Priyadarshini J. L College of Pharmacy, Nagpur, Maharashtra, India 440016
Natural binders play a crucial role in tablet formulation by imparting cohesiveness, mechanical strength, and modulating drug release behavior. Growing concerns regarding the cost, environmental impact, and safety of synthetic binders have increased interest in plant-derived polymers as sustainable alternatives. Among these, okra gum obtained from Abelmoschus esculentus has shown promising binding efficiency and release-modifying properties. Studies indicate that natural binders improve granule flow, compressibility, tablet hardness, and drug release profiles in both conventional and modified-release systems. However, challenges such as batch-to-batch variability, microbial contamination, and stability issues require proper standardization and quality control. Overall, natural binders, including okra gum, represent a biodegradable, cost-effective, and eco-friendly approach for sustainable tablet formulation in modern pharmaceutics.
In pharmaceutical tablet formulations, binders are essential excipients that serve mainly to give powders cohesion and guarantee the creation of mechanically robust compacts during the tableting process. A material's compressibility, hardness, and disintegration behavior are all directly impacted by its binding strength. Stronger binders usually produce more durable tablets, but they may also take longer to disintegrate, which could have an impact on the kinetics of drug release. The efficacy of polymeric binders during granulation is also greatly influenced by their film-forming and adhesive qualities, which eventually affect the quality of the tablets.1
Because of their portability and convenience, tablets are the most commonly prescribed dosage forms globally. Pharmaceutical binders, sometimes called adhesives, are a key category of excipients utilized to enhance tablet formulations.2
One kind of excipient that is added to a tablet formulation to improve its mechanical characteristics and release profile by inter-particle bonding is called a binder. They may be semisynthetic, synthetic, or natural. Pharmaceutical binders that are synthetic or semi-synthetic are costly, scarce, and nonrenewable. According to research, these artificial additives are dangerous for the environment as well as for humans.3
Gastroretentive Drug Delivery System
The primary strategy of stomach targeting is to prolong the gastric residence time of the formulations. The strategy is suitable for drugs that are mainly absorbed or work in the stomach or upper GIT, or for drugs that are not stable in intestinal alkaline conditions. 4 The gastroretentive delivery systems can also be used for sustained or controlled drug release, which is beneficial for reducing the fluctuations of systemic drug concentrations, decreasing the frequency of administration and increase patient compliance to drugs.5 Although a large number of gastroretentive formulations were studied, there is little progress on the clinical translation. The most frequently used gastric retention preparations are gastric floating, gastric expandable, and mucoadhesive and high-density formulations.
Local Targeting to GIT
Based on the physiological characteristics of different GIT sites, oral drug delivery systems are commonly used to deliver drugs specifically targeting the GIT. The main local targeting delivery strategies are summarized in Figure no.1
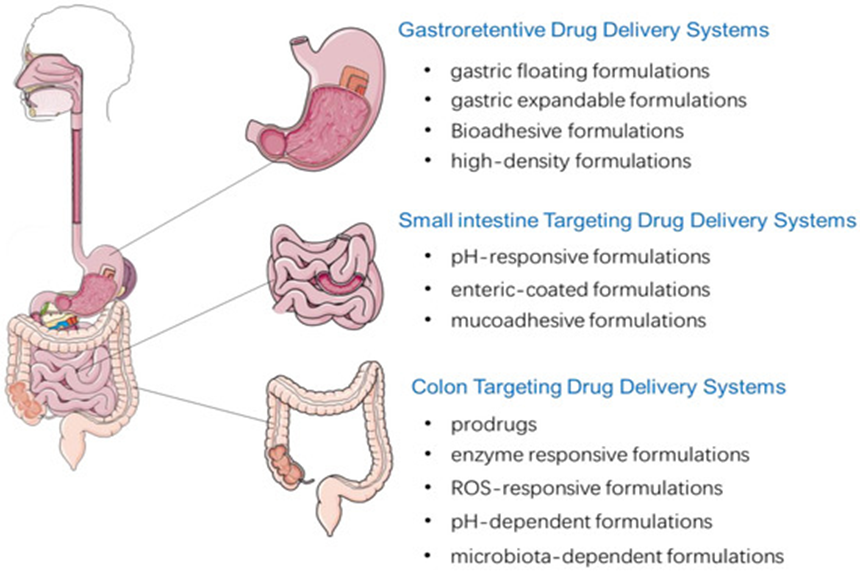
Figure no.01:- Local targeting drug delivery systems to GIT after oral administration.6
Oral medication is the most common form of drug administration because of advantages such as convenience of drug administration via the oral route, patient preference, cost-effectiveness, and ease of large-scale manufacturing of oral dosage forms. Around 60% of established small-molecule drug products available commercially are administered via the oral route. Current estimates indicate that oral formulations represent about 90% of the global market share of all pharmaceutical formulations intended for human use. Around 84% of the best-selling pharmaceutical products are orally administered and are currently valued at $35 billion, with an annual growth rate of 10%.7
The compliance of patients to oral formulations is generally higher than that to other parenteral routes such as intravenous, subcutaneous, and intramuscular injections, as well as to inhalation for asthma medications. Furthermore, orally administered drugs can be targeted to particular regionswithin the gastrointestinal (GI) tract for localized treatment of pathological conditions such as stomach and colorectal cancers, infections, inflammations, bowel diseases, gastro-duodenal ulcers, and gastroesophageal reflux disorders.8 Despite these advantages, the development of oral formulations presents several challenges, which are mainly attributed to the physicochemical properties of drugs, including poor water solubility and membrane permeability. In addition, the absorption of drugs can be limited by their poor chemical and biological stability, as well as by physiological barriers, including pH, efflux transporters, and metabolic enzymes. Further, some drugs can cause local irritation and nausea.9
Over the last four decades, numerous studies have focused on understanding the mechanism of drug absorption and transport, intestinal transit, microenvironment of the GI tract, and drug stability in the GI fluids.10 Thus, the elaboration of oral drug delivery systems necessitates a thorough understanding of the physicochemical properties, GI permeability, biological barriers, pharmacokinetics, and pharmacodynamics of drugs.11
Tablet
The Indian Pharmacopoeia defines pharmaceutical tablets as solid, flat, or biconvex dishes that are used as unit dose forms. They are made by compressing a medication or a combination of medications, either with or without diluents. A compacted solid dosage form that contains medications, either with or without excipients, is called a tablet. Depending on the quantity of therapeutic ingredients and the intended manner of administration, they fluctuate significantly in size, weight, and shape.12
The tablet is the most commonly used dosage form among all available options due to its ease of administration, lower production costs, and elegance.13 The aesthetic attributes such as color, texture, mouthfeel, and taste masking are determined by coating techniques. This coating technology has certain limitations or drawbacks, and to address these limitations. Tablet is one of the best alternatives. The present work aims to comprehensively review the formulation, characterization, and challenges in the development of Tablet in Tablet dosage form.
The principal benefit of tablets as a dosage form is that they offer a precise medication dosage. Every tablet has to have an established quantity of medication and has to be consistent in diameter, appearance, and weight. Orally administered tablets, once ingested whole, ought to easily break down in the stomach. This characteristic embodies a significant formulation paradox: tablets must be strong enough to endure the challenges of coating and packaging processes, yet they should also be able to release the drug quickly. The breakdown of the compact occurs due to aqueous fluids infiltrating the tablet's time-residual pore structure, causing it to burst apart.14
Properties15
Advantages16
Disadvantages17,18
Various Types of Tablet19
Various types of tablets are being developed and used recently Table 1 describes the various types of tablets used now days.
Table 1: Different Type of Tablets
|
Oral Tablets for Ingestions |
|
|
Tablets for Oral Cavity |
|
|
Tablets Administered by Others Routes |
|
|
Tablets for Solution Preparation |
|
Various Novel/Advanced Types of Tablet Drug Delivery System:
Now a day’s various kinds of advanced tablets were developed and used according to Table 2.
Table 2: Different Types of Novel Tablet Drug Delivery Systems
|
Sr no. |
Types of Tablet |
|
1 |
Oral extended release tablets |
|
2 |
Osmotic pressure controlled tablets |
|
3 |
Multi-layered tablets formulations |
|
4 |
Gastroretentive buoyant drug delivery system |
|
5 |
Mucoadhesive drug delivery systems |
|
6 |
Targeted drug delivery system |
|
7 |
Colon specific drug delivery |
|
8 |
Miscellaneous |
|
9 |
Vaginal tablets |
|
10 |
Ion exchange resin system |
|
11 |
Rapid disintegrating tablet |
Excipients
Excipients are additive substances incorporated into tablet formulations to enhance the bulkiness, disintegration, dissolution rate, and bioavailability of the drug. The interaction study of the drug and excipient is conducted using Infrared Spectrum to determine the stability of both the excipients and the drug.20
Common excipients used in tablets 21,22
Diluents:-
Binders, granulating agents, compression aids:-
Disintegrants:-
Glidants :-
Lubricants:-
Tablet coatings and films:-
Colouring agents:-
Flavoring Agents:-
Absorbents:-
Techniques for Making Tablets
1) Direct compression:-
Medicinal Without a doubt, the most straightforward method for tablet production is direct compression (DC). It is sufficient for the active ingredient to be correctly mixed with suitable excipients prior to compression, according to DC. In addition to the ease of formulation and production, direct compression offers significant benefits such as lower capital, labor, and energy expenses for manufacturing, as well as the elimination of water use for granulation with drug substances that are sensitive to moisture.23
Applicability of direct compression
Whether DC applies to a particular drug substance is primarily determined by dose. The three essential elements for effective tableting are the flow and compactability of the compression mix, as well as ensuring uniform drug content in both the mix and the finished tablets. It is probable that all of these factors will be influenced by the amount of drug administered. A low dose of around 10 mg or less, a medium dose of approximately 10 mg to 50 mg, and a high dose of about 50 mg are chosen. In the case of low-dose pharmaceuticals, the excipients play a major role in determining flow and compaction of the compression mix. The main objective is to ensure satisfactory content uniformity both in the blend and in the tablets. For drugs with medium doses, the flow of the compression mix may be crucial, while for drugs with high doses, both flow and compaction rely heavily on the characteristics of the drug substance. It is estimated that direct compression as a manufacturing technique accounts for up to 50% of formulations in the United States.24
2) Wet granulation
The most common method for agglomerating or granulating in pharmaceutical powder blends involves the use of a granulating liquid, followed by wet sizing and drying. the sector is wet granulation. The wet granulation process consists of three main steps: the powder blend is wet massed with a granulating liquid, then sized by weight, and finally dried.25
Important steps involved in the wet granulation26
Limitation of wet granulation27
3) Sintering Method
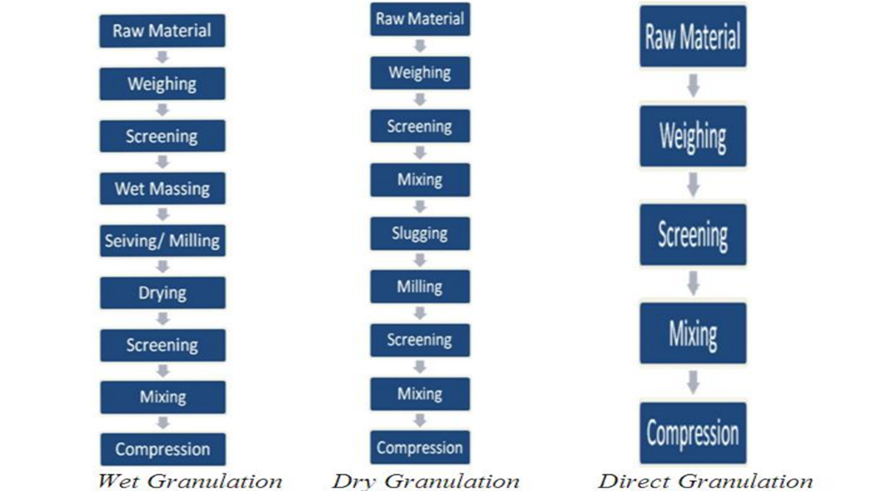
Fig no. 02:- Processing Steps in Wet Granulation, Dry Granulation and Direct Granulation29
During precompression, tablets are partially formed and the precompression roller is smaller than the compression roller, resulting in a lower applied force. A machine that provides multistage compression with high precompression and an optimal main compression force achieves the best compression efficiency. For items that experience brittle fracture, implementing precompression with a force greater than that of main compression leads to increased tablet hardness.
It is reported that using rollers for precompression and for the main compression that are of similar dimensions, so as to apply forces that are also similar, leads to optimal tablet formation.30
2) Main Compression:-
In the course of main compression, the energy applied is converted into the creation of interparticulate bonds. Upon the application of a force within a die, the particles initially rearrange themselves to create a structure with reduced porosity when subjected to very low forces. Subsequently, the particles attain a condition in which any additional relative movement is precluded; thus, an increase in the force applied results in fragmentation and/or deformation of the particles.31
3) Decompression:-
Once the applied force is taken away, a set of stresses arises within the tablet due to elastic recovery. The tablet needs to possess sufficient mechanical strength to accommodate these stresses; otherwise, failure of its structure may happen. If elastic recovery is pronounced and rapid, capping or laminating of the tablet may occur. During decompression, if the tablet experiences brittle fracture, it can lead to the formation of failure planes as surfaces fracture. Tablets that do not cap or laminate can relieve stresses through plastic deformation.32
4) Ejection:-
In the compression cycle, the final step is ejection from the die. The ejection phase necessitates a force to overcome the adhesion between the die wall and the compact surface, as well as additional forces to finalize the tablet's ejection.
The force required for the ejection of a tablet is the unique peak force needed to begin the process of ejection by disrupting the adhesion between die wall and tablet. The second stage consists of the force needed to push the tablet up against the die wall, while the final force is necessary for ejection. When lubrication is insufficient, variations in this process can occur due to a slip-stick condition between the tablets and dies wall. This results in ongoing formation and breakage of tablet die–wall adhesion. Lubricants reduce stress patterns, thereby decreasing the likelihood of materials capping or laminating. 33
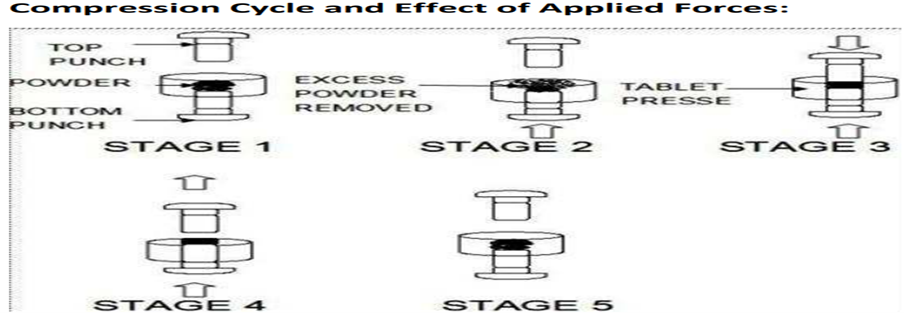
Fig no. 03:- Compression cycle and Effect of Applied forces
Validation of Tablet
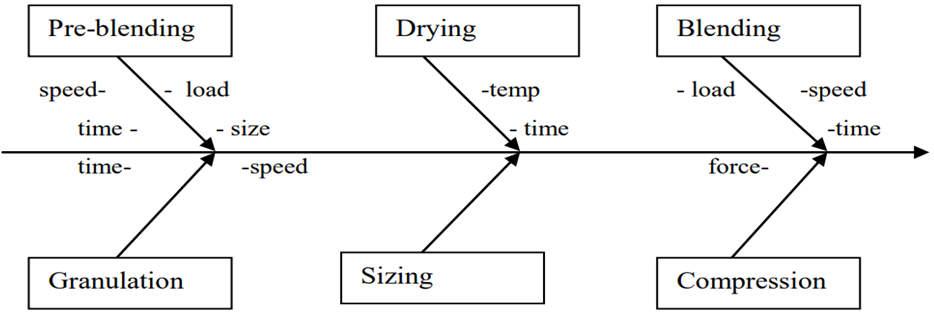
Fig no. 04:- Process flow diagram for process validation of tablet.34
Types of Tablets35,36
These tablets are created through compression and do not have any special coating. They are created from powdered, crystalline, or granular substances, either individually or in conjunction with a binder, disintegrates, controlled release polymer, lubricant, and diluents, and often include colorant.
Compressed tablets with a sugar coating are known as sugar-coated tablets.This coating can be colored and useful for concealing drug substances that have an unpleasant taste or smell, as well as for safeguarding materials that are prone to oxidation.
These tablets are compressed and coated with a delicate film made of water-soluble material. Several substances that have the ability to form a film are employed.
These are compressed tablets coated with a substance that withstands gastric fluid but disintegrates in the intestine. Enteric coating can be applied to tablets containing medicinal substances that are inactivated or destroyed in the stomach, those that irritate the mucosa, or those intended for delayed release of medication.
These are compressed tablets made by more than one compression cycle; Layered tablets, Pressed -coated tablets.
It is possible to create compressed tablets that release the medication gradually over an extended duration. Therefore, this dosage form is also known as a sustained-release and prolonged-release dosage form.
Tablets that are compressed and intended for use in preparing a solution or adding a specified characteristic to a solution must have labels indicating that they should not be ingested.
These tablets offer a user-friendly amount of strong medication that can be easily mixed into liquids and powders, eliminating the need for weighing out small amounts.
Immediate release tablets are designed to disintegrate and dissolve quickly, thereby releasing the medications. An appropriate pharmaceutically acceptable diluent or carrier may allow for immediate release, as long as it does not significantly extend the drug's release and/or absorption rates.
These tablets are small, flat, and oval-shaped. Tablets designed for buccal administration by placing them in the buccal pouch may dissolve or erode slowly, so they are formulated and compressed with enough pressure to create a hard tablet.
Problems with Existing Oral Dosage Form 37
Natural binders:-
Excipients are additives used to transform active medicinal substances into a pharmaceutical dosage form appropriate for patient administration.38 An essential part of tablet composition is the binder. It is utilized to create a cohesive bond between active pharmaceutical ingredients (API) and inactive substances (other excipients). In order to give flexibility and strengthen the inter-particulate bonding, binders are added to the tablet formulation.39 Correspondingly, binding agents in tablet formulations results in attaining specific tablet mechanical strength and drug release characteristics.40
To accomplish various pharmaceutical goals, different binders have varying mechanical strengths and drug release characteristics. A thorough understanding of binder qualities for improving strength and the interaction between different material constituents should be taken into account while making the tablet. For this reason, there is ongoing interest in developing novel excipients for use as tablet binders. In tablet formulation, a variety of natural and synthetic polymers are employed as binders. Because of their low cost, low toxicity, biocompatibility, and environmentally acceptable manufacturing, natural binders like starch, gums, and mucilage are commonly utilized.41
Gums can be categorized as natural, semi-synthetic, modified, or synthetic due to their hydrophilic nature. Acacia, ghatti, karaya, locust bean, albizia, khaya, guar, tragacanth, and xanthan are among the gums that are extracted or exuded from the bark of different plants' stems, branches, and roots. The plant groups Anacardiaceae, Combritaceae, Meliaceae, Rosaceae, and Rutaceae are renowned for producing gums. There are several explanations for why plants produce gums, such as as byproducts of regular plant metabolism.42 In order to give the tablet formulation flexibility and strengthen the interparticulate bonding, binders are added.43
Gums are often polysaccharides, which are naturally occurring polymeric substances derived from both woody and nonwoody plant parts, including bark, seeds, sap, roots, rhizomes, fruit, leaves, and plant gums. These substances are frequently utilized in the creation of pharmacological dosage forms. Gum is mostly used as a binding agent in tablet.44
The efficiency of natural gum and mucilage as a binder in tablet formulation was the focus of the current study.45 Binders are the agents which hold various powders together to form a tablet. They impart cohesiveness to the granules to improve compression and flow properties which derived the hardness of tablet.46 To accomplish various pharmaceutical goals, different binders have varying mechanical strengths and drug release characteristics. A thorough understanding of binder qualities for improving strength and the interaction between different material constituents should be taken into account while making the tablet.47
For this reason, there is ongoing interest in developing novel excipients for use as tablet binders. Tablet formulation uses a variety of polymers, both natural and synthetic, as binders. Because of their low cost, low toxicity, biocompatibility, and environmentally acceptable manufacturing, natural binders like starch, gums, and mucilage are commonly utilized.48 Although batch-to-batch variability and other restrictions have prompted innovations like chemically modified or co-processed binders for better consistency, natural binders enable sustainable tablet formulation due to their renewable sources.49
Advantages of Natural Gums in pharmaceutical science50
Disadvantages of Natural Gums in pharmaceutical science51,52
Binder types
1] Resource-based classification53
Examples of natural binders include carboxy methyl cellulose, ethyl cellulose, and methyl cellulose.
2] Source -based classification54
3] Shaped- based classification
4] Charge-based classification55
CATEGORIZATION BASED ON THEIR USE56
OKRA GUM
Okra gum is among these types of gums and has seen a rise in popularity in the pharmaceutical industry over the past few decades. It has been demonstrated to be a promising excipient for modifying drug release from tablets of various APIs in solid dosage forms.57 Okra gum serves as an emulsifying agent and stabilizer in liquid dosage forms, specifically in emulsions, and acts as a suspending agent in pediatric suspensions.58 Okra gum has been utilized in nasal drug delivery systems due to its gel-forming properties and mucoadhesive characteristics.59 Earlier studies have compared the binding ability of okra gum with that of PVP, cornstarch , and gelatin and have shown that okra gum is a better binder than these routinely used binders. However, there is no study signifying the binding strength of okra gum in quantitative terms.60
In this study, the binding strength of okra gum was assessed using two different methods based on the principle that two surfaces, initially bonded by applying adhesive material between them, are separated by applying a load. Furthermore, the binding efficacy of okra gum was illustrated through an analysis of the properties of granules and tablets produced via wet granulation with a model drug and varying concentrations of okra gum serving as a binder. The studied characteristics include the bulk properties of granules and the tablet’s hardness, friability, disintegration time, and drug release patterns. The results were compared to those of tablets made with a traditional binder, specifically pre-gelatinized starch, which is widely used in the pharmaceutical industry.61
Preparation of the Aqueous Extract of Okra
Okra gum was obtained from the fresh pods of Abelmoschus esculentus using a previously described extraction method from the literature.62 To achieve this, okra pods (approximately 0.25 kg) were cleaned, dried at ambient conditions (about 25 °C), and cut into small pieces of roughly 1 inch in length after taking off the calyces. These slices (with a weight of 0.10 kg) were placed in a pan, ~1.5 L of distilled water was added, and they were heated at ~60 °C for 4 hours with occasional stirring. A muslin cloth was used to filter the mixture, and the resulting aqueous extract was refrigerated at 4–6 °C.63
Isolation of okra gum
The gum okra was precipitated from the aqueous extract by adding three portions of acetone (~250 mL each) and filtering the resulting precipitates with filter paper after each addition. The precipitate was placed in an oven at approximately 40 °C until it reached a constant weight. The dried gum was ground using a pestle and mortar, sieved through a mesh of number 20, and kept in an air-tight glass container at room temperature until it was needed again.64
Methods
Extraction of mucilage from the pods of okra fruit
The pods of okra fruits were used to extract okra gum. The fruits were cleaned, washed, sliced, crushed, and macerated in distilled water for 10 hours with intermittent stirring. The mucilage was passed through a white muslin cloth to extract the gum, and acetone was added to precipitate the extracted gum. The gum was subsequently filtered under vacuum to eliminate acetone and was dried in a desiccator.65 The specific gravity, pH, water content, total ash content, acid insoluble ash, water soluble ash, and microbial limit of Okra gum binder were measured according to the recommendations of the U.S. pharmacopoeia.66
Evaluation of Powder Blend
The prepared mixture is assessed using the following tests.
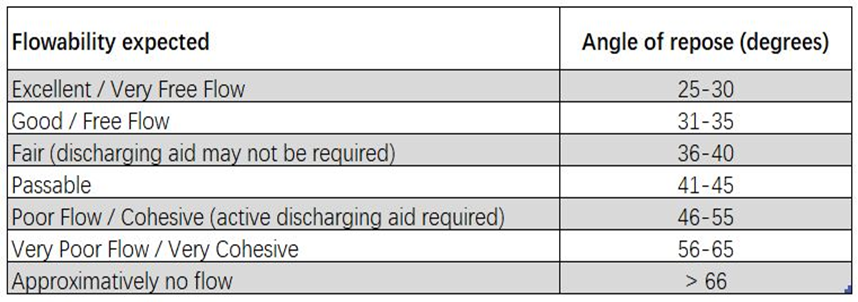
The funnel method was used to measure the angle of repose. A funnel was used to hold the blend, which had been weighed with precision. The funnel was adjusted to a height where its tip just made contact with the top of the pile of blend. The blend of drug (as solid dispersion) and excipient was allowed to flow freely through the funnel onto the surface. The diameter of the powder cone was measured, and the angle of repose was computed using the following formula
Tan θ = h/r
Angle of repose (θ) = tan-1 (h/r)
Where,
h = height of the powder pile
r = radius of pile circle
Weigh out granules (M) 25g that have been passed through a #20 sieve and place them in a 100ml graduated cylinder. Without compressing, level the powder with care and take note of the apparent volume (V0) Compute the apparent bulk density in gm/ml using the formula below: Bulk density (BD) is calculated as M/Vo
Bulk density = M/Vo
Where,
M = mass of powder taken,
Vo = apparent unstirred volume.
Weigh (M) 25g of granules, which have been passed through a #20 sieve, with precision and transfer them into a 100ml graduated cylinder. Then, using a mechanically tapped density tester that produces a fixed drop of 14±2mm at a nominal rate of 300 drops per minute, raise the cylinder containing the sample and let it fall under its own weight to tap it mechanically. Initially, tap the cylinder 500 times and measure the tapped volume (V1) to the nearest graduated unit. Then, repeat the tapping for an additional 750 times and measure the tapped volume (V2) to the nearest graduated unit. If the difference between the two volumes is under 2%, then volume (V2) is considered the final volume. Determine the tapped density in gm/ml using the following formula
Tapped density (TD) = M/VT
Where, VT = Tapped volume or final volume
In the field of pharmaceutics, the Carr index is often employed as a measure of a powder's flowability. A Carr index above 25 suggests poor flowability, while a value below 15 indicates good flowability. The Carr index indicates how compressible a powder is The percentage compressibility of the powder mixture was calculated using the following formula, which takes into account the apparent bulk density and tapped density
It is determined by formula
Car`s index (%) =
Tapped density - Bulk density × 100
Tapped Density
|
Carr’s index (as %) |
Flow Type |
|
5 -15 |
Excellent |
|
12 -16 |
Good |
|
18 - 21 |
Fair to passable |
|
23 - 35 |
poor |
|
33 - 38 |
Very poor |
|
40 |
Extremely poor |
By using following formula, the Hausners ratio can be calculated. This serves as an indirect indicator of how easy it is to measure powder flow. A Hausner ratio of less than 1.25 indicates better flow properties than one greater than 1.25.
|
Flow character |
Hausner ratio |
|
1.00 -1.11 |
Excellent |
|
1.12 -1.11 |
Good |
|
1.19-1.25 |
Fair |
|
1.26-1.34 |
Passable |
|
1.35-1.45 |
Poor |
|
1.46-1.59 |
Very Poor |
Future Aspects71
Natural binders offer significant opportunities for advancement in modern pharmaceutics. Future research and development may focus on the following areas:
CONCLUSION
Natural binders have emerged as promising alternatives to synthetic and semi-synthetic excipients in tablet formulation due to their biodegradability, biocompatibility, low toxicity, cost-effectiveness, and renewable origin. Their ability to impart adequate cohesiveness, mechanical strength, and desirable drug release characteristics makes them suitable for both conventional and modified-release tablet systems. Extensive research demonstrates that plant-derived gums, mucilages, and polysaccharides can effectively improve granule flow properties, compressibility, hardness, and overall tablet performance. In addition, natural binders contribute to sustainable pharmaceutical development by reducing environmental impact and dependence on non-renewable resources. However, challenges such as batch-to-batch variability, microbial contamination, uncontrolled hydration behavior, and viscosity changes during storage must be carefully addressed through proper standardization, processing, and quality control measures. Overall, natural binders represent a viable and sustainable approach in modern pharmaceutics, offering significant potential for the development of safe, effective, and eco-friendly tablet dosage forms.
REFERENCES

Trupti Nimburkar, Dr. Rahul Kasliwal, Dr. Yogesh Gholse, Dr. Dinesh Chaple, Sanket Chore, Tanaya Vairagade, Vidhi Sonbirse, Natural Gums as Pharmaceutical Binders: Current Perspectives and Future Opportunities, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 4224-4244. https://doi.org/10.5281/zenodo.19363465
 10.5281/zenodo.19363465
10.5281/zenodo.19363465
