Global Group of Institution, Kahanpur khuhi, Anandpur Sahib, Punjab, India, 140117
Migraine is a complex neurological disorder, often influenced by genetics, that causes recurring moderate to severe headaches, frequently accompanied by nausea, and sensitivity to light and sound. The word "migraine" comes from the Greek term "hemikrania." Migraines are common and pose significant personal and public health challenges, characterized by repeated headaches along with neurological and gastrointestinal symptoms. Treatment approaches have advanced over time, with improvements in both immediate and preventative care. Historically, treatments included triptans, NSAIDs, and preventative medications initially developed for other conditions. Migraines are a major cause of disability and absenteeism from work, with migraine without aura being the most prevalent form. Migraine classified into subtypes, such as migraine without aura, migraine with aura, and chronic migraine.
Migraine is a complex neurological disorder, often inherited, characterized by recurring episodes of moderate to severe headaches, typically on one side of the head. These headaches are frequently accompanied by nausea and increased sensitivity to light and sound. The term "migraine" comes from the Greek word "hemikrania," which evolved into "hemigranea" in Latin and "migraine" in French. [1] Migraines are a common neurological issue that affects a large portion of the global population, leading to significant personal and societal difficulties. They are characterized by recurring headaches, ranging from moderate to severe, often accompanied by neurological and gastrointestinal symptoms. Medical treatments for migraines have advanced over time. [2] The approach to treating migraines with medication has evolved, incorporating both immediate and preventative strategies. Immediate treatments focus on relieving migraine symptoms, while preventative treatments aim to reduce the frequency and severity of migraines. Until recently, common medications for managing migraines included triptans, nonsteroidal anti-inflammatory drugs (NSAIDs), and oral preventatives initially developed for conditions like hypertension, depression, and epilepsy. [3] Migraines significantly contribute to disability and absenteeism from work. These episodes involve complex neurological processes, lasting from hours to days, which substantially affect daily life and overall well-being. Migraines without aura are the most prevalent, accounting for 75% of all migraine cases. [4]
Phase of Migraine
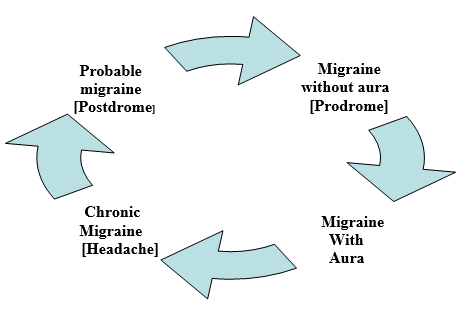
1. Prodrome:
The prodrome phase involves preliminary indicators related to the activation of the hypothalamus by dopamine. Approximately 77% of patients experience these prodromal symptoms, which can last from 24 to 48 hours, before the onset of a headache. This phase is more prevalent in females (81%) compared to males (64%). [5]
Common symptoms:
2. Aura:
In about 25% of cases, alterations happen in cortical function, blood flow, and how the nervous system and blood vessels work together. Auras might come before a headache or at the same time as it. Auras are short, typically under 60 minutes, and mainly visual, involving both positive and negative symptoms.
Symptoms:
Headache is generally unilateral and is associated with symptoms like:
4. Postdrome:
Genetic
Research indicates that genetics significantly influences a person's likelihood of experiencing migraines. Studies involving twins suggest that a single gene variation can cause monogenic migraine disorders. [9]
Genes associated with familial hemiplegic migraine (FHM):
Familial hemiplegic migraine (FHM) is linked to specific genes and affects roughly 0.01% of Europeans, encompassing both sporadic and familial instances. Typically inherited in a varied autosomal dominant pattern, FHM is often traced to a single gene. Genetic studies have pinpointed ATP1A2, CACNA1A, and SCN1A as the primary genes responsible for this condition. [10]
Table 1. Monogenic neurological disorders associated with migraine and their causal genes and mutations
|
Disorder |
Causal gene |
Mechanism of mutation |
|
Familial hemiplegic migraine [FHG] |
CACNA1A ATP1A2
SCN1A |
Missense mutation, gain of function. Missense mutation, partial to complete loss of functionality. Rare and highly complex mutation; mechanism unclear. |
|
Mendelian migraine with aura |
KCNK18 |
A frame shift mutation in the TRESK potassium channel |
|
Episodic ataxia type 2 |
CACNA1A |
Loss-of-function mutation results in decreased channel function and thereby a decrease in intracellular Ca2+ |
|
Spinocerebellar ataxia type 6 |
CACNA1A |
Expansion of ‘CAG’ polyglutamine repeats in the tail of the CACNA1A protein |
The first familial hemiplegic migraine (FHM) gene identified was CACNA1A, located on chromosome 19p13. It was discovered through positional cloning and mutation analysis, which revealed four missense mutations in its conserved regions. [12] This gene typically codes for the pore-forming α1 subunit of the neuronal voltage-gated Cav2.1 channel. A study indicated that deletions in the CACNA1A gene are associated with varying migraine phenotypes. Over 25 pathogenic variants have been found in FHM patients, inherited in an autosomal dominant manner. [13] Additionally, missense mutations tend to cluster near functional domains related to calcium channels, with the condition's severity depending on the variant type. Genetic modifier research using animal models, such as a Drosophila phospholipase C-beta knockdown model, showed that FHM mutations partially alleviate receptors linked to intracellular calcium stores. [14] Genes involved in the Notch and transforming growth factor-β signaling pathways have also been identified as modifiers of CACNA1A. [15] Studies in transgenic mice suggest that female sex hormones influence migraine disorders, potentially explaining their higher prevalence in females. [16] Heterozygous mutations in the CACNA1A gene are linked to spinocerebellar ataxia type 6 and episodic ataxia type 2, which share clinical features. [17] The ATP1A3 gene, encoding the Na+/K+-ATPase ion transport pump, is another cause of familial hemiplegic migraine (FHM). This pump maintains electrochemical gradients in heart, skeletal muscle, and central nervous system cells. Mutations in this gene exhibit autosomal dominant inheritance and cause various symptoms, including epilepsy, seizures, coma, fever, and mental retardation [18] A third FHM-related mutation occurs in the SCN1A gene, located on chromosome 2q24.3. This gene encodes the Nav1.1 protein, a voltage-gated sodium channel crucial for the permeability of excitable membranes in the central nervous system. [19]
Monogenic inheritance conditions associated with migraine:
Muscle and nerve tissue damage can trigger a series of events leading to migraine-like pain. This syndrome is linked to a specific genetic mutation, 3243A>G, in the mitochondrial transfer RNA. [20]] CADASIL, or cerebral autosomal-dominant arteriopathy with subcortical infarcts and leukoencephalopathy, affects small blood vessels in the brain. It causes brain damage leading to cognitive issues and is inherited through a dominant gene, NOTCH3. [21] Retinal vasculopathy with cerebral leukoencephalopathy (RVCL) is a neurovascular condition impacting multiple body systems, causing symptoms like muscle weakness, speech difficulties, stroke, and sometimes epilepsy and migraines. It can also affect the kidneys and liver and is inherited through a single gene, TREX1. [22-23] HIHRATL, or hereditary infantile hemiparesis, retinal arteriolar tortuosity, and leukoencephalopathy, is another small vessel disease related to stroke and migraines. It is passed down through a mutation in the COL4A1 gene on chromosome 13. [24]]
EPIDIMOLOGY
Headaches are a widespread health issue, affecting approximately 12% of the global population, with annual rates reaching up to 17% in women and 6% in men. They are more prevalent in young girls than boys, increase during adolescence, peak between the ages of 35 and 39, and tend to decrease later in life, particularly after menopause. Geographically, headaches are most common in North America, followed by South America, Central America, Europe, Asia, and Africa. Globally, headaches are recognized as the second leading cause of disability. [25- 26]
PATHOPHYSIOLOGY
The pathophysiology of headaches, a condition recognized for approximately 600 years, has evolved in its understanding. While the concept of chronic migraine emerged in the 17th century, initial explanations primarily focused on neurological or vascular mechanisms. More recently, the metabolic aspects of migraines have also been acknowledged. [27] Neuropeptides, including serotonin, calcitonin gene-related peptide (CGRP), and pituitary adenylate cyclase-activating polypeptide (PACAP), are thought to contribute to the development of migraines and role [28]
Serotonin, released from the brainstem, is believed to play a role in migraine, although its exact mechanisms are still under investigation. It's suggested that reduced serotonin levels between migraine episodes may impair the pain inhibition system, potentially triggering trigeminal system activation and worsening migraine symptoms. Serotonin's effects may involve direct influence on cranial vessels, pain pathways, or brainstem projections. [29-30] CGRP, found in trigeminal ganglion neurons, is released from nerve terminals and secreted within the ganglion. Upon release, CGRP boosts nitric oxide production, sensitizing trigeminal nerves. It also acts as a potent vasodilator in cerebral and dural vessels, contributing to neurogenic inflammation and pain transmission to the central nervous system. [31] PACAP may also be important in migraine, with increased levels during attacks, and its infusion can induce migraines in susceptible individuals.
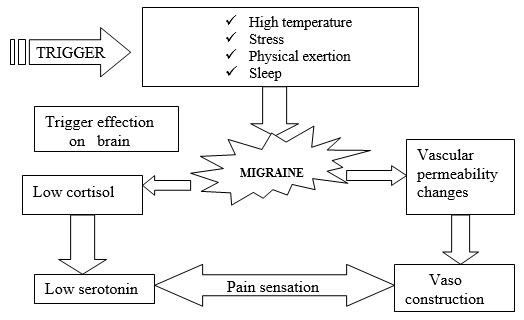
Fig.2: Pathophysiology of Migraine [32]
DIAGNOSIS
Diagnostic criteria differ for migraine with aura (MA) and migraine without aura (MO). MA is characterized by at least five headaches lasting 4–72 hours, and features such as a pulsating sensation, pain on one side of the head, intense pain, or worsening of pain during routine activities. [33]
To correctly diagnose a headache, it's essential to understand how it started. Headaches can manifest in two primary ways: as a worsening of existing headache conditions, marked by more frequent episodes that don't resolve, or as a sudden, unremitting headache. The former is termed a transformed migraine, while the latter is known as a new daily persistent headache. Recognizing these patterns is crucial because they indicate the underlying cause of the headache. Identifying the correct type of headache is vital for both accurate diagnosis and effective treatment. [34]
Recognition of the migraine phases
To correctly diagnose a headache, it's essential to understand how it started. Headaches can manifest in two primary ways: as a worsening of existing headache conditions, marked by more frequent episodes that don't resolve, or as a sudden, unremitting headache. The former is termed a transformed migraine, while the latter is known as a new daily persistent headache. Recognizing these patterns is crucial because they indicate the underlying cause of the headache. Identifying the correct type of headache is vital for both accurate diagnosis and effective treatment. [35]
To diagnose a condition accurately, a thorough medical history is essential, allowing patients’ ample time to detail their experiences. Physical examinations, including inspection, funduscopy, and palpation of the neck and head, alongside neurological and cardiovascular screenings, help identify factors worsening the condition. Screening questions should focus on the pain's pattern, onset, type (episodic or continuous), duration, and potential triggers. Detailed recording of pain characteristics and associated symptoms, like yawning, fatigue, or sensory disturbances, is crucial, as are symptoms such as conjunctival injection or rash, which may indicate primary or secondary headaches. Documenting prior and current treatments, including medication dosages, is also vital for a comprehensive understanding of the patient's condition. [36]
Migraines are typically diagnosed based on a patient's medical history without the need for specific tests. However, imaging and blood work may be used to rule out other potential causes of headaches. While a physical exam can reveal neurological issues, CT scans and MRIs can provide further confirmation of a diagnosis. [37]
To rule out other causes of headaches, doctors use clinical examinations along with CT and MRI scans. CT scans of migraine patients have revealed abnormalities in some cases. For instance, a study of 94 people with migraines showed that 2 had glioma, 6 had cerebral infarcts, and 6 had periventricular edema. Another study of 53 migraine patients showed that 25 had focal atrophy, generalized atrophy, and other abnormalities. Additionally, one out of 453 migraine patients had a choroid plexus papilloma. Hospitalized patients have shown ventricular enlargement and low-density areas. Other conditions, like acute infarction, subarachnoid hemorrhage, metastatic neoplasm, primary neoplasm, hydrocephalus, and subdural hematoma, have also been found in some studies. Focal atrophy is more common in older people, and abnormalities such as ischemia, atrophy, calcifications in the basal ganglia, and ventricular enlargement are frequently seen, with atrophy often indicating aging. [38-42]
MRI neuroimaging studies have shown that white matter lesions are linked to the clinical characteristics and demographics of individuals with migraines. People with heart disease, hypertension, or diabetes are more likely to have white matter abnormalities. Patients with migraine with aura (MA) have significantly more white matter lesions compared to those with migraine without aura (MO). [43] Additional findings include heterotopia and atrophy in the frontoparietal and cortical regions. Patients with headaches exhibit more intracranial abnormalities than those without headaches. White matter lesions are also observed in some younger individuals with migraines. Furthermore, studies have identified cortical abnormalities, petrous apex cholesterol cysts, and meningiomas in certain migraine patients. MRI studies have also revealed pituitary abnormalities and white matter hyperintensities (WMH) [44]
CT and MRI scans are both used in the assessment of the neurological condition of patients who suffer from migraines. A study by Wang et al. found abnormalities in MRI scans of 4 out of 688 migraine patients, but CT scans of the same patients showed no significant abnormalities. [45] These abnormalities included tumors in the nose and throat, as well as hydrocephalus. CT and MRI scans of individuals with late-onset migraines (after age 40) revealed cerebral infarction and carotid atheroma in a small number of participants, while 93% of the subjects showed normal neuroimaging results. [46] In a study comparing MRI and CT scans across 74 subjects, multiple foci were observed on T2-weighted MRI, but not on CT scans. Another study found that 26 subjects exhibited generalized ventricular or focal enlargement on both CT and MRI neuroimaging. [47]
Diagnosis of chronic headaches can be challenging due to the lack of a clear pattern. Doctors often rely on initial assumptions to differentiate between primary and secondary headache disorders. Patients usually seek medical attention for severe headaches rather than mild ones caused by stress or tension. Evaluating the history of a patient's headaches can reveal a pattern that has progressed into chronic migraines. These headaches can be triggered by factors such as excessive caffeine or painkiller use, psychological issues like depression or anxiety, or physical conditions like significant life events or sleep. [48]
TREATMENT
The primary goal in treating migraines is to lessen their intensity and duration, while also aiming to restore normal function, minimize the need for immediate relief medications, and promote effective long-term management with minimal side effects. [49] Opioids are not typically recommended for migraine treatment due to their potential for addiction and their ability to reduce the effectiveness of triptans, as well as increase sensitivity to medication. Over-the-counter drugs are a primary treatment option for most migraine sufferers. Medications like naproxen, ibuprofen, acetaminophen, and aspirin are commonly used as a first-line approach for migraine attacks. These drugs are favored due to their minimal side effects, ease of administration, affordability, and effectiveness. [50]
DRUGS:
It known as paracetamol, is a non-opioid pain reliever and fever reducer used to treat mild to moderate migraines.
Mechanism of action
While its exact mechanism is not fully understood, it is believed to work by inhibiting cyclooxygenase (COX), which reduces the production of prostaglandins, substances that contribute to inflammation. Acetaminophen specifically targets the COX pathway in the central nervous system.
side effects
It is not recommended for individuals with severe liver disease or hypersensitivity to acetaminophen.
Naproxen, a nonsteroidal anti-inflammatory drug (NSAID), is used to alleviate inflammation, pain, and fever. It is available in sodium salt and free acid forms and is rapidly absorbed in the gastrointestinal tract. Naproxen is often favored as an analgesic, taking effect within one hour and lasting for 8 to 12 hours. Its half-life is 15 hours, longer than that of ibuprofen. [52]
Mechanism of action
It works by inhibiting cyclooxygenase (COX) enzymes, which are responsible for producing prostaglandins and thromboxanes, key mediators of inflammation.
Side effects
Naproxen is a medication used in the initial treatment of migraine headaches. However, it is not suitable for everyone. Individuals who are hypersensitive to nonsteroidal anti-inflammatory drugs (NSAIDs) or aspirin, or who have ulcers, should not use naproxen. [53]
Ibuprofen is a medication used to alleviate pain, reduce fever, and decrease inflammation, and it is often prescribed for migraine headaches. [54]
Mechanism of action
It functions by inhibiting the enzymes COX-1 and COX-2, which are crucial in the production of prostaglandins. After ingestion, it has a half-life of 2 to 4 hours, with its highest concentration in the blood occurring 1 to 2 hours later.
Side effect [55]
Aspirin is a medication used for treating long-term headaches, either by itself or with other medications.
Mechanism of action
It works by preventing the body from producing thromboxane by blocking cyclooxygenase (COX) enzymes. Aspirin is also used as an antiplatelet drug, which can increase the risk of bleeding. It can be taken orally or intravenously.
Acetaminophen, aspirin, and caffeine are combined as a triple therapy for chronic migraine treatment. This combination has an analgesic effect, which has been confirmed in multiple studies. It is indicated for both migraine and tension-type headaches. The combined effect of these drugs is more effective than any single drug alone. [57-58]]
Melatonin, a hormone produced by the pineal gland, regulates the body's circadian rhythm and promotes sleep by acting on hypothalamic receptors. It is used for short-term treatment of insomnia and migraine prevention, with a typical dose of 3 mg for migraine prophylaxis.
Mechanism of action
Melatonin, a hormone produced in the pineal gland, primarily regulates the sleep-wake cycle by interacting with the suprachiasmatic nucleus of the hypothalamus and the retina. It binds to high-affinity receptors, MT1 and MT2, located on the plasma membrane, which are coupled with G proteins. This interaction promotes sleep and inhibits wake-promoting signals. Additionally, melatonin affects the hypothalamus, signaling it to reduce activity which lowers body temperature, blood pressure, and influences mood, preparing the body for sleep. Melatonin also functions as an antioxidant, reducing free radicals and protecting ATP synthesis at the mitochondrial level. [59]
Side effect
It is not recommended for pregnant or breastfeeding women. Patients with migraines that do not respond to initial treatments should be re-evaluated by specialists, who may consider non-pharmacological options like greater occipital nerve blocks, which can reduce pain in about 50% of patients. In rare, challenging cases, neurosurgical methods such as deep brain stimulation or occipital nerve stimulation may be used. [60]
Acute migraine headache: treatment strategies
In treating acute migraine attacks, triptans are considered the most effective first-line therapy, particularly for patients who do not respond to analgesics or NSAIDs. Triptans work by selectively activating serotonin receptors in intracranial blood vessels, causing vasoconstriction and alleviating the dilation associated with migraines. Triptans are selective Serotonin-agonists. Triptan binding to the Serotonin receptors (5-HT1B) in intracranial vessels (which are dilated during a migraine attack), produces vasoconstriction. Triptan binding to the neurogenic and central Serotonin receptors (5-HT1D) inhibits Substance P and CGRP release and blocks pain signals to the brain by inhibiting nociceptors. [61-62]
the first triptan, was released in 1991 and is still considered the standard treatment. It comes in various forms like tablets, nasal sprays, and injections. The injectable form works fastest and is preferred for severe headaches or when patients can't take pills due to nausea. Sumatriptan targets blood vessels in the head, which minimizes cardiovascular side effects. [63]]
Zolmitriptan, a medication used to treat migraines, is formulated as tablets, nasal sprays, and orally disintegrating tablets. The nasal spray form of zolmitriptan is considered safe for use in children who are 12 years of age and older. d safe for use in children who are 12 years of age and older. [64-65]
It is a medication with a 3-hour half-life, is administered orally in tablet form. It has received approval for treating migraine headaches lasting at least 4 hours in adolescents. [66]
They are available as oral tablets and are used to prevent menstrual migraines. Frovatriptan, which has a half-life of 26 hours, is suitable for migraine patients with longer-lasting headaches. It specifically targets the cerebral vascular system with limited vasoconstrictive effects. Naratriptan also has a longer half-life and higher bioavailability compared to sumatriptan. [67]
They medications available as oral tablets, have different half-lives of 4 hours and 2 hours, respectively. Rizatriptan also comes in an orally disintegrating tablet form. Triptans, including these medications, are not recommended for individuals with poorly managed hypertension, hemiplegic or basilar migraines, severe liver or kidney problems, or coronary artery disease. Furthermore, frequent use of triptans (more than 10 days a month) may result in medication-overuse headaches. [68]
GENERAL MANAGEMENT
General migraine management involves addressing lifestyle factors and related health conditions. Identifying and managing triggers like sleep issues and dietary factors (such as cheese, alcohol, chocolate, and excessive caffeine) is crucial. Maintaining a healthy weight and exercising are also recommended. Psychological, behavioral, or physical therapies may benefit patients, depending on their specific triggers. Natural remedies like riboflavin, feverfew, coenzyme Q-10, and magnesium are sometimes used, but their effectiveness varies and are not considered primary treatments. [69-70] Medications can be used to treat acute migraine episodes or reduce their frequency. Updated guidelines provide recommendations on general principles, dosages, and specific instructions for pregnant women and children. The goal of migraine treatment is to alleviate headache pain within 1-2 hours, although treatments may not significantly impact other phases of the migraine. Managing headaches as early as possible is important, and combination therapies, including aspirin, paracetamol, NSAIDs, triptans, and antiemetics, may be necessary in some cases. [71]
Managing nausea is crucial as it can hinder the body's ability to absorb medications. Combining antiemetics with analgesics aids in the overall management and treatment. If a patient cannot take medication orally, alternative administration methods such as ondansetron wafers for vomiting, NSAID suppositories, non-oral triptan formulations, or prochlorperazine suppositories can be considered. [72]
Menstrual migraines are challenging to treat due to their intensity and recurring nature. Oral contraceptives might help reduce the frequency and predict the timing of these migraines in relation to menstruation. However, individuals with migraine with aura (MA) should avoid oral contraceptives due to the increased risk of stroke. Naproxen, along with other acute treatments, can alleviate perimenstrual symptoms. [72]
Studies have explored how exercise affects pain intensity and the duration of attacks. Previous research showed a 20-54% reduction in pain intensity and a 20-27% reduction in the duration of attacks. However, the results regarding pain duration and intensity couldn't be combined due to differences in measurement methods. Exercise also led to a significant 71% decrease in the use of pain medication, although the study wasn't specifically designed to measure this. Other studies found no significant difference in medication use between people on drug treatment and those combining it with exercise. Another study indicated that fewer medications were used by those exercising compared to those maintaining their usual activities, but this result wasn't statistically significant. [73]
CONCLUSION:
Migraine is more than just a headache; it's a complex neurological condition that severely affects a person's life quality and can lead to disability. Although there is currently no cure, managing the condition can significantly lessen the impact of attacks. A comprehensive understanding of migraine, including its genetic roots and mechanisms, is essential for creating better, more targeted treatments.
REFERENCES

Neha, Jasmine Dhiman*, Sanjeev Duggal, Migraine Headache: An Overview, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 3239-3253. https://doi.org/10.5281/zenodo.15464259
 10.5281/zenodo.15464259
10.5281/zenodo.15464259
