its non-invasive nature, potential for widespread screening, and generation of vast genomic datasets. This section explores the key human considerations shaping its responsible integration into clinical practice.
7.1 Patient Burden and Experience
A primary advantage of liquid biopsy is the reduction of physical and psychological burden compared with tissue biopsy. Traditional biopsies often require invasive procedures — such as needle aspirations or surgical resections — associated with pain, infection risk, and recovery time.[139] For patients with advanced disease, repeated biopsies can be particularly distressing. Liquid biopsy, by contrast, requires only a blood draw or other non-invasive sample, significantly improving patient comfort and willingness to undergo repeat testing.[140] Serial sampling allows clinicians to track disease progression without subjecting patients to repeated invasive procedures. This shift enhances quality of life, particularly for those with limited treatment options.
7.2 Risk of Overdiagnosis and Overtreatment
The increasing sensitivity of liquid biopsy raises concerns about overdiagnosis. Detecting indolent tumours that may never progress clinically could lead to unnecessary interventions, anxiety, and healthcare costs.[141] Population-wide screening trials highlight this dilemma. While early detection improves outcomes for aggressive cancers, indiscriminate screening risks identifying biologically insignificant lesions. Balancing sensitivity with clinical relevance will be essential to avoid repeating the controversies seen with prostate-specific antigen (PSA) testing in prostate cancer.[142]
7.3 Incidental and Uncertain Findings
Liquid biopsy frequently generates incidental findings, such as CHIP mutations or variants of uncertain significance (VUS). Communicating these results to patients poses ethical challenges. Disclosure of uncertain information can create psychological distress without clear clinical benefit. [143] Consensus is needed on reporting standards: which findings should be disclosed, under what circumstances, and how uncertainty should be explained. Genetic counselling will likely become an integral part of liquid biopsy workflows, helping patients contextualise results. [144]
7.4 Genomic Privacy and Data Security
Liquid biopsy produces extensive genomic data, including germline information, which may have implications for family members. Ensuring confidentiality and secure data storage is paramount. Risks include unauthorised access, misuse by insurers or employers, and potential stigmatisation. [145] Clear legal frameworks are required to govern consent, data ownership, and secondary use. Policies such as the General Data Protection Regulation (GDPR) in Europe provide some safeguards, but global harmonisation is lacking. [146] Patients must be informed of potential risks, and robust cybersecurity measures must be implemented.
7.5 Equity of Access
Access to liquid biopsy remains uneven, both within and between countries. High costs and infrastructure requirements mean that many patients in low- and middle-income countries cannot benefit from these technologies. [147] Even within high-income settings, disparities exist based on socioeconomic status, race, and geography. Ethically, innovations should not widen health inequalities. Policies must ensure equitable distribution, perhaps through subsidies, tiered pricing, or public–private partnerships. [148] Developing affordable, point-of-care assays could further extend access to underserved populations.
7.6 Informed Consent in Screening and Research
In the context of population screening, informed consent is particularly complex. Participants must understand not only the benefits of early detection but also the risks of false positives, false negatives, and overdiagnosis. [149] In research settings, consent must cover the scope of genomic analysis, potential for incidental findings, and future data use. Dynamic consent models, where patients can update their preferences over time, may improve autonomy and trust.[150]
7.7 Patient Autonomy and Shared Decision-making
Liquid biopsy results must be incorporated into shared decision-making frameworks. Patients should be active participants in interpreting results and making choices about surveillance or treatment adjustments. Over-reliance on molecular data without patient input risks undermining autonomy. [151] Clinicians will require training in risk communication, particularly when dealing with uncertain or probabilistic results. Transparent dialogue fosters trust and aligns care with patient values.
7.8 Societal and Ethical Implications
Beyond individual patients, liquid biopsy raises broader societal questions. Widespread use in population screening could reshape cancer epidemiology, shifting the focus from treatment to prevention. While this has potential public health benefits, it also raises concerns about resource allocation and prioritisation of healthcare spending. [152]
Furthermore, the commodification of liquid biopsy data by private companies poses ethical questions around profit, transparency, and patient rights. Balancing innovation with public accountability will be essential.
8. CONCLUSION
Liquid biopsy represents a paradigm shift in oncology. From a simple blood draw or other bodily fluid, clinicians can now access real-time molecular insights into tumour biology, enabling earlier detection, personalised therapy, and dynamic monitoring. Over the past two decades, advances in ctDNA, CTC, and exosome detection technologies have established proof of principle and demonstrated clinical utility across multiple cancer types. Today, liquid biopsy is no longer a speculative tool but an increasingly routine component of precision oncology.
Nevertheless, challenges remain. Sensitivity is limited in early-stage disease, and distinguishing tumour-derived mutations from clonal haematopoiesis requires careful interpretation. Standardisation across laboratories and harmonisation of regulatory frameworks are urgently needed. Costs remain prohibitive in many health systems, and equitable access is far from universal. Beyond technical barriers, ethical considerations — including overdiagnosis, incidental findings, and genomic privacy — must be addressed transparently.
The future of liquid biopsy lies in multi-omic integration, artificial intelligence, and expansion of biomarker repertoires. Combining genetic, epigenetic, transcriptomic, proteomic, and metabolic signals will yield unprecedented resolution of tumour biology. Portable and point-of-care platforms promise to democratise access, bringing cutting-edge diagnostics to resource-limited settings. At the same time, global initiatives are building the evidence base through large prospective trials, such as the Galleri and PanSeer studies, which aim to validate liquid biopsy as a population-wide screening tool.
Most importantly, liquid biopsy has the potential to shift oncology from a reactive to a proactive discipline. Instead of waiting for symptoms or radiographic changes, clinicians may soon intervene at the earliest molecular signs of malignancy. Surveillance of minimal residual disease, prediction of therapeutic resistance, and early interception of cancer precursors exemplify this transformative potential.
As the field matures, success will depend not only on technical innovation but also on responsible clinical integration. Ensuring equity, patient-centred communication, and robust ethical safeguards will be essential. With these foundations, liquid biopsy could become a cornerstone of 21st-century cancer care — a tool that not only improves outcomes but also redefines how society approaches cancer detection, treatment, and prevention.
REFERENCES

Vaidehi Pathak, Liquid Biopsy for Cancer Detection: Biology, Clinical Applications, and Future Horizons, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 838-862. https://doi.org/10.5281/zenodo.18200004
 10.5281/zenodo.18200004
10.5281/zenodo.18200004