
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, Srinivas College of Pharmacy, Valachil, Farangipete, Mangalore – 574143, Karnataka, India
Self-microemulsifying drug delivery systems (SMEDDS) have become a strong method for using lipids to help drugs that are not very soluble in water and have low absorption when taken by mouth, especially for drugs classified as BCS class II and IV. These systems are mixtures of oils, surfactants, and co-surfactants that mix evenly and form tiny oil-in-water droplets when gently stirred in the stomach and intestinal fluids. This helps keep the drug dissolved and makes it easier for the body to absorb. Although SMEDDS have many benefits in terms of drug delivery, traditional liquid forms of SMEDDS (L-SMEDDS) have issues like not staying stable, leaking, being hard to handle, and not being easy to make into solid tablets. To fix these problems, a lot of research has been done to create solid SMEDDS (S-SMEDDS), which combine the ability of lipid-based systems to dissolve drugs with the benefits of solid oral medicines, such as being stable, easy to use, and more acceptable to patients. This review gives a detailed look at SMEDDS, covering the basics of how they are made, how they form micro-emulsions on their own, choosing the right ingredients, and strategies for designing the formulations. Important ways to test these systems are also covered, including measuring the size of the droplets, how charged they are, how they dissolve in water, and how they behave in solid form. The review also mentions current challenges in making these systems stable, scaling up production, and meeting regulatory standards.
Self-emulsifying drug delivery systems (SEDDS) have become an important method to tackle the ongoing issue of low oral bioavailability in poorly water-soluble drugs. This is especially true for drugs classified in Biopharmaceutics Classification System (BCS) classes II and IV, where dissolution is more of a problem than permeability1. The increasing number of highly lipophilic new chemical entities from modern drug discovery has raised the demand for formulation methods that can improve solubility. These methods must also keep drugs dissolved during their journey through the gastrointestinal tract2. Traditional techniques, such as micronization, salt formation, solid dispersions, and complexation, often offer only partial or unstable improvements. They can also be limited by scalability and the types of excipients that can be used. This has led to a greater interest in lipid-based systems3. SMEDDS are mixtures of oils, surfactants, and co-solvents or co-surfactants. They form fine oil-in-water emulsions when gently agitated in gastrointestinal fluids, mimicking gastric and intestinal movement4. By presenting the drug in a pre-dissolved state and creating micro- or nano-sized droplets (SMEDDS and SNEDDS, respectively), these systems improve the surface area for absorption. They maintain drug supersaturation and can promote lymphatic transport, allowing the drug to bypass the hepatic first-pass metabolism, which increases systemic exposure5. Mechanistic studies suggest that the movement of the drug between emulsion droplets and the aqueous phase, rather than just better solubility, leads to the improved absorption seen with SMEDDS6.Despite their proven ability to improve solubility and bioavailability for various small molecules and some peptides, conventional liquid SMEDDS (L-SMEDDS) have significant drawbacks. These include leakage, physical instability, incompatibility with standard solid dosage manufacturing, and the risk of drug precipitation during storage or after dilution7. These issues have led to extensive research into solid self-microemulsifying systems (S-SMEDDS). In these systems, liquid formulations are held on or within solid carriers using methods like adsorption, spray drying, hot-melt extrusion, and 3D printing8. The goal of solidification is to merge the biopharmaceutical benefits of SMEDDS with the stability, ease of handling, dose uniformity, and patient acceptance of traditional solid oral dosage forms. This process also allows for added features such as controlled release, mucoadhesion, and targeted delivery9.This review looks at self-emulsifying drug delivery systems, focusing on the change from liquid to solid SEDDS, SMEDDS, and SNEDDS. It summarizes the key principles of formulation, the choice of excipients, and how to improve bioavailability. It also discusses solidification materials and technologies. Finally, it highlights current applications, challenges, and future trends in creating effective self-emulsifying systems for poorly water-soluble drugs10.
Advantages of SMEDDS11:
When SMEDDS disperse in water, they form small droplets with a large surface area. This helps the drug move from the oil part into the water part easily, which is not possible with regular oily mixtures of drugs that don't dissolve well in water.SMEDDS are more stable than regular emulsions because they require less energy to produce. The process is simpler, using basic mixing tools, and takes less time than making emulsions.Drugs that dissolve slowly in water can be absorbed better with SMEDDS. This keeps the amount of the drug in the blood steady, which helps maintain a consistent level in the body. This happens because the drug is already in a dissolved form, so it doesn’t need to dissolve again.Drugs that break down in the stomach or intestines can be protected by SMEDDS because the drug is delivered in oil droplets, which help keep it safe.Using a pre-concentrated microemulsion in liquid-filled soft gelatin capsules is better than using a regular microemulsion.SMEDDS are preferred over self-emulsifying drug delivery systems (SEDDS) because they don’t need as much bile salt to form droplets, which may help the drug be absorbed better.SMEDDS make it easier to adjust the drug dose by simply changing the mix of ingredients, allowing for more personalized treatment options.
Disadvantages of SMEDDS12:
There are some issues with this system:
Drug precipitation when diluted: When SMEDDS mix with the fluids in the stomach or intestines, they can cause the drug to form solid particles. The drug's solubility is reduced, which also minimizes the advantages of a lipid-based system.Water-based solvents can increase the likelihood of solidifying drugs if they are mixed with water. To prevent this, special substances called polymers are needed in the body.Encapsulation in soft gelatin capsule: Most marketed SMEDDS come in soft gelatin capsules, which can be costly to produce and may have stability issues. They can also conflict with dietary or religious restrictions, and volatile solvents can cause the drug to precipitate. Researchers are looking into HPMC capsules as a better alternative to overcome these limitations.Storing and handling: Liquid SMEDDS are hard to store and handle because they can change over time.Limited ability to effectively target the lymphatic system: Although the lymphatic system bypasses the liver's first-pass effect, the drug's movement is not predictable, and it depends on its interaction with fats and triglycerides.Lack of good in vitro models: Traditional lab tests don't accurately represent their behavior, since SMEDDS depend on lipid digestion. The current in vitro models that attempt to replicate duodenal metabolism still need further validation and must be more closely aligned with in vivo conditions.Oxidation and polymorphism of the lipids used in formulating SMEDDS: lipids that contain unsaturated fatty acids are prone to oxidation, which means they need antioxidants to keep them stable. Additionally, lipids that soften with heat can change their structure, so it's crucial to maintain strict control over the manufacturing process.
MECHANISM OF SMEDDS13,14:
SMEDDS works by self-emulsifying. This happens when the change in entropy, which helps spread things apart, is greater than the energy needed to make the surfaces bigger. In a normal emulsion, the free energy depends on the energy needed to make a new surface between the water and oil. This can be shown with the equation:
ΔG = ?Nπr2σ
Here, ΔG is the free energy during the process, N is the number of droplets with radius "r," and "σ" is the energy at the surface over time. To lower the surface area and the free energy, the emulsion phases usually separate. In a self-emulsifying system, the energy needed to make the emulsion is very low, whether it's positive or negative, so the emulsification happens on its own. It only takes a little energy to emulsify, which happens because the interfacial area becomes more concentrated and unstable.
COMPOSITION OF SMEDDS:
Oil/ lipid phase:
Lipids help dissolve drugs that don’t mix well with water, making the intestinal cell membrane more fluid, speeding up the dissolution rate, and improving solubility in gastrointestinal (GI) fluids. They also protect drugs from chemical and enzymatic breakdown by changing the pharmaceutical properties of the drug. Most drugs used in SMEDDS are hydrophobic and dissolve better in triglycerides than in surfactants. Triglycerides are oily molecules that are very lipophilic. The ability of drugs to dissolve depends on the effective concentration of ester groups. Medium-chain triglycerides (MCT) have a higher capacity for dissolving substances and are more resistant to oxidation compared to long-chain triglycerides (LCT). Currently, MCT is being replaced by new semi-synthetic versions. These changes are significant for improving the water solubility of poorly soluble drugs. The oil phases are modified using vegetable oils and fats, which can be digestible or non-digestible. Examples include olive oil, palm oil, corn oil, oleic acid, sesame oil, soybean oil, and hydrogenated oil. Because of this, they are used in concentrations of 40–80%15.
Surfactants:
Surfactants are substances that help mix oil and water by preventing them from separating. They also help reduce the tension between different liquids and keep droplets from clumping together. Currently, the choice of surfactants is limited because of safety concerns for oral use. Natural emulsifiers, like lecithin, are preferred over synthetic ones because they are seen as safer. Nonionic surfactants are popular because they are less harmful and less likely to irritate the digestive system. They also mix well with other substances and help maintain the stability of emulsified vesicles across a wide range of pH levels and electrolytes. Surfactants play a key role in these systems by lowering interfacial tension and ensuring enough coverage at the interface to microemulsify both oil and water phases16.The choice of surfactant is important for making SMEDDS. When selecting a surfactant, it's essential to consider the HLB value and the safety of the surfactant. The HLB of a surfactant provides important information about its use in SMEDDS formulation. The surfactant or emulsifier used in SMEDDS should have a relatively high HLB and be hydrophilic. This allows for quick and easy mixing in the watery gastrointestinal fluid as a very fine oil17.
Co-surfactants:
In SMEDDS, high concentrations of surfactants are needed to reduce interfacial tension. However, these concentrations may cause gastric irritation. To address this, cosurfactants are used to lower the amount of surfactant needed. They help dissolve large amounts of either lipophilic drug or hydrophilic surfactant in a lipid base. This also decreases the oil/water interface, leading to the quick formation of a microemulsion. Cosurfactants with hydrophile-lipophile balance (HLB) values between 10 and 14 are commonly employed. Intermediate-chain-length alcohols like hexanol, pentanol, and octanol are preferred cosurfactants. They help reduce the oil-water interface and promote the spontaneous formation of microemulsion 18.
Co-solvents:
Organic solvents that are safe for oral use, such as ethanol, propylene glycol (PG), and polyethylene glycol (PEG), can dissolve significant amounts of either the hydrophilic surfactant or the drug in the lipid base19. These solvents can also function as co-surfactants in microemulsion systems. However, alcohols and other volatile cosolvents can evaporate into the shells of soft gelatin or hard, sealed gelatin capsules, causing the drug to precipitate. As a result, alcohol-free self-emulsifying microemulsions have also been discussed in the literature20.
FORMULATION DESIGN OF L – SMEDDS21:
1. Solubility studies: The first and most important step is to find out how much of the drug can dissolve in different oils, surfactants, and co-surfactants. This can be done using methods like the shake flask technique or an air oscillator at room temperature22. These solubility studies help us choose the oil that allows for the highest drug solubility, as well as the surfactant and co-surfactant that provide the best solubilization. Another goal is to achieve the highest drug loading while keeping the overall volume of the formulation low. When SMEDDS are diluted, drug precipitation may happen. This depends on the drug’s octanol-water partition coefficient and how much surfactants aid in drug solubilization 23.
2. Screening of Surfactants and Co-surfactants: Surfactants and co-surfactants are evaluated for how well they self-emulsify, the time it takes to emulsify, the clarity of the emulsion, and the distribution of droplet sizes. Non-ionic surfactants with high HLB values are usually preferred because they have better emulsifying properties and lower gastrointestinal toxicity. Adding co-surfactants lowers the needed surfactant concentration and improves the flexibility of the interfacial film, making it easier for microemulsions to form spontaneously24.
3. Construction of Pseudoternary Phase Diagrams: Pseudoternary phase diagrams are created using the phase titration method. This helps identify the microemulsion region and optimize component ratios. These diagrams offer useful information about the self-emulsifying area and aid in choosing formulation compositions that can make stable microemulsions across a wide range of dilutions. Phase inversion methods have also been used to improve emulsification efficiency25.
Phase Titration Method:
The phase titration method identifies the self-microemulsifying region and optimizes the composition of SMEDDS. In this method, mixtures of oil and surfactant/co-surfactant (Smix) are prepared in different ratios. These mixtures are gradually mixed with water while stirring gently. When a clear and uniform system forms, it indicates the creation of a microemulsion. The results are plotted on a pseudoternary phase diagram to find the best formulation composition26.
Phase Inversion Method
The phase inversion method relies on changing an emulsion system from water-in-oil to oil-in-water. This happens due to shifts in composition or temperature. Water is slowly added to the oil and surfactant mixture, or the temperature is changed, until spontaneous inversion takes place and a fine microemulsion forms. This method typically results in smaller droplet sizes and better emulsion stability.27,28.
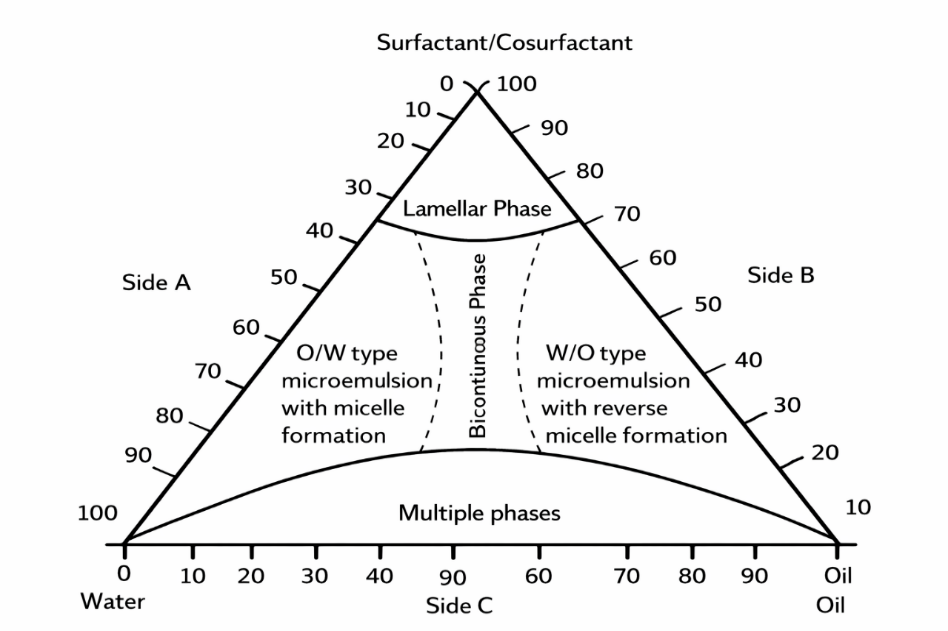
Fig 02 Ternary phase diagram29
Solidification Techniques for Converting L?SMEDDS to S?SMEDDS
Encapsulation of Liquid and Semisolid SMEDDS :
Encapsulating L-SMEDDS directly into hard or soft gelatin capsules minimizes processing steps, which reduces manufacturing complexity30. In semisolid systems, the formulation is heated just above its melting point, filled while molten, and then allowed to solidify inside the shell. Key variables include fill volume, which is usually 90% or less of the capsule capacity, viscosity, and filling temperature to prevent shell deformation and ensure consistency. This method works for both low-dose and relatively high-dose drugs without any extra drying steps31.
Adsorption onto Solid Carriers (Liquid- Solid Compacts) :
Adsorption changes L-SMEDDS into free-flowing powders or granules by loading the liquid onto porous, high-surface-area carriers like silica, magnesium aluminometasilicate (Neusilin®), magnesium trisilicate, microcrystalline cellulose, lactose, or other inorganic and organic excipients. The liquid is mixed with the carrier in mixers or high-shear granulators until complete adsorption occurs and acceptable flow is achieved. This process often allows high liquid loading of 40 to 70% w/w while keeping rapid self-emulsification during reconstitution. The resulting powders can be filled into capsules or compressed into tablets32.
Spray Drying:
Spray drying is one of the most common methods for solidifying materials in industry. L-SMEDDS, which is a mixture of a drug dissolved in oil, surfactant, and co-solvent, is atomized into a hot drying chamber. This often includes a dissolved or dispersed carrier, like maltodextrin, lactose, silica, or calcium silicate. Rapid evaporation of the solvent creates solid microparticles that trap or adsorb the SMEDDS phase and drug. Factors such as inlet and outlet temperature, atomization pressure, feed rate, and solid content play a critical role in determining particle shape, leftover solvent, redispersion behavior, and yield33.
Melt Granulation and Hot-Melt Extrusion (HME):
In melt granulation, L-SMEDDS is mixed with low-melting lipid or polymer binders using high-shear or fluid-bed granulators. Heating the mixture above the binder’s softening point allows it to form granules without needing an external solvent-drying step. These granules can be compressed into tablets or filled into capsules while still self-emulsifying upon dispersion34. HME provides a continuous way to solidify L-SMEDDS with polymers in a twin-screw extruder. This process creates extrudates that form microemulsions when they come into contact with water35. Key factors for processability and solid-state stability include the oil-binding capacity of the polymer, screw speed, barrel temperature, and feeding strategy, such as splitting the feeding of SEDDS and polymer36.
CHARACTERIZATION OF SMEDDS:
Visual Evaluation:
Visual evaluation is used to check how well SMEDDS self-emulsify after being mixed with water. If the solution becomes clear and transparent after dilution, it means a microemulsion has formed properly. Incontrast, a cloudy or milky appearance indicates incomplete emulsification or a macroemulsion. This observation also helps identify any drug precipitation or phase separation. Formulations are stable when no precipitation is seen. Adding more surfactant can help prevent precipitation, especially when water-soluble co-solvents are used37.
Droplet Size and Polydispersity Index (PDI):
Droplet size is an important factor that influences drug release and absorption. After proper dilution, SMEDDS should form tiny droplets with a narrow size range, which can be measured using dynamic light scattering (DLS). A smaller droplet size increases surface area, which improves dissolution. A recent study found average droplet sizes of about 183 nm with a PDI of 0.24. This indicates a uniform distribution and good stability after dilution38.
Zeta potential measurement:
Zeta potential is measured using a zeta potential analyzer after the sample is properly diluted. Higher absolute zeta potential values indicate better formulation stability because of increased electrostatic repulsion between emulsion droplets. In most SMEDDS formulations, the zeta potential is generally negative due to the presence of free unsaturated fatty acids in the lipid phase39.
Cloud Point Determination:
The cloud point is found by gradually increasing the temperature of the formulation in a water bath and checking the changes with a spectrophotometer. The cloud point is the temperature where a clear solution turns cloudy, shown by a drop in percentage transparency. Since normal body temperature is around 37 °C, SMEDDS formulations should have a cloud point above this to keep their self-emulsifying ability inside the body. Temperatures above the cloud point can cause surfactants to lose water, leading to phase separation and less drug solubility. The cloud point is influenced by factors like the lipophilicity of the drug and the formulation's composition40.
In-Vitro Dissolution Studies
In-vitro dissolution studies are commonly used to check how well self-microemulsifying drug delivery systems (SMEDDS) release drugs. These studies typically use the USP dissolution apparatus in aqueous or simulated gastrointestinal media. When diluted, SMEDDS quickly form fine microemulsion droplets that keep the drug solubilized, resulting in faster and more complete drug release compared to traditional formulations. This improved dissolution is mainly due to the large interfacial surface area of the droplets and the presence of surfactants that prevent drug precipitation. As a result, in-vitro dissolution testing is a key tool for predicting the potential increase in bioavailability of SMEDDS41.
Solid State Characterization:
The surface structure of solid SMEDDS is typically studied using SEM to evaluate particle shape, surface texture, and signs of leftover drug crystals or clumping. Samples are usually placed on double-sided adhesive tape attached to an aluminum stub, coated with a conductive metal like gold, and then imaged in a high vacuum.42 Following properties were studied: Angle of repose 43, Bulk density 44. Compressibility Index45, Differential scanning calorimetry (DSC)46, Fourier transform infrared spectroscopy47.
RECENT ADVANCEMENT:
Recent advancements in self-microemulsifying drug delivery systems (SMEDDS) have mainly aimed at overcoming the challenges of traditional liquid formulations and expanding their use in therapy. One significant progress is the introduction of supersaturable SMEDDS (S-SMEDDS). These systems include polymers that prevent precipitation, helping keep the drug in a supersaturated state after dilution. This approach reduces drug precipitation and improves oral bioavailability48. To address issues with stability, storage, and handling, researchers have turned liquid SMEDDS into solid dosage forms. They use methods like adsorption onto solid carriers, spray drying, melt extrusion, and freeze drying. This approach combines the bioavailability benefits of lipid-based systems with the ease of solid formulations49. Additionally, the introduction of new excipients and lipid materials has improved formulation stability and safety. Functional surfactants like D-α-tocopheryl polyethylene glycol 1000 succinate (TPGS) have shown the two benefits of improving drug solubilization and blocking efflux transporters. This leads to greater bioavailability50. More recently, researchers have explored combining SMEDDS with nanotechnology methods, including nanocarriers and liquisolid systems. This combination aims to achieve controlled drug release, targeted delivery, and better therapeutic effects51.
FUTURE PERSPECTIVES OF SMEDDS:
Future research on self-microemulsifying drug delivery systems is expected to focus on improving formulation optimization, stability, and clinical translation. The application of quality by design and computational tools may enhance formulation predictability and reproducibility. Development of controlled-release and stimuli-responsive SMEDDS could enable site-specific drug delivery and improved therapeutic outcomes. Exploration of novel, safe, and multifunctional excipients is likely to further enhance drug solubilization, permeability, and bioavailability. Additionally, integration of SMEDDS with nanotechnology-based platforms may expand their application to targeted delivery and complex drug molecules. Addressing scale-up, regulatory, and long-term stability challenges will be crucial for the successful commercialization of SMEDDS.
REFERENCE:




Deeksha*, Krishnananda Kamath K, Anirudh Bm, A. R. Shabaraya. Approaches For Formulation and Evaluation of Self-Microemulsifying Drug Delivery Systems (Smedds): A Review , Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 156-166. https://doi.org/10.5281/zenodo.18454493
 10.5281/zenodo.18454493
10.5281/zenodo.18454493