
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Annasaheb Dange College of B Pharmacy, Ashta, Sangli, Maharashtra, India
This study focuses on improving the delivery and effectiveness of antifungal medications through the skin using novel transdermal formulations. The skin, being the body’s largest organ, serves as a natural barrier that limits drug penetration. To overcome this, advanced systems like transferosomes ultra-flexible lipid vesicles are explored for their ability to transport drugs deeply and efficiently across skin layers.The project reviews current challenges in topical antifungal therapy, including poor drug permeability and resistance, and highlights the advantages of Transdermal Drug Delivery Systems (TDDS) such as enhanced bioavailability, avoidance of first-pass metabolism, and controlled release. Transferosomal gels, in particular, show promise due to their biocompatibility, high deformability, and ability to deliver both hydrophilic and lipophilic drugs. A series of evaluation tests including pH, spreadability, drug content, diffusion, stability, and skin irritation studies were performed to ensure safety, uniformity, and sustained drug release. The report also discusses the role of pharmacists in dermatological care and the growing influence of Artificial Intelligence (AI) in diagnostics and treatment. In conclusion, the project demonstrates that transferosome based transdermal systems offer a safe, efficient, and patient friendly approach for antifungal therapy, representing a significant step toward next-generation skin drug delivery.
INTRODUCTION TO SKIN
The skin biggest organ of the human body. It covers and protects everything inside us. It works like a shield to stop germs, dirt, chemicals, and harmful things from entering the body[1].
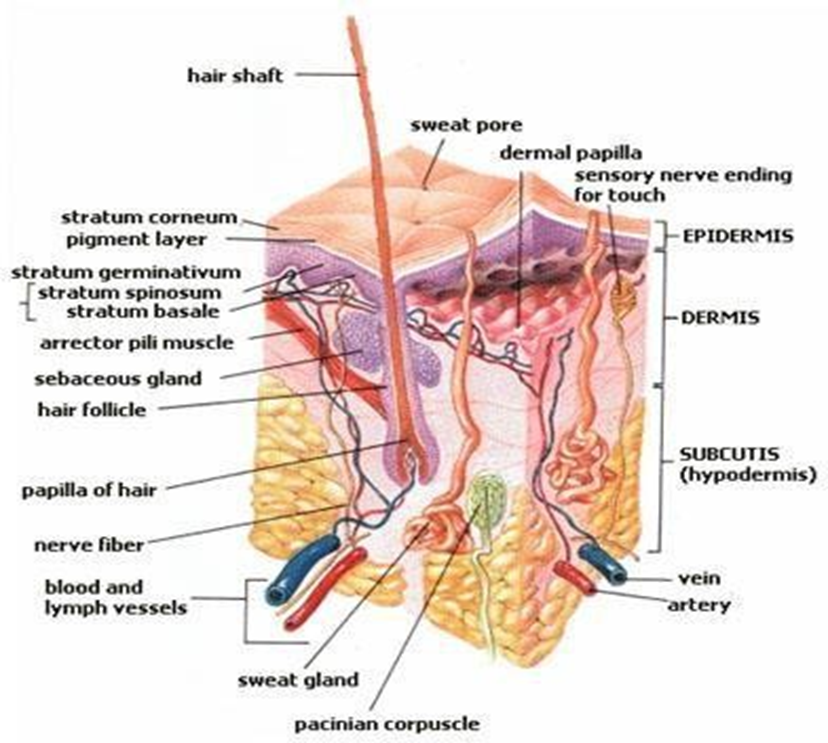
Fig 1. Cross sectional area of skin
It consists of three main structural layers:
|
Skin Layers |
Description |
|
Epidermis |
Outermost layer, avascular, made of 5 distinct sublayers (stratum layers). |
|
Dermis |
Lies beneath the epidermis, provides structural support, elasticity, and contains blood vessels and nerves. |
|
Hypodermis |
Subcutaneous layer, composed mainly of adipose tissue, connective tissue, and blood vessels, providing cushioning and insulation. |
The epidermis is avascular and varies in thickness depending on the body location. It is thinnest on the eyelids and thickest on the heels. Areas exposed to constant friction (such as fingertips or soles) develop thicker layers. Although devoid of true nerves, free nerve endings from the dermis extend into the mid-epidermis.
|
Layer (Superficial Deep) |
Key Features |
|
Stratum corneum |
15–30 layers of dead keratinocytes (corneocytes), rich in keratin, providing a waterproof barrier. Cells are continuously shed and replaced (cell cycle ~30 days). |
|
Stratum lucidum |
Found only in thick skin (palms, soles). Composed of 2–3 non-living keratinocyte layers. |
|
Stratum granulosum |
Contains the highest concentration of free nerve endings. Last living cell layer of the epidermis. |
|
Stratum spinosum |
Contains Langerhans cells and lymphocytes; important for immune defense. |
|
Stratum basale |
Basal layer; only layer undergoing continuous mitosis. Produces keratinocytes which migrate outward. |
The dermis provides structural support and nourishes the epidermis. It is highly vascular and innervated.
• Papillary Layer: Interdigitates with the epidermis, forming fingerprints. Contains fibroblasts that produce collagen and elastin, giving strength and elasticity.
• Reticular Layer: Lies between the papillary dermis and hypodermis. Contains dense collagen fibers, blood vessels, nerves, immune cells, hair follicles, and glands. Hair follicle stem cells aid in wound healing.
The hypodermis (subcutaneous tissue) is composed of adipose tissue and loose connective tissue. It is well vascularized and innervated. Functions include:
Functions of the Skin
AIM & OBJECTIVES:
Aim
To investigate novel formulation strategies that enhance the bioavailability and sustained release of antifungal agents through the skin.
Objectives
LITERATURE REVIEW
Studied the information carried out in this review is about the anatomy and physiology of the skin and various permeation factors of the skin
Studied the information is carried out in this review about the skin and barriers of the skin
Transferosomes are ultra-flexible lipid vesicles designed to deliver drugs through the skin more effectively than traditional creams or liposomes Topical gels, when combined with transferosomes, enhance drug stability, absorption, and patient comfort..
Studied the information about what are the advancements in the dermatology and the role of the AI in advancement.
Delivering drugs through the skin is appealing because it avoids needles or a pill’s journey through the gut – but the skin’s outer layer (the stratum corneum) is a formidable barrier. This review focuses on a clever solution: transferosomes, which are ultra-flexible lipid vesicles designed to squeeze through skin pores and deliver a wide variety of therapeutics (even big ones like proteins and nucleic acids) rather than only small lipophilic drugs.
Studied the information carried out in this review is about the introduction to fungal infection and types of the fungal infections like superficial , subcutaneous and systemic mycoses.
Studied about the various skininfections mainly about the parasitic infections of the skin.
Studied about the information carried in this review is about skin diseases mainly about viral skin infections .
Studied the information about the antifungal agents in21st century its Advances, Challenges and future perspectives and various perspectives about the resistenace of the antifungal agents , limitations of the current antifungal agents.
Studied the information carried out in this review is about the anatomy and physiology of the skin and different layers of the skin and permeation through the various layers of the skin.
Fungal infections are a growing global concern, especially among people with weakened immune systems. Conventional antifungal creams often fail to deliver sufficient drug concentrations through the skin’s tough outer layer, the stratum corneum. To address this, researchers have developed transferosomes—ultra-flexible lipid vesicles that can squeeze through tiny skin pores and deliver drugs more effectively
Artificial Intelligence (AI) is rapidly transforming healthcare by improving diagnostic accuracy and efficiency, especially in fields like dermatology. AI-powered image analysis systems can now detect and classify skin conditions such as melanoma, eczema, and ulcers with high precision—sometimes outperforming dermatologists.
Transdermal drug delivery is an effective alternative to oral or injectable routes but is limited by the skin’s barrier layer. Transferosomes, flexible lipid vesicles made with phospholipids and surfactants, overcome this issue by enhancing drug penetration.
INTRODUCTION TO TDDS:
Drug administration via skin has effective approach in drug delivery .transdermal drug delivery is innovative term in pharmaceutical field of drug administration. Large dose is required and larger regimen to get therapeutic effects in Conventional drug delivery system, it has major side effects due to longer regimen which effects on patient compliance , patient may be skip the dose fluctuation in drug plasma level may occur due to avoid such kind of complications transdermal drug delivery system is used in drug administration.
TDDS is improved delivery of many pharmacological activities such as drugs, hormones , therapeutic agents, proteins and RNA based therapeutics which can degraded in GIT due to acidic environment. TDDS gives vital contributions in medicine field to achieve full potential
Transdermal delivery of particle is largely limited for SC lipids. It mainly depends upon molecular size and hydrophobicity / hydrophilicity of drug various methods developed to overcome this problem such as use of penetration enhancer, electrical impules , ultrasound etc.
TDDS delivers the solutes by following three routes:
1. Trans-appendageal route (shunt route)
2. Intracellular (Transcellular) route
Here, the drug passes through the skin cells (called corneocytes) in the outer layer.
3. Intercellular route
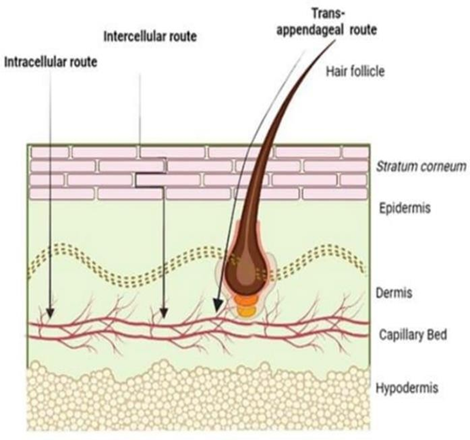
Fig 2. Permeation routes of TDDS
Advantages of TDDS:
Disadvantages of TDDS:
Various formulations permeation through TDDS:
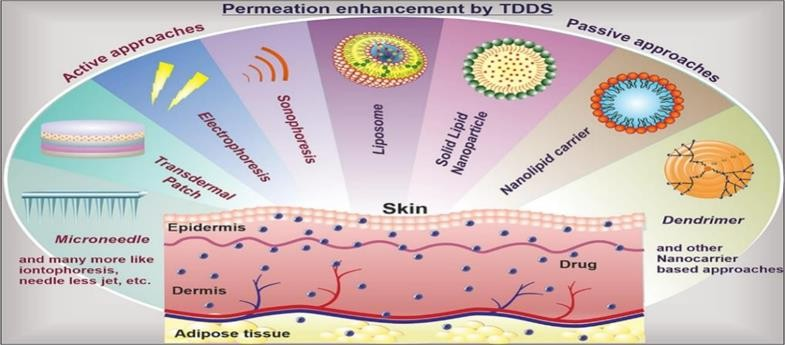
Fig 3.Overcoming skin barrier through TDDS[5].
Skin Diseases
Extrinsic Diseases
Caused by parasites. In parasitic infections it involves the skin and subcutaneous tissues. Depending on the species of then its involvement is transient, the parasite passing through the skin and migrates into the blood stream and at the specific site of the targeted organ or infection may get localized to skin [6].
Caused by viruses. Skin diseases due to the viruses occurs they may be primary infection of the epidermis or may arises as the secondary infections to the skin . It depends on the viruses they may cause necrotic damage of the infected cells.
Caused by bacteria. Also called as pyroderma this disease often commonly start as primary skin problem like impetigo or they appear as secondary in places where skin is already damaged .The main bacteria responsible are streptococci and staphylococcus aureus it can also cause folliculities (infection of hair roots).
Caused by fungi. They are most common everywhere .They include ringworm (dermatophytosis), candidiasis, infections from malassezia (like pityriasis versicolor and other fungal infections such as scytalidium that often affects on feet. A common example is athelets foot (tinea pedis)[7].
Intrinsic Skin Diseases
Fungal Infections
Definition: Fungal infections (mycoses) are caused by fungi, either molds or yeasts. They commonly affect the skin and nails but may also involve the mouth, throat, lungs, urinary tract, or internal organs.
Fungi Characteristics:
Need of focusing on fungal infections:
Before the medical advances severe fungal infections are less common. This rise of invasive and skin fungal infections are due to:
Antifungal resistance is also a one of the consequences. It is an escalating health concerns contributes to invasive fungal infections [9].
Types of Fungal Infections
Superficial fungal infections are common everywhere, but they occur more often in hot and humid climates. These conditions make the skin more prone to infections like dermatophytosis or Malassezia. The exact reason is not clear, but higher levels of carbon dioxide (Pco2) on the skin surface may help fungi grow and invade. Examples include tinea Pedis (athlete’s foot) and tinea infections in other body areas.
These infections mainly occur in tropical and subtropical regions. They are called implantation mycoses because the fungi enter the body through the skin, usually after a minor injury. The fungi are normally found in soil or plants and get into the skin or tissue under the skin when pricked, often by thorns. Many patients do not remember the injury that caused the infection.
Systemic fungal infections affect deep organs such as the lungs, liver, and spleen. They can also spread through the blood to the skin and mucous membranes, causing widespread or localized disease [10].
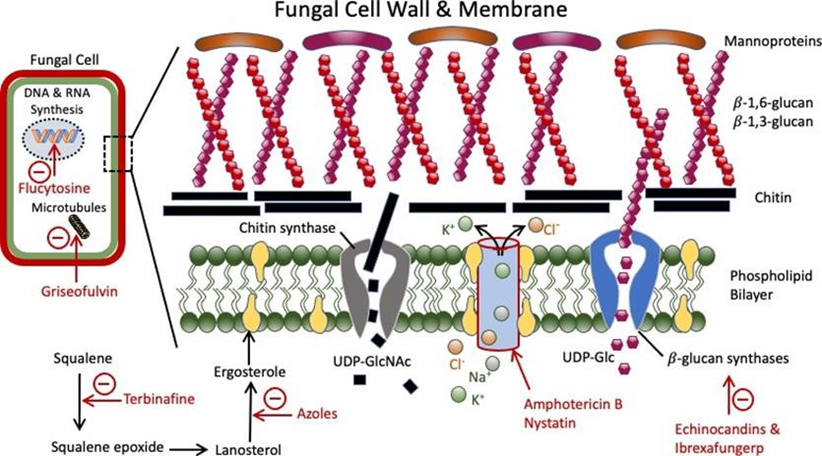
Fig 4.Mechanism of antifungal agents
Management and Treatment :
Vary depending on the site and severity of infection:
|
Form |
Administration |
Use |
|
Oral (tablets/ capsules) |
Systemic treatment |
Skin/ nail infections |
|
IV therapy |
Hospital setting |
Severe systemic infections |
|
Lotions, creams, powders |
Topical treatment |
Local skin mycoses |
|
Mouthwash/ lozenges |
Oral cavity infections |
Oral thrush |
|
Eye drops |
Ophthalmic fungal infections |
Keratitis, endophthalmitis |
|
Shampoo |
Scalp infections |
Tinea capitis, seborrheic dermatitis |
Antifungal medications:
Based on their chemical structures:
|
Antifungal agents |
Drugs |
Mode of action |
|
Azoles |
Econazole, voriconazole, traconzole ketoconazole, cotrimazole ,econazole |
Inhibition of lanosterol 14a- demethylase |
|
Echinocandins |
Capsofungin , micafungin |
Inhibition of 1,3 b – glucan synthase |
|
Polyenes |
Amphotericin B ,nystatin |
Binding to ergosterol |
|
Pyrimidine analogues |
Flucytosine |
Inhibition of DNA /RNA/ Protein synthesis |
Various formulations:
Transferosomes:
Transferosomes are ultra-flexible vesicles developed in the 1990s to improve drug delivery through the skin. They are made from phospholipids, cholesterol, and special surfactants called edge activators, which make them highly deformable and able to pass easily through the skin barrier. Unlike regular liposomes or solid lipid nanoparticles, transferosomes can carry both water-loving and fat-loving drugs, including small and large molecules. Their flexibility allows them to deliver higher amounts of drugs deep into the skin and even into the bloodstream. They are especially useful for controlled and targeted drug delivery [11].
Advantages:
Disadvantages:
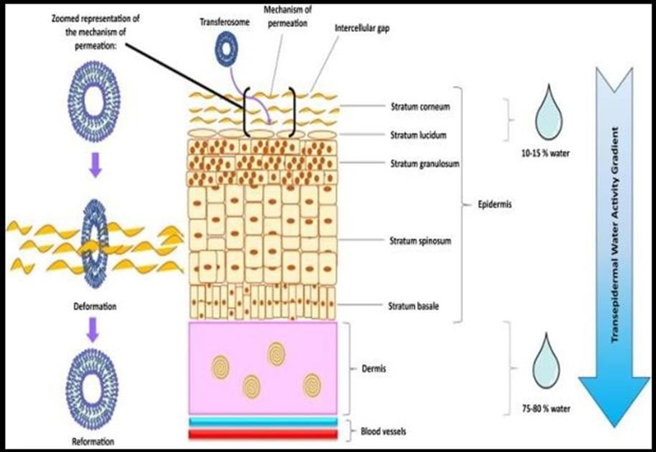
Fig 5. Mechanism of permeation through transferosomes
Basic components of transforesome gel:
1. Drug:
|
Sr. no |
Parameters |
Properties |
|
1 |
Molecular weight |
Less than 500 Daltons |
|
2 |
Lipophilicity |
Log P between 1 & 3 |
|
3 |
Melting point |
Less than 200 |
|
4 |
Pka |
5.5 to 6.5 |
|
5 |
Skin reaction |
Not irritating, not sensitizing |
2. Components:
|
Sr. no |
Class |
Example |
Use |
|
1 |
Phospholipids |
Egg Phosphatidyl Choline, Soya Phosphatidyl choline, di palamitoyl phosphatidyl choline |
Vesicle forming compound |
|
2 |
Solvent |
Ethanol, methanol, isopropyl alcohol, chloroform |
As a solvent |
|
3 |
Surfactant |
Sod. Chelate, Sod. Deoxycholate , Tween- 80, Span 80, Tween 20 |
Edge activator |
|
4 |
Buffering agent |
Saline phosphate, phosphate buffer |
As a hydrating medium |
METHODS OF PREPARATION:
The drug (API), lecithin, and edge activator are mixed in equal parts of chloroform and ethanol and shaken manually at a temperature higher than the lipid’s melting point.
The mixture is left to evaporate, removing the organic solvents and leaving a thin lipid film overnight
The lipid film is then hydrated by rotating it at 60 RPM for 1 hour at room temperature using a pH 6.5 buffer.
The remaining vesicles are allowed to swell for 2 hours at room temperature
Finally, small vesicles are made by sonication of the swollen vesicles at room temperature
Lipids and organic solvents are mixed in a round-bottom flask while purging with nitrogen.
The drug is added to either a fat-loving (lipophilic) or water- loving (hydrophilic) medium, depending on its solubility
The mixture is sonicated and then left for 30 minutes to form a uniform Mixer
The organic solvents are removed under low pressure.
The remaining mixture turns into a thick gel, which forms the vesicles.
Phospholipids and edge activators are mixed by continuous swirling in phosphate buffer. This forms a milky suspension.
The suspension is then sonicated in a sonicator bath.
Finally, it is passed through polycarbonate membranes to form uniform vesicles.
This method is considered better than others.
The drug and water are warmed at a constant temperature with continuous stirring.
Phospholipids and edge activators are mixed in ethanol.
Then added to the aqueous drug solution They react together to form the vesicles.
In this process, the organic solvent, lipophilic drug, phospholipids, and edge activator are added into a round- bottom flask.
All these ingredients are mixed until a clear solution is formed.
Instead of using a vacuum evaporator, the solvent is removed by shaking the flask by hand.
The flask is placed in a warm water bath (about 40–60°C). As the solvent evaporates, a thin layer of lipids forms on the inner wall of the flask.
The flask is then kept overnight to let the solvent fully evaporate. The next day, the thin lipid film is gently shaken and hydrated with a suitable buffer solution at a temperature above its phase transition point
Evaluation tests:
PH tells us whether the gel is acidic, neutral, or basic.
PH meter is used because it gives a very accurate value. Before checking the gel, the pH meter is calibrated using standard solutions (pH 4, 7, 9).This makes sure the reading is correct. The electrode of the pH meter is dipped into the gel sample. Wait for the reading to become stable, then write it down observations. This test is done 3 times (triplicates) on different samples to avoid error. Final PH is reported as the average of the 3 readings. Skin pH is around 5.5, so gels should ideally be close to skin PH to avoid irritation [16].
Spreadability means how easily the gel spreads on the skin. Good spreadability helps in better drug absorption and patient comfort. Gel is placed between the slides. Weight pulls the upper slide, and the gel spreads. The distance the slide moves and time taken is measured.
Spreadability is calculated using the formula:
S = ???? × ???? ÷ ????
Where:
The test is repeated 3 times and the average is taken as final value.
Higher S value = Gel spreads faster. It is better patient application
Too runny gel = poor retention on skin
Too thick gel = difficult to apply
To check how much drug is actually present in the gel, we first calculate the amount of drug that should be in one normal dose. Then, we take at least 6 gel samples from different places (because gel is thick and can be uneven) to make sure the drug is spread evenly. These samples are then tested using a proper laboratory method (like UV-spectroscopy or HPLC) to confirm the correct drug content.
The drug release from the gel is tested in the lab using a Franz diffusion cell.
A dialysis membrane is placed between: Donor compartment in transferosome gel (one dose) & Receptor compartment in phosphate buffer (pH 7.4), which acts like body fluid The setup is kept at 32°C (similar to skin temperature) and stirred at 50 rpm to mimic real skin conditions. Samples are taken from the receptor compartment at different time intervals through a side tube. Each sample is then analyzed to check how much drug has passed through the membrane.
Guinea pigs (400–500 g) were used to check whether the gel causes irritation on the skin. They were kept under normal lab conditions with proper food and water. Hair from the back of each animal was shaved, and two small areas (4 cm² each) were marked. One for the test gel and the other as control (no gel). The gel (500 mg per animal) was applied twice daily for 7 days. The skin was checked regularly to see if there were any signs of irritation such as:
This helps determine if the gel is safe and non-irritating for topical use.
All gel samples were checked under a light microscope to ensure there were no visible particles or rough materials in them. A good gel should feel smooth on the skin, so being free from grit or particles
To check if the transferosomal gel remains stable during its shelf life, it is stored under accelerated conditions (higher temperature and humidity). At specific time intervals, important parameters are tested again, such as:
These tests help confirm that the formulation remains effective and unchanged during storage.
This test checks how easily the gel comes out of its tube. The gel is packed in collapsible tubes, and pressure is applied to squeeze out the gel. The weight (in grams) needed to push out a 0.5 cm strip of gel in 10 seconds is recorded.
A good gel should:
Role of Pharmacists in Dermatology
Advancements in Dermatology
CONCLUSION
This report details a project aiming to enhance the delivery and sustained release of antifungal agents through the skin using novel formulations. It begins with an overview of the skin's anatomy and physiology, highlighting the skin as the body's largest organ, which acts as a protective barrier. The skin is composed of three main layers: the Epidermis (the avascular, outermost layer with the waterproof Stratum corneum), the Dermis (providing structural support, containing blood vessels and nerves), and the Hypodermis/Subcutis (a subcutaneous layer primarily made of adipose tissue for cushioning and insulation). The report then addresses the major health concern of fungal infections (mycoses), which are increasing in prevalence and often face challenges like antifungal resistance. These infections can be superficial, subcutaneous, or systemic, and current treatments involve various forms such as oral tablets, topical creams, and IV therapy. To overcome the limitations of conventional therapy, the report focuses on the Transdermal Drug Delivery System (TDDS), an innovative approach that avoids first- pass metabolism and improves bioavailability. Finally, the report outlines a comprehensive set of evaluation tests essential for confirming the quality and safety of the final transferosomal gel formulation.
REFERENCES




Rohan Patil, Sanika Jagadale, Omkar Yadav, Sakshi Vibhute, Nanotechnology-Based Transdermal Systems for Antifungal Therapy: Emphasis on Transferosomal Gels, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 1135-1148. https://doi.org/10.5281/zenodo.18519609
 10.5281/zenodo.18519609
10.5281/zenodo.18519609