
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1237Research Scholar at Department of Pharmaceutics, Dr. Shivajirao Kadam College of Pharmacy, Kasabe - Digraj, Maharashtra, India
4Research Scholar at Department of Pharmaceutics, St.John Institute of Pharmacy and Research, Palghar, Maharashtra, India
5Graduate Student, Womens college of pharmacy, peth vadgaon, Maharashtra, India
6Research Scholar at Department of Pharmaceutics, Maratha Vidya Prasarak Samaj College of Pharmacy Nashik, Maharashtra, India
The vaginal route of drug administration offers significant advantages for both local and systemic therapy due to its large absorptive surface area, rich vascularization, avoidance of first-pass hepatic metabolism, and reduced gastrointestinal degradation. However, conventional vaginal dosage forms such as creams, gels, tablets, and suppositories often exhibit limited therapeutic effectiveness because of rapid mucus turnover, vaginal self-cleansing, pH variability, formulation leakage, and poor patient compliance. To overcome these limitations, mucoadhesive drug delivery systems (MDDS) have emerged as a promising approach to improve vaginal drug delivery outcomes. By establishing prolonged and intimate contact with the vaginal mucosa through physicochemical interactions between polymers and mucin, mucoadhesive systems enhance formulation residence time. This review provides a comprehensive overview of vaginal anatomy and physiology, challenges in vaginal drug delivery, mechanisms of mucoadhesion, and the role of mucoadhesive polymers. Various mucoadhesive dosage forms, evaluation parameters, therapeutic applications, recent advancements, and future clinical and regulatory challenges are also discussed.
Because of its unique anatomical, physiological, and biochemical features, the vaginal route of administration is universally acknowledged as a very beneficial method for both local and systemic drug delivery. The vagina offers a comparatively large surface area for medication absorption because it is a muscular, fibromuscular canal bordered with stratified squamous epithelium. Drugs that are ingested can be quickly transported into the systemic circulation thanks to this epithelium's abundance of blood arteries and lymphatic network.[1] Vaginal drug distribution, as opposed to oral administration, avoids exposure to harsh gastrointestinal conditions that might affect drug stability and bioavailability, such as acidic pH, digestive enzymes, and varying gastric emptying durations. Additionally, medications given vaginally can avoid first-pass hepatic processing, which is a significant contributing cause to the decreased systemic availability of many therapeutic medicines. Therefore, vaginal delivery provides a useful substitute for increasing the bioavailability of medications that are poorly absorbed or heavily metabolized when taken orally.[2]Because of these benefits, the vaginal route is especially well-suited for a variety of therapeutic uses, such as the management of infertility, hormone replacement therapy, gynaecological infections, STDs, contraception, and even the systemic delivery of peptides, proteins, and vaccines.[3] Additionally, vaginal drug delivery is linked to easier administration, fewer doses, and better patient convenience—all of which are critical factors in long-term treatments. Additionally, localized drug administration via the vagina minimizes systemic side effects while enabling high drug concentrations at the site of action a significant benefit in the treatment of inflammatory diseases and vaginal infections.[4]The therapeutic efficacy of vaginal medication delivery is nevertheless limited by the disadvantages of traditional dose forms as creams, gels, foams, pills, pessaries, and suppositories, despite the many benefits provided by the vaginal route.[5] These conventional formulations are less suitable for long-term or prolonged therapy because they are often designed for rapid drug release and brief duration of action. The innate self-clearing characteristic of the vaginal canal is a major physiological barrier to successful vaginal medication administration.[6]Constant vaginal fluid renewal, frequent exfoliation of epithelial cells, and ongoing mucus production are characteristics of this process. Because of this, given formulations are quickly eliminated from the vaginal canal, which reduces the amount of time the medication is in touch with the mucosal surface and, as a result, lowers drug absorption and retention.[7]Conventional vaginal dose forms hence frequently show inadequate retention, uneven drug distribution, and less interaction with the vaginal mucosa, resulting in less than ideal therapeutic effects. Furthermore, patients frequently experience discomfort, difficulty, and social embarrassment due to formulation leaks.[8] In order to maintain therapeutic drug levels, these factors often require repeated administration, which may raise the risk of local irritation, disturb the natural vaginal microbiota, and have a detrimental effect on patient compliance. Therefore, despite the vaginal route's inherent benefits, sophisticated drug delivery methods that can get beyond these physiological obstacles and increase treatment efficacy are still desperately needed.[9]Mucoadhesive drug delivery systems (MDDS) have become a viable and successful method for vaginal drug delivery in order to overcome these obstacles. The ability of a substance to stick to a mucosal surface through interactions with the mucus layer or the epithelial tissue is known as mucoadhesion.[10] Mucoadhesive systems are made to make close, long-lasting contact with the vaginal mucosa in order to prevent clearance mechanisms and prolong the formulation's residence time at the administration site. This extended retention lowers the frequency of dosing, improves therapeutic efficacy, and increases drug absorption.[11]The process of mucoadhesion involves several steps, starting with the polymer's initial wetting and hydration, followed by polymer swelling and the subsequent interpenetration of polymer chains into the mucus layer. Alongside this, a number of intermolecular interactions are established between the polymer and mucin glycoproteins, such as hydrophobic interactions, van der Waals forces, hydrogen bonding, and electrostatic attraction.[12] Mucoadhesive drug delivery systems improve formulations' adhesion to the vaginal mucosa through these coupled mechanisms, which increases drug retention and site-specific localization. As a result, these systems can offer controlled and extended drug release, which makes them especially useful for the treatment of long-term illnesses that need constant therapeutic exposure.[13]Numerous mucoadhesive vaginal formulations have been created to address a range of therapeutic requirements. Mucoadhesive gels, pills, films, suppositories, microspheres, and nanoparticles are some of them. Mucoadhesive gels are the most popular of these since they are simple to apply and spread evenly across the vaginal mucosa. While suppositories give prolonged medication release and localized action, mucoadhesive tablets and films enable accurate dosing and enhanced durability. Particulate systems like microspheres and nanoparticles have drawn a lot of attention lately because of their capacity to improve penetration, offer regulated release, and shield medications from deterioration.[14]In order to achieve adhesion and prolonged medication release, conventional mucoadhesive systems mostly rely on synthetic and natural polymers. Because of their superior swelling behavior and potent mucoadhesive qualities, synthetic polymers like polyacrylates are commonly employed. Conversely, natural polymers provide benefits including limited toxicity, biocompatibility, and biodegradability.[15] New Nano carrier-based systems that combine mucoadhesive qualities with controlled release and mucus-penetrating capabilities have been created because to developments in pharmaceutical technology. These cutting-edge solutions are made to go past the diffusion barrier that vaginal mucus presents while still having enough adhesion to guarantee long-term retention.[16]The effectiveness of vaginal MDDS is significantly influenced by the choice of suitable mucoadhesive polymers. Poly(acrylates) like Carbopol, chitosan, cellulose derivatives (such hydroxypropyl methylcellulose and carboxymethyl cellulose), alginates, hyaluronic acid derivatives, and other natural polysaccharides are often used polymers. Each of these polymers has unique physicochemical characteristics that affect their drug release qualities, mechanical strength, swelling capacity, and mucoadhesive behavior.[17]Because polyacrylates contain carboxylic groups that can establish hydrogen bonds with mucin, they are recognized for having a high mucoadhesive strength. Strong electrostatic interactions between negatively charged mucus and chitosan, a cationic polymer, make it very useful for mucoadhesive applications. While alginates and hyaluronic acid derivatives offer biocompatibility and hydration that are advantageous for vaginal applications, cellulose derivatives offer superior film-forming qualities and regulated drug release. To achieve the intended balance between adhesion, medication release, mechanical stability, and patient comfort, the choice of polymer or polymer combination must be carefully optimized.[18] The dynamic biological milieu of the vagina has a considerable impact on the effectiveness of mucoadhesive medication delivery devices in addition to polymer selection. Changes in pH, enzymatic activity, mucus composition, and hormonal swings related to menstruation, pregnancy, and menopause define the vaginal environment.[19] Polymer swelling, drug stability, and release behavior can all be impacted by vaginal pH, which normally ranges from acidic to neutral depending on physiological circumstances. Vaginal secretions contain enzymes that can break down specific medications or polymers, and mucus turnover can affect how long mucoadhesion lasts.[20]Hormonal fluctuations can also affect the effectiveness of drug delivery by changing vaginal fluid volume, mucus viscosity, and epithelium thickness. Effective MDDS formulations must therefore be thoughtfully created to endure these physiological difficulties while preserving a robust and reliable adherence to the mucosal surface.[21] To increase the robustness and dependability of vaginal MDDS, advanced formulation techniques as pH-responsive systems, enzyme-resistant polymers, and thermosensitive gels are being investigated.[22]All things considered, vaginal mucoadhesive drug delivery systems offer a viable and adaptable platform for improving the management of numerous local and systemic disorders. These systems provide substantial advantages over traditional vaginal formulations by extending residence time, enhancing drug retention, and permitting controlled release. They have shown great promise in the treatment of vaginal infections, hormone administration, contraception, and new uses like microbicide delivery and vaginal immunization.[23]
2. Anatomy and Physiology of the Vaginal Mucosa
The human vagina is a dynamic, intricate organ used for both medicinal and reproductive purposes. Anatomically, it is a fibromuscular tubular canal that runs from the uterine cervix to the external genitalia (vestibule). Its length is around 7–10 cm, and its breadth and thickness vary according to age, hormonal status, and physiological phase. The surrounding fascia and pelvic muscles support the vaginal tube, which is positioned at a 90° angle to the uterus. This allows for flexibility and distension during sexual activity and birthing. The anterior, posterior, and lateral fornices surrounding the cervix are among the anatomical divisions of the vaginal canal, and the walls exhibit transverse folds known as rugae that increase surface area and permit expansion.[24]
2.1 Histological Structure
Three primary layers make up the vaginal wall histologically: the adventitia (outside connective tissue layer), the muscularis (middle smooth muscle layer), and the mucosa (inner layer). The non-keratinized stratified squamous epithelium that makes up the mucosa lacks glands; instead, cervical mucus, vaginal transudate, and exfoliated epithelial cells provide lubrication.[25] The lamina propria, a vascular, collagen-rich layer of connective tissue that supports immune surveillance and cellular turnover, is located underneath the epithelium. While the adventitia comprises collagen and elastin fibres that provide elasticity and resilience, the muscular layer is made up of smooth muscle fibres scattered with elastic tissue to provide structural integrity and contractility.[26]
2.2 Vaginal Mucosa Function and Barrier Properties
Both absorption and defence depend on the vaginal mucosa. Pathogens and mechanical injury are physically prevented by the squamous epithelium and the mucous layer that covers it. Mucus from cervical secretions and transudate produces a viscoelastic covering over the epithelium, even though other mucosal tissues lack goblet cells that make mucus. This mucus, which forms a protective gel and affects medication transport and retention, is made up of water, mucin glycoproteins, enzymes, immunological proteins, and exfoliated cells.[27]The vaginal environment is maintained by a complex interaction between hormonal and microbial variables. Oestrogen promotes cellular glycogen storage and epithelial growth in women of reproductive age. After being exfoliated and broken down, glycogen acts as a nutritional substrate for Lactobacillus species, which ferment the breakdown products of glycogen into lactic acid, keeping the pH between 3.5 and 4.5. Many diseases find this acidic environment to be unfriendly, offering a natural defence. Epithelial thickness, mucus composition, and pH are all dramatically altered by changes in oestrogen levels, which can occur throughout the menstrual cycle, pregnancy, or menopause. These changes have an impact on barrier function and permeability.[28]
2.3 Physiological Variability and Implications for Drug Delivery
The vaginal mucosa's physiological properties differ significantly between biological situations and life stages. For instance, throughout the menstrual cycle, progesterone dominance following ovulation results in distinct mucosal characteristics, whereas oestrogen peaks close to ovulation cause increased epithelial thickness and alterations in mucus consistency. Reduced oestrogen levels during menopause lead to epithelium thinning, decreased mucus production, elevated pH, and an increased risk of infection and dryness. Drug absorption, mucoadhesion, and formulation performance are all directly impacted by these variables.[29] The lamina propria contains a vast network of capillaries that provide good vascularization to the vaginal mucosa. This abundant blood supply promotes both systemic drug absorption and local therapeutic benefits. The vagina is an appealing route for both local and systemic therapy since pharmacokinetic studies have shown that numerous lipophilic and low-molecular-weight drugs can effectively pass through the vaginal epithelium and into the systemic circulation.[30]
2.4 Protective Immune Functions
The vaginal mucosa supports mucosal immunity in addition to its barrier and absorptive functions. It has immune cells that identify and react to microbial threats, including lymphocytes, dendritic cells, and macrophages.[31] Additionally, the mucosal surface secretes antimicrobial peptides and displays pattern recognition receptors that are involved in preserving homeostasis and protecting against infections such as bacterial vaginosis and vulvovaginal candidiasis. By generating hydrogen peroxide and other inhibitory compounds against pathogenic organisms, Lactobacillus species, which are major members of the vaginal microbiota, further strengthen immune protection.[32]
2.5 Relevance to Drug Delivery Systems
The structure and physiology of the vaginal mucosa offer both opportunities and obstacles for medication delivery. While the mucus layer and pH can affect formulation residence duration and drug release profiles, its enormous surface area, permeability, and circulatory network facilitate effective medication absorption. For instance, the viscoelastic gel structure of mucus acts as both a barrier to medication diffusion and a target for mucoadhesive formulations intended to increase absorption and prolong contact duration. To guarantee constant function, formulation design must also take into account dynamic variations in mucus qualities throughout the menstrual cycle.[33]
3. Challenges in Vaginal Drug Delivery
The intricate anatomy and physiology of the vaginal route provide serious obstacles to efficient and reliable treatment results, despite the route's potential benefits for both local and systemic medication delivery. The protective and dynamic vaginal milieu is a significant barrier to vaginal medication administration. The first line of defence against viruses, foreign objects, and irritants is the viscoelastic mucus layer lining the vaginal cavity. Although this layer of mucus aids in the maintenance of vaginal health, it also functions as a chemical and physical barrier that may hinder the diffusion and retention of drugs. Conventional formulations, including gels and suppositories, are quickly cleared by the constant secretion and turnover of mucus, which shortens their residence time and decreases their bioavailability at the target region.[34]Additionally, because Lactobacillus species create lactic acid, the pH of the vaginal environment is normally acidic (between 3.5 and 4.5) in healthy women. Although this acidic environment protects against infections, it can affect the stability and solubility of medications, particularly those that are sensitive to pH. Formulation design is further complicated by pH variations linked to ageing, menstruation, infection, or hormonal changes.[35]Variations in vaginal mucous and epithelial thickness across various physiological conditions present another difficulty. Mucus viscosity, volume, and epithelial cell turnover are all greatly impacted by hormonal changes throughout the menstrual cycle or menopause, which also have an impact on drug absorption and distribution. Additionally, through adhesion and steric interactions, the mucus layer can retain particle delivery systems, causing quick clearance before enough drug release can take place.[36]Complicating matters further are the immune system and vaginal bacteria. Drug disposition and therapeutic efficacy can be altered by microbial composition disruptions, such as those caused by bacterial vaginosis or candidiasis, which can change mucus characteristics, pH, and enzyme activity. All things considered, these physiological obstacles-such as mucus clearance, pH fluctuations, epithelium alterations, and microbiota dynamics-represent significant obstacles to successful and long-lasting vaginal medication administration. To improve retention and absorption, novel formulation techniques such mucoadhesive and mucus-penetrating delivery methods are needed to address these problems.[37]
Table No 1: Challenges in Vaginal Drug Delivery
|
Challenge |
Physiological Basis |
Effect on Formulation Performance |
Impact on Drug Bioavailability & Efficacy |
Formulation Strategies to Overcome |
References |
|
Viscoelastic mucus barrier |
Vaginal mucus composed of mucins, water, enzymes, and lipids forming a protective gel layer |
Limits diffusion of drug molecules and particulate carriers |
Reduced penetration and uneven drug distribution |
Mucoadhesive polymers, mucus-penetrating nanoparticles |
38 |
|
Rapid mucus turnover (self-cleansing) |
Continuous secretion and renewal of vaginal mucus and fluids |
Quick removal of gels, creams, and suppositories |
Short residence time; frequent dosing required |
Mucoadhesive gels, films, tablets, in situ gelling systems |
39 |
|
Epithelial cell exfoliation |
Constant shedding of superficial epithelial cells |
Loss of drug–epithelium contact |
Decreased absorption and retention |
Bioadhesive systems with prolonged adhesion |
40 |
|
Acidic vaginal pH (3.5–4.5) |
Lactic acid production by Lactobacillus species |
Drug instability or precipitation of pH-sensitive drugs |
Reduced solubility and therapeutic activity |
pH-buffered systems, polymer-based carriers |
41 |
|
pH variability |
Changes during menstruation, menopause, infections, pregnancy |
Unpredictable drug release behavior |
Variable therapeutic response |
pH-responsive polymers, adaptable formulations |
42 |
|
Hormonal fluctuations |
Estrogen/progesterone changes alter mucus thickness and viscosity |
Inconsistent formulation performance |
Variable absorption across patient populations |
Personalized or hormone-responsive delivery systems |
43 |
|
Mucus entrapment of particles |
Adhesive and steric interactions between mucus and particles |
Nanoparticles cleared before drug release |
Low bioavailability of particulate systems |
Surface-modified mucus-penetrating nanoparticles |
44 |
|
Microbiota alterations |
Conditions like bacterial vaginosis or candidiasis alter flora |
Changes in pH, enzymes, mucus composition |
Altered drug metabolism and efficacy |
Microbiota-compatible excipients |
45 |
|
Enzymatic activity |
Presence of proteases and esterases in vaginal fluid |
Drug degradation |
Reduced drug stability |
Enzyme-resistant formulations, encapsulation |
46 |
|
Patient discomfort & leakage |
Fluid nature of conventional dosage forms |
Poor retention and acceptability |
Reduced compliance |
Films, tablets, bioadhesive gels |
47 |
4. Mucoadhesion: mechanisms & theories.
The ability of a substance (often a polymer) to stick to a mucosal surface is known as mucoadhesion. This property increases a formulation's residence duration at the site of delivery, boosting medication absorption and therapeutic efficacy. In pharmaceutical sciences, this phenomenon has been thoroughly investigated as a way to get beyond the conventional dose forms' quick clearance and low retention on mucosal tissues such the oral, nasal, and vaginal mucosa.[48]The contact (or soaking) stage and the consolidation stage are the two broad stages of the mucoadhesion process. Mucoadhesive polymers spread out and make first contact with the mucosal surface during the contact stage, which is frequently made possible by the polymer's swelling and hydration. Interfacial contacts between the polymer and the mucus layer intensify during the consolidation stage, creating adhesive connections that maintain attachment in physiological settings.[49]
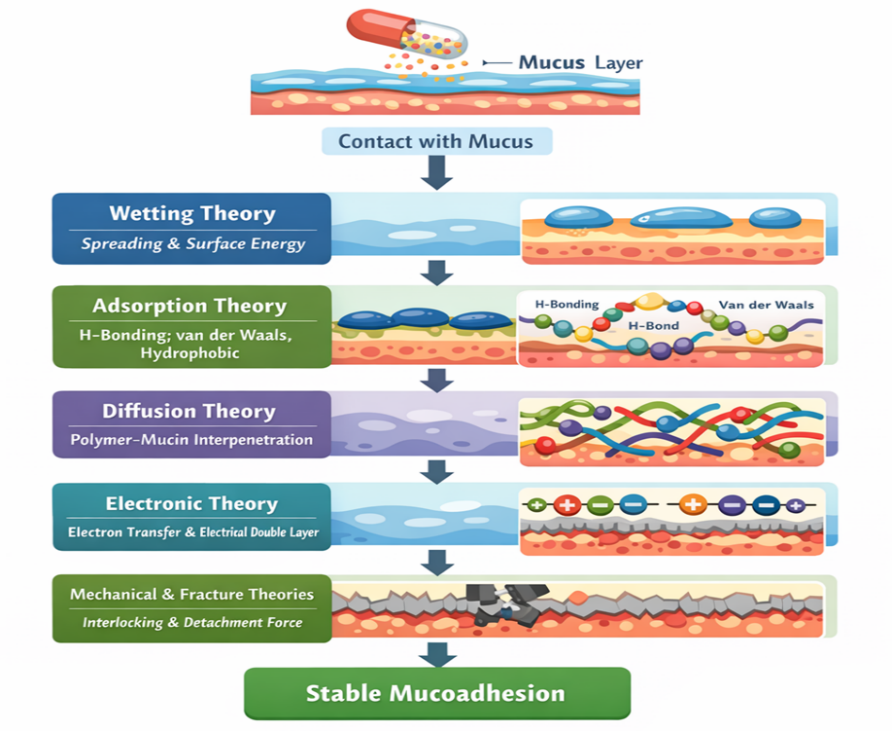
Fig No 1: Theories of Mucoadhesion
4.1 Wetting Theory:This theory highlights the significance of surface energy and spreading in liquid or low-viscosity mucoadhesive systems. Contact area and adhesion strength are increased when a polymer is more wettable on the mucosal surface.[50]
4.2 Adsorption Theory: Secondary chemical interactions between the mucoadhesive polymer and mucin glycoproteins, including hydrogen bonding, van der Waals forces, and hydrophobic interactions, cause adhesion.[51]
4.3Diffusion idea: According to this idea, adhesion is stabilized by a physical entanglement network formed when polymer and mucin chains interpenetrate. The molecular weight and flexibility of the polymer determine the degree of interpenetration.[52]
4.4 Electronic Theory: An electrical double layer and attractive forces form at the contact as a result of electron transfer between the polymer and mucus, which causes adhesion.[53]
4.5 Mechanical and Fracture Theories: Additional insights into mucoadhesion strength and detachment behavior are provided by mechanical interlocking between polymer and mucosal surface imperfections and the force necessary to break adhesive connections.[54]
5. Mucoadhesive Polymers
Mucoadhesive polymers are essential to mucoadhesive drug delivery systems because they create and sustain close contact between the mucosal surface and the formulation. Through hydrogen bonding, electrostatic attraction, van der Waals forces, and polymer chain interpenetration, these polymers interact with mucus, extending residence time and improving drug absorption. Mucoadhesive polymers can be generically categorised into three types based on their origin and chemical modification: natural, semi-synthetic, and synthetic.[55]
5.1 Natural Polymers
The biocompatibility, biodegradability, and low toxicity of natural polymers make them popular. Pectin, gelatin, xanthan gum, guar gum, chitosan, and alginates are typical examples. Because of its electrostatic interactions with negatively charged mucin, chitosan, a cationic polysaccharide produced from chitin, demonstrates high mucoadhesive characteristics. When hydrated, alginates and pectin create hydrogels that offer prolonged drug release without compromising mucosal compatibility.[56]
5.2 Semi-Synthetic Polymers
Chemically altered natural polymers with enhanced mechanical strength and regulated swelling behaviour are known as semi-synthetic polymers. Vaginal mucoadhesive formulations frequently use cellulose derivatives as hydroxypropyl methylcellulose (HPMC), carboxymethyl cellulose (CMC), and hydroxyethyl cellulose (HEC). These polymers are suitable for tablets, films, and gels because of their good film-forming ability, moderate mucoadhesion, and consistent drug release profiles.[57]
5.3 Synthetic Polymers
Strong and consistent mucoadhesive qualities are provided by synthetic polymers because of their distinct chemical structures. Among the most widely utilized synthetic mucoadhesive polymers are poly(acrylic acid) derivatives as Carbopol and polycarbophil. Extensive hydrogen bonding with mucin is made possible by their high carboxyl group density, which improves adherence and prolongs retention. Controlled-release vaginal medication delivery systems benefit greatly from these polymers.[58]
Table No 2: Mucoadhesive Polymers
|
Polymer Category |
Representative Polymers |
Key Properties |
Mucoadhesion Mechanism |
Advantages in Vaginal Delivery |
Limitations |
References |
|
Natural Polymers |
Chitosan, alginate, pectin, gelatin, xanthan gum, guar gum |
Biocompatible, biodegradable, hydrophilic, low toxicity |
Hydrogen bonding, electrostatic interaction, gel formation, polymer chain interpenetration |
High safety, good patient acceptability, prolonged residence time |
Batch variability, lower mechanical strength |
59 |
|
Chitosan (Natural) |
Chitosan and derivatives |
Cationic, pH-sensitive, permeation-enhancing |
Electrostatic attraction with negatively charged mucin |
Strong mucoadhesion, enhanced drug absorption |
Solubility dependent on acidic pH |
60 |
|
Alginate & Pectin (Natural) |
Sodium alginate, calcium alginate, pectin |
Gel-forming, swellable, moisture responsive |
Hydrogen bonding and hydrogel formation |
Sustained drug release, good mucosal compatibility |
Weak adhesion under high fluid turnover |
61 |
|
Semi-Synthetic Polymers |
HPMC, CMC, HEC |
Controlled swelling, film-forming ability, stable viscosity |
Hydrogen bonding and polymer chain interpenetration |
Reproducible release, good mechanical properties |
Moderate mucoadhesive strength |
62 |
|
Cellulose Derivatives |
HPMC, CMC |
Non-ionic or anionic, inert, stable |
Physical entanglement and hydrogen bonding |
Suitable for films, tablets, gels |
Limited adhesion alone (often combined with others) |
63 |
|
Synthetic Polymers |
Carbopol, polycarbophil |
High molecular weight, pH-sensitive, high viscosity |
Extensive hydrogen bonding via carboxyl groups |
Strong and prolonged mucoadhesion |
Possible irritation at high concentrations |
64 |
|
Poly(acrylic acid) Derivatives |
Carbopol®, polycarbophil |
High carboxyl group density, strong swelling |
Hydrogen bonding with mucin glycoproteins |
Excellent retention, controlled drug release |
Requires pH optimization |
65 |
|
Polymer Combinations |
Chitosan+HPMC, Carbopol + HEC |
Synergistic mucoadhesion and release control |
Combined electrostatic and hydrogen bonding |
Improved adhesion and mechanical strength |
Formulation complexity |
66 |
6. Types of Mucoadhesive Vaginal Drug Delivery Systems
In order to increase residence duration, improve drug absorption, and improve treatment outcomes, mucoadhesive drug delivery systems (MDDS) for vaginal administration are made to stick to the vaginal mucosa. Conventional dose forms including creams, gels, and tablets frequently show limited retention and require repeated dosing for efficacy due to the vaginal tract's self-cleaning mechanism and constant mucus turnover. By utilizing polymer–mucin interactions to extend contact time and maintain medication release at the target region, mucoadhesive methods overcome these constraints.[67]The two main categories of mucoadhesive vaginal drug delivery methods are advanced particle and innovative technologies, as well as traditional semi-solid and solid formulations. The composition, adhesion method, drug release properties, and therapeutic uses of these dosage forms differ.[68]
6.1 Mucoadhesive Gels
Mucoadhesive gels, which are semi-solid formulations of mucoadhesive polymers like carbopol, hydroxypropyl methylcellulose (HPMC), chitosan, or poloxamer that hydrate upon contact with vaginal fluid and form a viscous gel matrix, are among the most widely used vaginal dosage forms because of their ease of application, flexibility, and capacity to spread evenly across the mucosal surface. The mucoadhesion of these polymers allows for gradual drug release. Mucoadhesive hydrogels that include antivirals or antibiotics to treat infections, contraceptives, or local anti-inflammatory medications are a few examples. Gel strength, swelling, and drug release kinetics are all influenced by the polymer and crosslinking selection.[69]
6.2 Mucoadhesive Tablets
When hydrated, solid dosage forms like mucoadhesive tablets and suppositories are made to progressively swell and stick to the mucosal surface, releasing the medication gradually over time. These formulations frequently include mucoadhesive polymers, such as pectin, chitosan, or polycarbophil, in a matrix that promotes adherence while preserving mechanical integrity.[70] Tablets are small, offer accurate dosage, and are relatively easy to manufacture and store. For ailments such vaginal infections or the preventive administration of microbicides, they can be made for controlled drug release. For instance, chitosan-based mucoadhesive tablets that show prolonged drug release and retention on vaginal mucosa ex vivo have been created for the sustained release of tenofovir, an antiretroviral medication for HIV pre-exposure prophylaxis.[71]
6.3 Mucoadhesive Suppositories
Suppositories are solid or semi-solid inserts that interact with vaginal mucous and release medication when they melt or dissolve at body temperature. They can have a long-lasting effect, particularly if they are made with bio-adhesive polymers that slow down clearance.[72]
6.4 Mucoadhesive Films
Mucoadhesive films are thin, flexible polymeric sheets that are intended to be placed in the vagina. They can stick to the mucosa and provide regulated drug delivery. Films combine the advantages of solid and semi-solid solutions with close mucosal contact, precision dosage, and convenience of insertion.[73] Typically, films are made by solvent casting polymers such polyvinyl alcohol, hyaluronic acid, or HPMC, frequently with plasticisers to guarantee flexibility. They are mechanically sound and can release medications over a few days. In order to treat bacterial vaginosis, a study created cross-linked hyaluronic acid-based mucoadhesive films. The films' ability to stay in place and release therapeutic doses of medication throughout long treatment durations was demonstrated.[74]
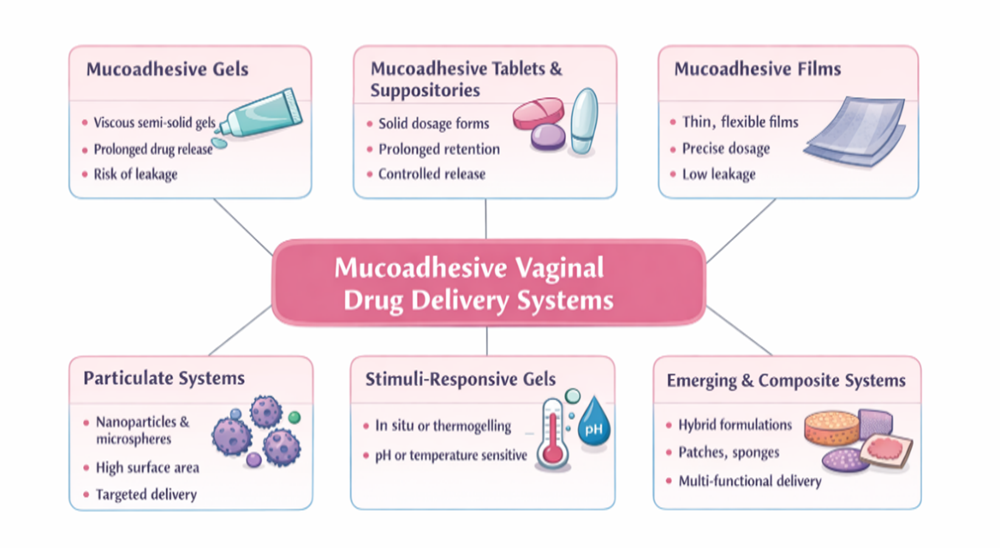
Fig No.2: Types of Mucoadhesive Vaginal Drug Delivery Systems
6.5 Particulate Systems: Microspheres and Nanoparticles
Particulate systems like mucoadhesive microspheres and nanoparticles have been thoroughly studied to further improve drug stability, mucosal contact, and controlled release. These solutions are superior to bulk gels or tablets in terms of surface area augmentation, targeted delivery, and diffusion control.[75] The purpose of microspheres, which typically range in size from 1 to 1000 µm, is to combine medication within a polymer matrix that interacts with mucin. They might be designed to swell or break down and offer sustained release.[76]Nanoparticles, which are usually smaller than 1 µm, provide benefits for surface functionalization and mucosal penetration. To enhance adherence and regulate release, mucoadhesive nanoparticles employ polymers such chitosan, PLGA, PEGylated surfaces, or thiolated derivatives. Reviews show that polymeric nanoparticles, which are designed for both local and systemic activity, are promising vaginal drug delivery vehicles for antimicrobials, antivirals, and anticancer medicines.[77]
6.6 Stimuli-Responsive and In Situ Gelling Systems
Stimuli-responsive or in situ gelling formulations, which change from liquid to gel when exposed to physiological circumstances (temperature, pH, or ions), are a subgroup of mucoadhesive delivery methods.[78] These solutions combine ease of application with improved retention because they often have low viscosity when administered and gel when they come into touch with vaginal secretions.[79]For example, in situ gels based on chitosan and poloxamer blends are examples of thermogelling copolymers that have been investigated for vaginal usage. These formulations create gels that stick to mucosa and prolong medication release by taking advantage of body temperature. Benefits include improved patient comfort and little leaking during implantation.[80]
6.7 Emerging and Composite Delivery Systems
To further improve medication retention and controlled distribution, ongoing research has investigated composite devices that combine various dosage forms, such as films embedded with nanoparticles or tablets with expandable mucoadhesive layers. Although they are less prevalent, advanced techniques include sponges, mucoadhesive patches, and cervix-targeted carriers.[81]
7. Evaluation Parameters for Vaginal Mucoadhesive Systems
In order to guarantee that the system will offer extended residence time, sufficient drug release, and therapeutic efficacy in the intricate vaginal environment, the study of mucoadhesive vaginal drug delivery systems is an essential stage in formulation development. In contrast to traditional dosage forms, mucoadhesive systems need to be evaluated for their adhesion behavior, mechanical integrity, and interaction with mucosal tissue in addition to drug release. To fully characterize these characteristics, several in vitro, ex vivo, and in vitro/permeation models have been documented in the literature.[82]
7.1 Mucoadhesion Testing
Effective adhesion to the vaginal mucosa strongly affects residence time and drug absorption, making it one of the most crucial evaluation metrics. Typical methods include of:
Tensile strength and the force needed to separate the formulation from mucosal tissue are measured using texture analyzers. Typical outputs include detachment force (Fdt) and work of adhesion (Wad).[83] Polymer–mucin contact is evaluated by rheological and indentation studies, which provide information about possible mucoadhesive behavior. Residence time tests (wash-off or immersion models) measure the length of adhesion by subjecting formulations to simulated vaginal fluid in order to replicate the vaginal environment.[84]
7.2 Swelling and Hydration Studies
Mucoadhesive performance is influenced by swelling behavior in two ways: sufficient swelling promotes polymer chain entanglement with mucin, whereas excessive swelling might reduce adherence by diluting functional groups. These investigations measure the amount of water absorbed over time and are frequently associated with mucoadhesive strength.[85]
7.3 In Vitro Drug Release
For mucoadhesive systems to be therapeutically effective, controlled and prolonged drug release is necessary. Release investigations are carried out utilizing Franz diffusion cells or dissolving apparatus under simulated vaginal circumstances (pH ~4.2–4.5) to provide release kinetics, which are then frequently fitted to mathematical models to comprehend release mechanisms.[86]
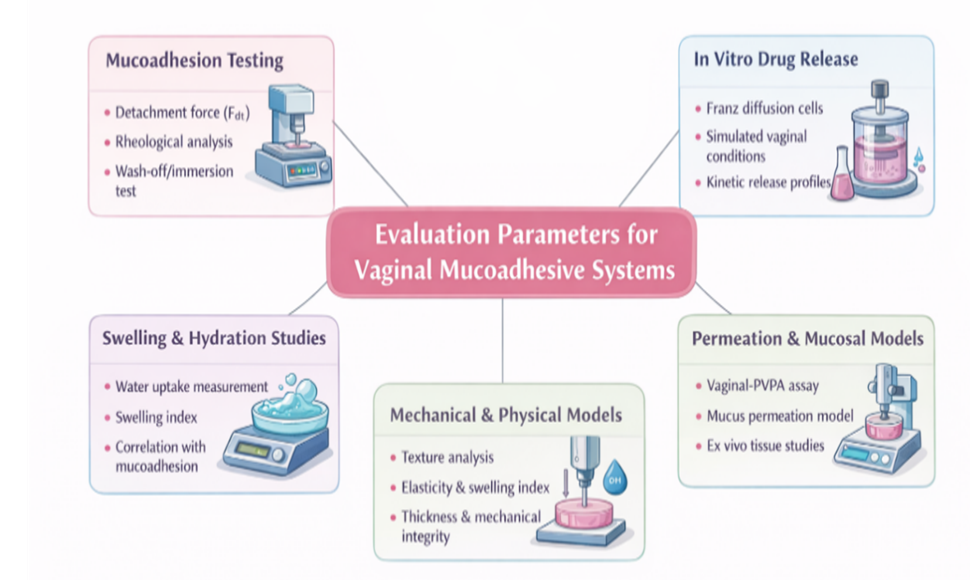
Fig No. 3: Evaluation Parameters for Vaginal Mucoadhesive Systems
7.4 Permeation and Mucosal Models
Drug penetration in the presence of mucus and simulated vaginal fluid is tested using sophisticated in vitro permeation models such as the vaginal-PVPA (Phospholipid Vesicle-based Permeation Assay), which replicates the mucosal barrier. These models offer vital information about how medicine penetrates the mucosa and how formulations interact with mucus.[87]
7.5 Mechanical and Physical Characterization
To make sure the formulation can tolerate handling and self-cleaning forces in vivo, parameters such textural strength, elasticity, swelling index, thickness, and mechanical integrity are assessed.[88]
8. Therapeutic Applications of Vaginal Mucoadhesive Drug Delivery Systems
Because they can increase drug localization, extend residence duration at the site of administration, and improve therapeutic outcomes for both local and systemic applications, vaginal mucoadhesive drug delivery systems are being investigated more and more. By permitting sustained and controlled medication release and overcoming fast clearance caused by vaginal self-cleaning processes, these methods provide notable advantages over traditional formulations.[89]Vaginal illnesses, such as bacterial vaginosis, vulvovaginal candidiasis, and sexually transmitted infections (STIs), are among the main therapeutic uses of mucoadhesive vaginal delivery systems. Improved mucoadhesion improves localized medication action and reduces systemic adverse effects by increasing the retention of antibacterial drugs at the mucosal surface.[90] Mucoadhesive systems based on hydrogel or nanoparticles have been studied for the delivery of antivirals, antifungals, and antibiotics to successfully prevent the growth of pathogens and the formation of biofilms. Additionally, these systems improve drug penetration to the infection site by overcoming diffusion restrictions within mucus.[91]Contraceptive delivery also uses mucoadhesive vaginal systems. Spermicidal chemicals or hormone formulations can be added to polymeric gels, films, or rings for extended release and localized action, which can increase the effectiveness of contraception while lowering dosage frequency and irritation. These systems can serve two purposes at once, such as combining STI prevention with contraception.[92] Vaginal mucoadhesive systems have potential for systemic medication administration of peptides, hormones, and vaccinations in addition to local therapy. Certain medications can avoid first-pass hepatic metabolism due to the vaginal mucosa's strong vascularization, providing an alternate pathway for substances with low oral bioavailability.[93] Mucoadhesive systems have been tested to improve absorption and lower dosage frequency for hormonal therapy (such as oestrogen administration for menopausal symptoms).[94]All things considered, these applications show that mucoadhesive vaginal drug delivery methods not only increase local therapeutic efficacy but also broaden the scope of innovative systemic medicines while improving patient comfort and compliance. It is anticipated that when polymers and formulation techniques continue to be improved, their clinical impact will increase.[95]
9. Recent Advances and Future Perspectives in Vaginal Mucoadhesive Drug Delivery System
Recent studies on vaginal mucoadhesive drug delivery systems (MDDS) have concentrated on using new materials, sophisticated formulations, and multifunctional carriers to improve therapeutic performance and overcome physiological obstacles of the vaginal environment. Significant advancements have been made in customizing mucoadhesive systems for more efficient local and systemic drug delivery, despite the persistent difficulties presented by fast mucus turnover, pH fluctuations, and enzymatic activity.[96]The incorporation of stimuli-responsive and in situ gelling polymers, which alter chemically or physically when they come into touch with vaginal secretions, is one important area of development.[97] In order to improve residence time and drug release management, these systems are made as low-viscosity liquids at the moment of administration but change into gels in response to temperature, pH, or ionic concentrations. This method is a potential option for long-term treatments and continuous drug delivery since it not only improves mucoadhesion but also lowers leakage and improves patient comfort.[98]The application of nano and micro based carriers in mucoadhesive matrices is another significant area of development. Polymeric micelles, liposomes, solid lipid nanoparticles, and nanoparticles (NPs) have all been studied to enhance medication stability, mucus barrier penetration, and targeted action.[99] These carriers' interaction with mucin fibres is increased by surface modification with mucoadhesive polymers or mucus-penetrating ligands, which prolongs retention and improves therapeutic results. These nanosystems have shown promise in delivering hormonal, antiviral, antifungal, and antibacterial drugs more efficiently than traditional versions.[100]The design space for vaginal mucoadhesive systems has also increased due to developments in functionalized polymers and excipients. To optimize medication release and mucosal contact, new biocompatible and biodegradable excipients with multifunctional qualities—such as pH responsiveness, increased swelling, and improved bioadhesive strength are being used.[101] A greater focus on precision formulation engineering, which allows for customized treatment for certain vaginal conditions, is shown in this trend.[102]
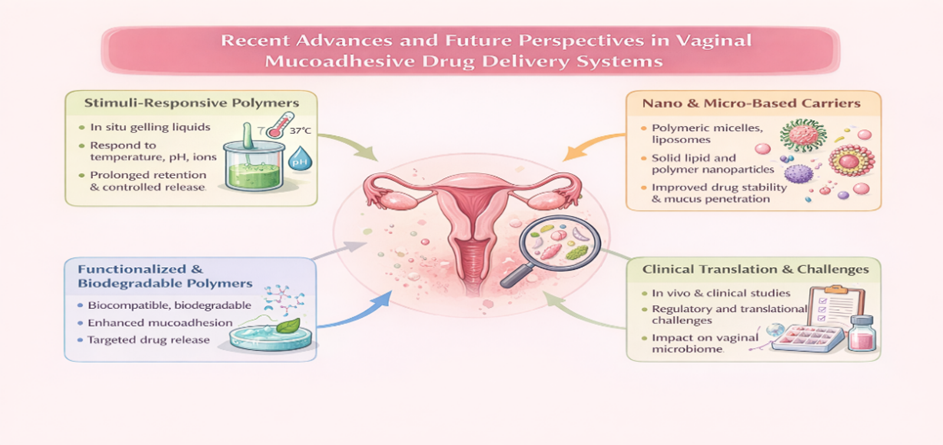
Fig No.4: Recent Advances and Future Perspectives in Vaginal Mucoadhesive Drug Delivery Systems
Clinical translation and regulatory adoption of these cutting-edge systems are the main areas of focus for the future. Extensive in vivo and clinical evaluations are necessary to establish safety, efficacy, and patient compliance, even though in vitro and ex vivo investigations provide encouraging results.[103] For practical use, more investigation into mucus-penetrating versus mucoadhesive balance, long-term tolerability, and the effect of formulation on the native vaginal flora is essential.[104]The future of vaginal MDDS is being shaped by current developments in stimuli-responsive gels, nano carriers, functional polymers, and formulation excipients.[105] These technologies show great promise for improved local therapy and non-invasive systemic delivery while resolving present vaginal drug delivery constraints with further interdisciplinary research and thorough clinical validation.[106]
CONCLUSION
A very promising and adaptable method for enhancing both local and systemic drug therapy via the vaginal channel is the use of vaginal mucoadhesive drug delivery systems (MDDS).[107] The vaginal mucosa is a desirable site for drug delivery due to its distinct anatomical and physiological characteristics, which include extensive vascularization, a wide surface area, and avoidance of first-pass hepatic metabolism. However, quick clearance, poor retention, and unpredictable therapeutic results are common limitations of traditional vaginal dose formulations.[108] By extending residence time, improving mucosal contact, and facilitating sustained and regulated medication release, mucoadhesive systems have been created to address these issues.[109]The design and functionality of vaginal mucoadhesive drug delivery devices have significantly improved because to recent advancements in polymer science.[110] A variety of delivery platforms, such as gels, tablets, films, microspheres, nanoparticles, and in situ gelling systems, have been made possible by the availability of natural, semi-synthetic, and synthetic mucoadhesive polymers.[111] These formulations have shown increased effectiveness in treating hormonal therapy, vaginal infections, contraception, and new uses like peptide and vaccine administration. Additionally, new developments in stimuli-responsive polymers and nanotechnology-based carriers have improved patient acceptance, medication stability, and bioavailability.[112]The successful clinical translation of vaginal mucoadhesive systems necessitates careful evaluation of safety, biocompatibility, impact on vaginal microbiota, and long-term tolerability, despite significant progress. Robust in vivo and clinical trials, mucus–polymer interaction optimization, and regulatory standardization should be the main topics of future study.[113]
REFERENCES







Kadam Swapnil, Patil Snehit, Patil Rajvardhan, Shirke Sanket, Kadam Vasundhara, Sulgudle Shivraj, Dr. Gejage Santosh, Mucoadhesive Drug Delivery Systems for Vaginal Administration, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 1853-1876. https://doi.org/10.5281/zenodo.18620462
 10.5281/zenodo.18620462
10.5281/zenodo.18620462