
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, The Oxford College of Pharmacy, Bengaluru, Karnataka, India
A common skin condition ‘melasma’ which is signalized by the occurrence of dark, blotchy patches on sun-stroked areas, especially the face, particularly affecting women during their reproductive years. Despite its prevalence, the true cause of melasma has recorded to remain puzzled, with change in hormone, heat stroke, and genetic factors which has been identified as potential triggers. A comprehensive exploration of melasma is provided in this article, with its historical recognition as a distinct dermatological concern associated with altered hormones and environmental influences being traced. The classification of melasma is summarised in brief, that makes it easier to distinguish between transient and persistent types of its kind on the basis of pigmentation patterns and depth. The cross-work of genetic liability, hormonal fluctuations, and UV radiation in melasma's development is unravelled, highlighting its multifactorial nature. Different treatment methods and options are discussed, ranging from topical creams containing ingredients like kojic acid, azelaic acid, and hydroquinone to advanced therapies like chemical peels and laser treatments. The evaluation parameters and criteria for assessing the quality of topical creams, including their efficacy, safety, and tolerability, are also examined. Despite the challenges in managing melasma due to its complex etiology, ongoing research aims to explore alternative agents and combination therapies for improved outcomes, emphasizing the need for further investigations to enhance treatment strategies and ensure patient safety.
Melasma is a most commonly procured condition of hyperpigmentation issue, resulting in darker, blotchy and uneven skin tone on sun exposed areas, mainly observed on face. Women are more susceptible to this condition in comparison to men. As it generally appears for the First time during reproductive age or pregnancy1. Originating from the Greek word “melas”, referring black, characterising the patchy brown clinical representation. This skin ailment is also known as ‘chloasma’, ‘mask of pregnancy’ or ‘pregnancy mask’. With an exactly unknown etiology of the condition, it still has various triggering factors that influences the development of melasma. Like pregnancy, sun tanning, often use of oral birth controls, steroid administration, intake of improper diet, ovarian tumours, gastrointestinal parasitosis, replacement of hormone, over use of cosmetics and stressful events2. Clinical classification of melasma briefly has three types. Classification is done on the basis of the distribution of hyper pigmented lesions ranging as a single lesion or multiple lesions formed symmetrically normally on forehead, cheek, upper lip and chin. The clinical classifications are recognised as, I. The centofacial pattern, where the pigmentation appears on forehead and chin, II. The malar pattern, hyperpigmentation around cheeks. III. The mandibular pattern, Involvement of regions around mandibula3. Further melasma is histologically classified as a. Dermal, b. Epidermal, c. Intermediate, d. Mixed type. This histological classification is based on the Wood’s light test 4 , which is also used for the clinical assessment of melasma5 . However, melasma can be treated with topical creams. ‘Creams,’ being the important part of cosmetic products, intended for the topical application for a very long time due to its ease in applying and removal property. Medicated creams have a wide range of applications, including beautifying, cleansing, moisturizing, altering appearance, demalanising, and providing skin protection against infections caused by bacteria and fungus, and healing burns, cuts, wounds, as well as lightening scar marks on the skin. Out of various cosmetic products available today, the topical creams are found out to be more efficient in the treatment of epidermal melasma. Combinations of demelanising agents with varying concerntration are incorporated within the cream that are intended for treatment of melasma for several months to achieve noticeable significant clinical benefits by lightning the patchy appearance on the skin6.
History
Individuals of Asian region may have greater susceptibility to pigmentation related skin diseases. Despite having elevated melanin levels in skin, people of Asian descent still facing hyperpigmentation. Melasma is one such condition observed on face. Melanosis, “black degeneration” was the foremost phrase to depict a condition comprising obscuration in the structures viscerals. In 1910, localized skin melanosis was reported and in the following year, the term ‘Chloasma’ was devised to outline facial discolouration. In 1980, it was speculated that the disease is associated with lack of vitamin C and other etiologies7. Dr. G. Pernet initially described melanosis that was limited to the skin in 1910. He presented microscopic slices of skin samples showing early epithelial degradation, slow-growing melanosis cutis, and visible melanocytes. In 1922, the medical literature saw the re-emergence of melanosis cutis, linked with melanotic carcinoma. This connection was highlighted in a case study involving a patient who had experienced central pallor, depigmentation, and the gradual development of a rough, black to dark brown patch of hyperpigmentation on thenar prominence of their left hands thumb over a span of 16 years. Melanised pigmented cells, either superficial or deep, originated in the vicinity of the neural tube to safeguard the central nervous system and later extended into the skin7. A case of facial melanosis in 1959 led researchers to conclude that exposure to "cutting" oil was the source of the hyperpigmentation in men. Three melasma patterns are malar, mandibular, and Centro facial, were clinically identified in the 1980s7. Early in the 1980s, research on "idiopathic melasma" was conducted in addition to pattern definition. Among them was melasma unconnected to pregnancy, usage of OCP, prostate cancer treated with diethylbestrol, or conjugated oestrogen usage in hormone replacement therapy (HRT). The investigation concluded that different treatment suggestions were made depending on the size of the patches and the degree of melanosis8.

Fig. 1: Comparison between normal and melasma skin
Classification
Based on History

Fig. 2: Distribution pattern of melasma
Based on Depth:

Fig. 3: Types of melasma
Pathogenesis
Genetic Predisposition
Emphasizing the significance of family history as a contributor to melasma development supports the idea of genetic predisposition. Despite this, no gene association studies have been conducted on melasma up to date. Some studies report a 55-64% occurrence of a positive family history among melasma patients across worldwide8. Patients having Fitzpatrick skin types (FST) II and III exhibit a lower likelihood of having positive family history compared to those who have darker skin types (IV-VI) 9. Considerable variation exists in melasma prevalence across diverse ethnic populations1. An Indian study reported a positive family predisposition in 20% of cases9. Epidemiological indicators suggest facial melasma likely follows a dominating inheritance pattern, with exposure factors triggering disease development in genetically vulnerable individuals10. Thus, abnormal gene expression is speculated to hold significant implications in the melasma pathogenesis.
Hormonal Influence
Melasma is more prevalent in females than males, with country-specific variations in female to male ratios (e. g., 4:1 in India and 21:1 in Singapore). This female dominance implies a potential involvement of female sex hormones in the onset of melasma, as evidenced by the increased prevalence during pregnancy, use of oral contraceptive and other hormonal therapies9. In the last trimester of pregnancy, melanogenesis stimulations increase, with sex steroids inducing melasma synergistically with UV exposure. In men finasteride, an anti-androgen is the one that might trigger melasma11.
The mechanism of action for female sex hormones (oestrogen and/or progesterone) in hyperpigmentation has not been thoroughly explored. Some studies suggest that, Oestrogen enhances melanin synthesis in melanoma cells by activating the cAMP- protein kinase A (PKA) pathway. Recent investigation identifies PDZ domain containing 1(PDZK1) protein as a mainstream mechanism of oestrogen in melasma, with heightened expression in the hyper pigmented skin of melasma patients11. Various studies examining hormonal profiles in melasma patients have also revealed significantly elevated luteinizing hormone levels and decreased serum oestradiol, indicating subtle signs of mild ovarian dysfunction. A noteworthy correlation has been noted between thyroid autoimmunity and melasma12.
UV radiation
The primary catalyst and exacerbating element in melasma, the UV component of sunlight, is stood as, leading to an elevation in melanosomes and focal melanocyte hyperplasia. Heightened melanogenic activity is directly triggered by UV radiation, resulting in the development of epidermal pigmentation, which is more pronounced in regions affected by melasma than in adjacent skin8, 9. Chiefly, melanogenesis is triggered by UVA and UVB radiations, while notably lower melanogenic potential is exhibited by infrared radiation and visible light. It is suggested by epidemiologic studies that some patients with melasma may be triggered or exacerbated by sun exposure alone or sun exposure during pregnancy 9, 12. The strong support of the role of UV radiation in the development of melasma by clinical evidence is indicated by the improvement shown by many patients during the winter compared to the summer. The levels of dermal stem cell factor and alpha melanocyte stimulating hormone in the skin are raised by UV radiation, which potentially accounts for the increased melanocytosis and melanogenesis, respectively11. By the binding of ?-MSH to its receptor, melanogenesis is stimulated10. The pathogenesis of melasma has been implicated with the increased proliferation of dermal vasculature and the upregulation of proangiogenic factors such as vascular endothelial growth factor (VEGF), basic fibroblast growth factor (bFGF), and interleukin (IL-8) induced by UV irradiation. The role of mast cells in the pathogenesis of melasma has been highlighted, with the ability of mast cells to induce vascular proliferation by secreting various dermal proangiogenic factors like VEGF, FGF-2, and TGF-B, thereby enhancing melanogenesis in melasma13.
Treatment

Fig. 4: Therapy phases
Kojic acid
The organic acid which is yielded from carbohydrate sources by variety of microorganisms in the presence of oxygen (aerobic process) 14. It is naturally obtained from fungal products of Trichocomaceae family mainly from the species of Penicillium and Aspergillus15. Kojic acid is mainly found in food and is ingested by human16. It is a skin-lightening ingredient, ultra violet filter and proven clinically to use in the patients suffering from hyper pigmentary disorder such as solar lentigines, melasma, freckles, and postinflammatory pigmentation17. Melasma and hyperpigmentation are caused by the aggregation of tyrosine and melanin in cells. Kojic acid in cosmetic industry is used as tyrosinase inhibitor hence used in managing melasma and hyperpigmentation which acts as skin lightning/depigmenting agent15, 17.
Liquorice
The liquorice plant (Glycyrrhiza glabra L,) also known as gancao, grandfather herb, is one of the main plant used in the Ayurvedic system of medicine for its amazing pharmacological activities which has been proven and reported. It is a plant that persists for several years, and is not a seasonal plant available in all the different seasons18. Liquorice consists of many active constituents and mainly roots of liquorice are used for their therapeutic efficacy some of which are flavonoids, liquirtigenin, isoliquiritigenin (ISL), liquiritin and glycyrrhizin (glycyrrhizic acid) 19. A constituent deriverd from the root extract of licorice (Glycyrrhiza glabra), glabridin has many remarkable effects on skin foremost inhibition of melanogenesis, glabridin effectively inhibits tyrosinase activity in melanoma cells by this it helps to regulate skin pigmentation and prevents excessive synthesis of melanin and also has anti-inflammatory activity20. Another liquorice derivative, Liquiritin, has demonstrated promise in treating melasma in a clinical investigation.
Azelaic acid
It has been reported that azelaic acid (AZA) constitutes naturally occurring straight-chain saturated dicarboxylic acid that competitively inhibits tyrosinase and melanin biosynthesis by direct interference21, 22. Beneficial effects in treating melasma have been documented with AZA cream, which when applied twice daily exhibits anti-proliferative properties and targets selective hyperactive melanocytes, inhibiting both tyrosinase and enzymes of mitochondrial oxidoreductase with minimal impact on normally pigmented skin3, 5. Various studies have demonstrated that AA treatment is either less effective or equally effective as HQ, making it a viable alternative for individuals intolerant to HQ13.
Hydroquinone
Among the various agents employed over time for treating melasma, hydroquinone (HQ) stands out as one of the most effective1. Hydroquinone (HQ; 1, 4-dihydroxybenzene) is a hydroxyphenol along with catalytic amounts of dopa, competes with tyrosine, the natural substrate of tyrosinase. This competivity inhibits the enzymatic oxidation of tyrosine to dopa, consequently halting the generation of melanin21, 22. HQ concentrations ranging from 2–4% are commonly used either alone or in combination creams. Concentrations exceeding 5% are not recommended due to their severe irritancy without improved efficacy5. Concentrations of 4% and 5% are highly effective but moderately to strongly irritant21. Some have also suggested that it may induce melanocyte destruction and melanosome degradation directly. Despite its high efficacy and availability in various concentrations, it may induce irritant dermatitis in certain individuals, and prolonged usage can result in exogenous ochronosis13.
Vitamin C and E
Vitamin E appears to complement Vitamin C's effects synergistically in this regard3. Alpha-tocopherol present in tissues, membranes, and plasma and the most prevalent vitamin E derivative in humans. It demonstrates photoshielding effects and induces toning through tyrosinase inhibition13. Ascorbic acid (vitamin C) along with two biologically active forms of vitamin E, (?-tocopherol and ?-tocopherol), are detected in the skin. Excess exposure to the UV light will lead to the depletion of these vitamins from the skin. Vitamins C, E, and carotene demonstrate antioxidant properties, aiding in the prevention of UVB- and UVA-induced phototoxic reactions23. However, the ability of this to reduce melanogenesis is comparatively less than that of HQ. The union of Vitamin C and Vitamin E significantly enhances the inhibition of melanogenesis compared to using Vitamin C alone10.
Corticosteroids
Corticosteroids have anti-inflammatory properties and can prevent pigmentation by non-selectively suppressing melanogenesis. When used as monotherapy, corticosteroids are unlikely to be more effective than depigmenting drugs. Based on available data, corticosteroids can decrease melanogenesis on their own, but they haven’t been shown to provide long term advantages in the treatment of melasma. In addition, stretch marks, hypopigmentation, acne, telangiectasias [spider veins], and epidermal atrophy might result from prolonged steroid use8. By reducing the melanocytes' overall secretory and metabolic activity, they prevent the creation of melanin without destroying the cells5.
Retinoids
Topical retinoids are also proven to be useful in the treatment of melasma, with keratinocyte turnover being suggested as the mechanism. A small sentinel research conducted in 1993 revealed that melasma pigmentation might be dramatically reduced by using 0.1% of tretinoin cream. Relevant research has validated the effectiveness of 0.1% tretinoin cream in treating melasma in persons with darker skin tones23. Initially used in conjunction with HQ to increase HQ’s penetration. Tretinoin's capacity to disrupt pigment transfer, disperse keratinocyte pigment granules, and speed up epidermal turnover24.
Tranexamic acid
Tranexamic acid (TA) is a lysine analog that’s been in use for more than 30 years now as an antifibrinolytic drug. By impeding plasminogen's attachment to keratinocytes, it suppresses plasmin activity induced by UV radiation in keratinocytes. This leads to a reduction in prostaglandin synthesis and free arachidonic acid, which in turn lowers melanocyte tyrosinase activity12.
Chemical Peel
Chemical peeling agents primarily work by eliminating melanin rather than inhibiting melanocytes or melanogenesis, making them generally well handled by subjects with lighter skin tones22. Dermatologists, however, are wary of using chemical peels on patients from darker racial/ethnic backgrounds since they may exacerbate melasma and cause post-inflammatory hyperpigmentation22, 10. Chemical exfoliation efficacy in treating melasma can vary, with some cases improving while others worsen due to post-inflammatory hyperpigmentation3, 5. Glycolic acid (GA) peels are widely favoured for treating melasma due to their perceived effectiveness, ease of administration, safety, minimal downtime, and low risk of scarring, hyperpigmentation, or persistent erythema, while salicylic acid being a safer alternative for individuals with sensitive or darker skin22, 10. Recent investigations have explored combination peel treatments. A study found that a blend of 20% and 10% salicylic acid and mandelic acid respectively was as effective as 35% GA for Fitzpatrick skin types IV and V patients. Common adverse reactions across all peel types include persistent post-peel erythema and the potential for infection8, 22.
Laser Therapy
The rationale behind utilizing lasers to address pigmentary disorders is rooted in the concept of selective photothermolysis, where specific light wavelengths emitted by lasers are absorbed by particular cell or tissue types. Over time, a variety of laser treatments have been explored for melasma, yielding mixed outcomes22. The use of laser therapy for melasma is thought to be a promising replacement for conventional techniques. While the topic is still in debate, it's crucial to evaluate its current supremacy. Laser therapy work on by disorganising the melanin granules in the overlying dermis, which is then engulfed by macrophages23. With differing degrees of effectiveness, laser therapy has been examined recently as a therapeutic option for melasma. This is because lasers use thermal energy to target specific chromophores in the skin. Because non-ablative lasers are less likely to induce inflammation and, consequently, less post-inflammatory pigment alteration (PIPA), they are being considered as a potential treatment for melasma8. Due to potential adverse effects such as hyperpigmentation, mild scarring, and atrophy associated with laser treatment, the role of lasers in treating melasma remains uncertain10. Various lasers utilized for treating melasma are as follows: Fractional photothermolysis (FP) has been applied to melasma treatment, employing fractional lasers for pigmented lesions, including melasma. Q-Switched Nd: YAG stands out as the most frequently employed laser for melasma treatment. The duration of treatment ranges from 5 to 10 sessions with a week’s interval12.

Fig.5 Laser removal melasma
Classification of Cream
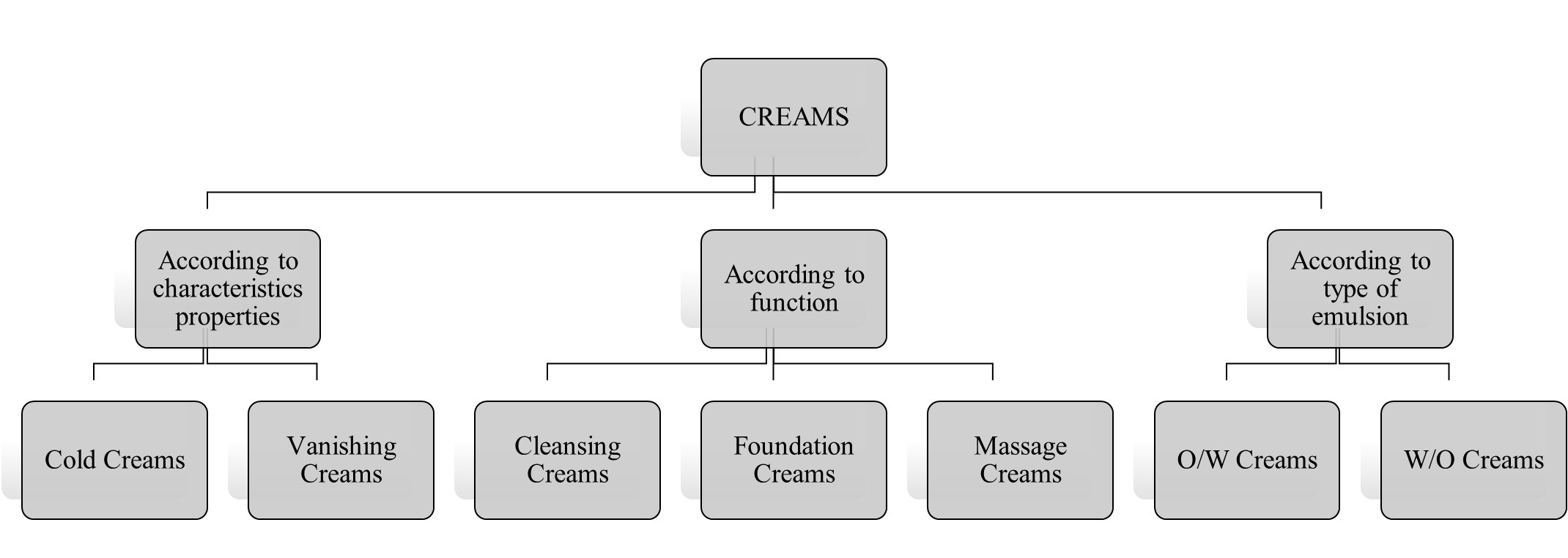
Fig.6: Types of cream
Evaluation of cream
The cream colour, scent and appearance were assessed for its organoleptic characteristics6.
The spreadability of cream is assessed using glass slide apparatus24. Where an excess amount of cream is sandwiched between two slides, and a pressure is applied to the slide for 5 minutes to condense the sample to a homogenous thickness25. The period taken for the two slides to separate is then measured in seconds as a measure of spreadability26. A shorter separation time indicates better spreadability27. This process is described by the formula,
S = w*l / t,
Where,
S represents spreadability in g cm/sec,
w denotes the weight on the top slide in grams,
l indicates the length of the slide in cm, and
t signifies the duration taken in seconds28.
The effectiveness of the formulation depends on how well it spreads when applied to the affected areas of the skin29.
An area of 1 sq. cm was marked on back of the left-hand side, where the cream was put on and application was recorded61. Irritation, erythema, and edema to be monitored periodically for 24hours, and any observations were recorded29.
Homogeneity was assessed through visual inspection to evaluate appearance and to detect any potential clogs27.
The cream is mixed with scarlet red dye for the test6. A droplet of the mixture is studied under a microscope after being placed on a tiny glass slide, covered with a cover slip24. If red disperse droplets are seen against a colourless background, it indicates an O/W type cream. Conversely, in W/O type cream, the dispersed particles appear colourless28.
Reflux 2 grams of the substance with 25 ml of 0.5 N alcoholic potassium hydroxide for duration of 30 minutes27. Next, 1ml of phenolphthalein is introduced, and it is promptly titrated with 0.5 N HCl28. Record the volume as 'a'. The process is then repeated without the substance, and the volume is noted as 'b'26. The saponification value can be calculated using the formula:
(b - a) * 28.05 / w,
Where,
‘w’ represents the weight of the substance in grams.
‘a’ represents the volume of titre in ml
‘b’ represents volume of blank in ml
Dissolve 10 grams of the substance in a precisely measured 50 ml of alcoholic mixture and solvent ether26. Set up the flask to a reflux condenser and gently heat until the sample is fully dissolved. Then, add 1 ml of phenolphthalein and titrate with 0.1N NaOH until a faint pink colour appears upon agitation for 30 seconds27. The acid value can be calculated using the formula:
Acid value = n * 5.61 / w,
Where,
‘n’ represents the volume of 0.1N NaOH used
‘w’ is the weight of the substance29.
The manageability of the creams was evaluated by cleansing the treated area with tap water. The effectiveness of the formulation is dependent on how well it spreads when applied to the affected areas of the skin. Additionally, when the cream is applied to the skin, it is completely absorbed and provides a cooling effect. It can be easily washed off in water without requiring rubbing31.
Uniform viscosity in creams is crucial for maintaining quality throughout the manufacturing process, according to the Non-Newtonian nature, viscosity should remain constant over their shelf life. Tools such as the Brookfield viscometer or Ford viscosity cup are employed to measure viscosity, and if it shows high viscosity, adjustments like incorporating additional fatty materials or emulsifiers can be made to correct it6, 25.
Agar media is first prepared, followed by inoculating agar plates using the steak plate method with the formulated cream, while a control is prepared without the cream. Subsequently, the plates are incubated for twenty-four hours at 37°C. Following the incubation period, the plates are removed, and the microbial propagation is examined and compared with the control24, 31.
CONCLUSION
The resolute dysfunction of the epidermal-melanin unit with the disarray of the melanogenesis, results in the recurring pigmentation on the skin leading to the formation of untidy patches of melasma. Thus, managing of melasma can indeed be a challenging task and demands prolonged treatment over a period of time with topical agents. While the skin being one of the sensitive and the most accessible part of the body, that can get significantly vulnerable to allergies and injuries. In cases where topical agents are used, they may develop few adverse effects on the skin surface, often making the outcome unsatisfactory; although hydroquinone remains the highest standard of topical treatment for melasma. But hydroquinone, retinoic acid, and corticosteroids in triple combination are recommended as the first-line topical treatment for this pigmentary disorder. Along with these agents manier topical agents are newly developed which are potentially compatible, individually as well as in combinations, that are prescribed for the inhibition of the distorted melanogenesis and the same are opted in the successive therapy in the management of melasma. Several experimental studies are on process despite the lack of evidences for their safety and efficiency. Their prospective role in the management of melasma has been suggested by in-vivo and in-vitro experimental setups, but the majority of controlled clinical studies are deficient and will be desperately needed in the future.
REFERENCE

Adithi P., Monika N., Nasiba N. K., Nidhishree S., Nikshep N. S., P. Jeevitha., A Comprehensive Review On History, Pathogenesis, And Treatment Innovations For Melasma, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 8, 2359-2370. https://doi.org/10.5281/zenodo.13150683
 10.5281/zenodo.13150683
10.5281/zenodo.13150683