1 Department of Pharmacy, G.L.A University Mathura, Uttar Pradesh, India
2 Department of Arts, Lalit Kala Sansthan, Agra, Uttar Pradesh, India
3 Department of Pharmacy, Anand College of Pharmacy, Agra, Uttar Pradesh, India
4 Faculty of Pharmacy, Goel Institute of Pharmaceutical Sciences Lucknow, Uttar Pradesh, India
5,6,7 Faculty of Pharmacy, Agrawan Heritage University, Agra Uttar Pradesh, India
8 Department of Pharmacy, College of Pharmacy, Agra Uttar Pradesh, India
Schizophrenia is a disabling neuropsychiatric illness that is a chronic illness that is characterized by alterations in cognition, affect and social behaviour. Whereas standard antipsychotics drugs still form the foundation of method, the effectiveness is often not enough to manage negative and cognitive symptoms, and the poor efficacy is restricted by adverse effect drainage, which may decrease adherence. In the past decades, herbal medicine as a supplementary approach to treatment gained attention, which is facilitated by traditional systems like Ayurveda, Traditional Chinese Medicine and Unani medicine. Different botanicals such as those including Withania somniferum, Ginkgo biloba, Panax ginseng, Bacopa monnieri, Curcumin longa, and Rhodiola rosea have been found to modulate neurotransmitter systems, lower oxidative stress and neuroinflammation, increase neuroplasticity, and ameliorate metabolic status. These effects target some of the pathophysiological features of schizophrenia such as dopaminergic and glutamatergic imbalances, neuroinflammation, oxidative stress, HPA axis dysregulation as well as gene-environment interactions. Despite preclinical and clinical findings, the barriers to total acceptance by the Western population, including variation in herbal composition, inadequate standardization, and herb-drug interactions remain. Hence, it needs large-scale, well-controlled studies to formulate standard and evidence-based plans of using herbal medicines in the comprehensive management of schizophrenia.
Schizophrenia is a neuropsychiatric disease that is severe and chronic and is associated with the abnormality of thoughts, insights as well as emotional responds. Scorn antipsychotic pharmacotherapy being the fundamental modality of care, adverse effect profiles (top among them being the extrapyramidal symptomatology), and unimpressive usage adherence rates even in the long-term, have catalyzed the research investigating the suitability of complementary and alternative measures, the most widely studied of which include herbal remedies[1]. Herbal medicine has in the previous 20 years proved to be an added treatment to schizophrenia particularly, improvement of cognitive deficits, negative symptoms, and side effects of medication. Ethnopharmacological basis of these interventions usually based on the Traditional Chinese Medicine (TCM), Ayurveda, and other indigenous medicine[2]. During the last twenty years herbal medicine has been ascribed greater and greater significance as a complementary treatment of schizophrenia; special attention has been paid both to the possibility that it will improve cognitive deficit, negative symptoms, and adverse drug effect. Most of these solutions belong to the Traditional Chinese Medicine (TCM ), Ayurveda, and other native medical systems[3]. Particularly in the most recent scholarship on plant medicine, the plant Withania somnifera (Ashwagandha) has been singled out as an adaptogenic agent within the Ayurvedic practice of therapeutics, on account of its empirically-evidenced anxiolytic, anti-inflammatory, and cognition-enhancing effects, when used in the context of providing such treatment to individuals with schizophrenia[4]. There are many herbal preparations under research in cognition as cognitive enhancers. Panax ginseng, Bacopa monnieri and Salvia miltiorrhiza are some of the most studied and it has been found that they all have the capacity to regulate the neurotransmitter processes and boost the neurotrophic pathways in the end to impact better working memory and executive functions[5]. It is implied that botanical agents would help to reduce the negative outcome on metabolism due to the long-time treatment of antipsychotics. In particular, Rhodiola rosea and Berberine were shown to be effective in the glucose metabolism improvement and lipid deposition reduction processes, thus helping to establish better physical health in people who take long-term antipsychotic treatment[6]. With very encouraging empirical results, there is a need to integrate herbal therapies in the standard clinical practice of schizophrenia. The major deterrents include great variation in the composition of herbs, lesser degrees of standardization, and herb-drug interactions[7]. Schizophrenia is a multipronged psychiatric issue that is long-standing, lasting a lifetime and whose occurrence is highlighted by distributed disturbances in terms of putting thoughts, way of arranging it, the way of seeing both oneself and the external reality, emotional and interactional aspects. Prevalence rates reveal that the condition is likely to be faced in 1 % of the world population thus posing a heavy burden on its patients, their immediate family members as well as the health-care system across the globe[8]. The inadequacy of modern pharmacological therapies has led to the increase of academic inquiries concerning integrative practices especially herbal medicine which is the core aspect of established systems like Ayurveda, Traditional Chinese Medicine (TCM), and Unani medicine. The design of these systems is holistic in nature as they introduce herbal agents structured to mediate neurochemical pathways as a means of treating mental conditions[2]. Ginkgo biloba is among the best researched botanical and it has been discovered to have high degree of anticarcinogenic, antioxidative, and anti-inflammatory abilities. Research has revealed that its adjuvant treatment with antipsychotics, in addition to improving the therapeutic response, reduces positive and negative symptomatology of schizophrenia[3]. Withania somnifera, also commonly known as Ashwagandha, is yet another high ranked adaptogen and its pharmacological properties are familiar to the extent of validation. Remarkably, Ashwagandha demonstrates a high level of antipsychotic-like activity as recorded during clinical trials, which can probably be attributed to the simultaneous influence of cortisol regulation, synaptic plasticity, and processes relating to oxidative stress[4].
CAUSES OF SCHIZOPHRENIA – A SCIENTIFIC RATIONALE FOR HERBAL INTERVENTION
There is no unitary etiological mechanism of schizophrenia; instead, it is caused by a multidimensional and changing interaction between biological, environmental and developmental determinants. These interdependencies are crucial to explain and could not be done without examining the ways to treat the underlying neural disturbances of the schizophrenic disorder using specific herbal medicines.
1. GENETIC VULNERABILITY AND EPIGENETIC ALTERATIONS
The definite genetic predisposition of schizophrenia flirts with the 80 % heritability estimates. Empirical findings have pinned down risk variants in genes namely DISC1, COMT and NRG1, the functions of which can be summarized under synaptic signaling, dopaminergic metabolism and neurodevelopment. However, genetic variations are insufficient to entirely explain the development of the disease; their interaction with the environment in the form of exposure to environmental factors (via epigenetic modulations) results in the translation of a psychosis phenotype[9].
2. DOPAMINERGIC DYSREGULATION
Dopaminergic Dysregulation also forms one of the foundations of modern debates on the topic of schizophrenia. A contemporary theory is based on the notion that imbalance of mesolimbic hyperactivity and mesocortical hypoactivity is necessary in the expression of symptoms; mesolimbic hyperactivity in this theory can serve as the basis of positive symptomatology, whereas the mesocortical hypoactivity seems to be the root of negative symptomatology and cognitive deficits[10]. The current state of neuroimaging and pharmacological studies holdings has lent further support to the existing dopamine hypothesis of schizophrenia since it has been able to reveal an increased presynaptic capacity of dopamine synthesis in the associative striatum of both individuals with schizophrenia and those with high risks to develop this affliction. In particular, there is a consensus on the use of positron-emission tomography and radiotracer assessment, that has reached a point of anatomically localized overproduction of dopamine in the ventral striatum, which is diminished upon the administration of antipsychotics[11].
3. GLUTAMATERGIC AND GABAERGIC DYSFUNCTION
In addition to dopamine, a growing body of empirical research supports the essential role of glutamate neurotransmission, namely NMDA receptor hypofunction, in causing cognitive impairments, learning/memory deficits and NMDA receptor dysfunction. There is also a concomitant glutamatergic imbalance that disrupts GABAergic inhibition, that, in turn, destabilized cortical synchrony. Bacopa monnieri and Salvia miltiorrhiza botanicals have shown a potential in the regulation of glutamate and GABA systems[12].
4. NEURODEVELOPMENTAL INSULTS AND ENVIRONMENTAL RISKS
The conceptual models that are currently being used increasingly view schizophrenia as a neurodevelopmental disorder. Early stressors that disrupt early brain development are prenatal stressors, such as infections and nutritional shortcomings, and stressors encountered early in an urban environment, including social adversity[13].
5. NEUROINFLAMMATION AND OXIDATIVE STRESS
Oxidative stress should be defined as a condition of imbalance between the generation of reactive oxygen species (ROS) and the endogenous antioxidant defense response capacity to control them. It is believed that this imbalance contributes to conditions that include: lipid peroxidation, mitochondrial dysfunction, and neuronal apoptosis, and all have been reported in schizophrenia brain tissue. Some plant-derived antioxidants, such as Curcuma longa (curcumin), Ginkgo biloba and Centella asiatica, have been found to reduce the level of ROS and improve the structural integrity of mitochondria, which hold the promise of clinical use in schizophrenia patients[14].
6. HPA AXIS DYSREGULATION AND CHRONIC CORTISOL ELEVATION
Oxidative stress will occur in the case of surpassing the production of reactive oxygen species (ROS) in the ratios constrained by the efficiency of antioxidant defenses. The following effects are the production of lipid peroxidation, dysfunction in mitochondria, and neuronal apoptosis-the pathologies realized in the cerebral tissue of schizophrenic patients. Antioxidants are herbal (e.g. Curcuma longa (curcumin), Ginkgo biloba, Centella asiatica, etc.), which have been reported to mitigate the formation of ROS and support the integrity of the mitochondrion[15].
7. ENVIRONMENTAL STRESSORS AND SUBSTANCE USE
Epidemiological studies show that urban household environment, isolation experienced during childhood, childhood trauma and the use of cannabis are also linked to an increased risk of schizophrenia. Such exposures can affect the brain functions through epigenetics reprogramming. The available evidence indicates that some adaptogenic herbs can increase resilience, support the recovery of homeostatic balance in case of chronic psychosocial stress[16].
Table 1
|
Etiological Factor |
Herbal Intervention |
Mechanism of Action |
REFRENCES |
|
Genetic Vulnerability & Epigenetic Alterations |
Withania somnifera (Ashwagandha) |
Modulates gene expression, enhances synaptic plasticity |
[17] |
|
Dopaminergic Dysregulation |
Mucuna pruriens |
Increases dopamine levels, inhibits monoamine oxidase |
[18] |
|
Glutamatergic & GABAergic Dysfunction |
Bacopa monnieri, Salvia miltiorrhiza |
Enhances NMDA receptor function, restores GABAergic balance |
[19] |
|
Neurodevelopmental Insults |
Panax ginseng, Rhodiola rosea |
Enhances neuroplasticity, reduces early-life stress effects |
[20] |
|
Neuroinflammation & Oxidative Stress |
Curcuma longa, Ginkgo biloba, Centella asiatica |
Antioxidant, anti-inflammatory, preserves mitochondrial structure |
[21] |
|
HPA Axis Dysregulation & Cortisol Elevation |
Curcuma longa, Centella asiatica |
Decreases cortisol, strengthens antioxidant response |
[22] |
|
Environmental Stressors & Substance Use |
Ocimum sanctum, Rhodiola rosea |
Adaptogenic action, epigenetic regulation under psychosocial stress |
[23] |
PATHOGENESIS OF SCHIZOPHRENIA: A SCIENTIFIC BASIS FOR HERBAL APPROACHES
The careful understanding of the pathophysiology of schizophrenia as a multifactorial disorder preconditions the evaluation of herbal treatment interventions that are able to ameliorate the major neurobiological imbalances. Extant evidence on various mechanisms has been amalgamated in the subsequent synthesis that contributes to our increased understanding. One is, of course, alteration of neurotransmitter systems, particularly those of glutamate, GABA, and dopamine, which is a central pathology. Consistently, empirical literature illustrates changes in synaptic plasticity, glutamatergic and GABAergic receptor signalling; all of which have been considered to reflect neurodevelopmental disturbances. Second, functional brain abnormalities are based on maladaptive inflammatory cascades. It has been shown that immune cells that are pathogenic penetrate into the neural tissue and elicit infiltration by microglia and increase production of pro-inflammatory cytokines. Such processes combine to deteriorate synaptic development and pruning and may interrupt trophic support. Third, immune dysregulation impairs plasticity of immune cell phenotype which deregulates the neuroimmune interactions. Different lines of enquiry report a movement towards pro-inflammatory, murderous T-cell subsets and absence of the neuroprotective arm to the immune system. These phenomena also increase inflammatory disorders and weaken neurotrophic Doing. In short, concurrence of neuroimmune and neurotransmitter dysregulations result in both neurocognitive and behavioural deficits that are the hallmarks of schizophrenia. Herbal remedies that will target more than one node in these convergence points stand the best chance of generating significant clinical value.
1. NEURODEVELOPMENTAL AND NEURODEGENERATIVE DYNAMICS
Schizophrenia is conceptualized as a disorder rooted in abnormal early brain development, followed by progressive neurodegeneration, particularly during psychotic episodes, leading to treatment resistance and functional decline. Early intervention is emphasized to preserve neurocircuit integrity[24].
2. STRUCTURAL BRAIN ALTERATIONS
Both neuroimaging technologies and autopsy studies suggest less grey and white mass in the prefrontal, temporal, thalamic, and striatal areas in particular. Reductions of this nature can be found long before the onset of pharmacotherapy and worsen according to the duration of diseases[25].
3. NEUROTRANSMITTER DYSREGULATION
Dysregulation of dopaminergic transmission is one of the major key pathophysiological processes in schizophrenia. Positive symptoms are associated with hyperactivity of the mesolimbic dopaminergic pathway; negative and cognitive deficits are associated with the hypoactivity of the mesocortical pathway. Moreover, there has been proved glutamatergic and GABAergic imbalance. Abnormal functional results of the NMDA receptor, especially in quick-spiking cortical interneurons, are implicated in inhibited GABA induced rotational and cognitive functioning. Expanding on these results, additional mechanisms have been identified as down regulation of CB2 receptors and increased kynurenic acid (an NMDAR blocker) both of which further damage glutamatergic modulation as well as synaptic pruning[26].
4. IMMUNE ACTIVATION AND OXIDATIVE STRESS
The pathophysiology of schizophrenia has been associated with the constant elevation in the neuroinflammatory mechanisms characterized by the presence of elevated peripheral cytokines like interleukin-6(IL-6) and tumor necrosis factor-alpha (TNF-alpha) in combination with the compromised blood-brain barrier integrity, both of which stimulate microglial activation. At the same time, oxidative stress reduces neuronal loss, highlighted by oxidative signs of DNA damage (which are increased) and mitochondrial dysfunction[27].
5. GENE–ENVIRONMENT INTERACTION AND EPIGENETICS
Epigenetic alterations represent an important piece of the aetiopathogenesis of schizophrenia and their induction can be explained by the exceptional interaction of predisposing genes (i.e. DISC1, NRG1, COMT, DTNBP1) with environmental factors (i.e. prenatal infections, perinatal complications, nutritional deficiencies, childhood trauma, and cannabis).This kind of interactions reshapes neural circuitries and therefore increases likelihood of schizophrenia[28].
6. STRESS, HPA AXIS DYSFUNCTION, AND CORTISOL
The extended psychosocial stress has a dysregulatory effect on the hypothalamic-pituitary-adrenal axis, hence causing chronic cortisol increase. Hippocampal atrophy occurs with this hormonal imbalance, neuroplasticity is weakened and oxidative and inflammatory destruction is repeated[29].
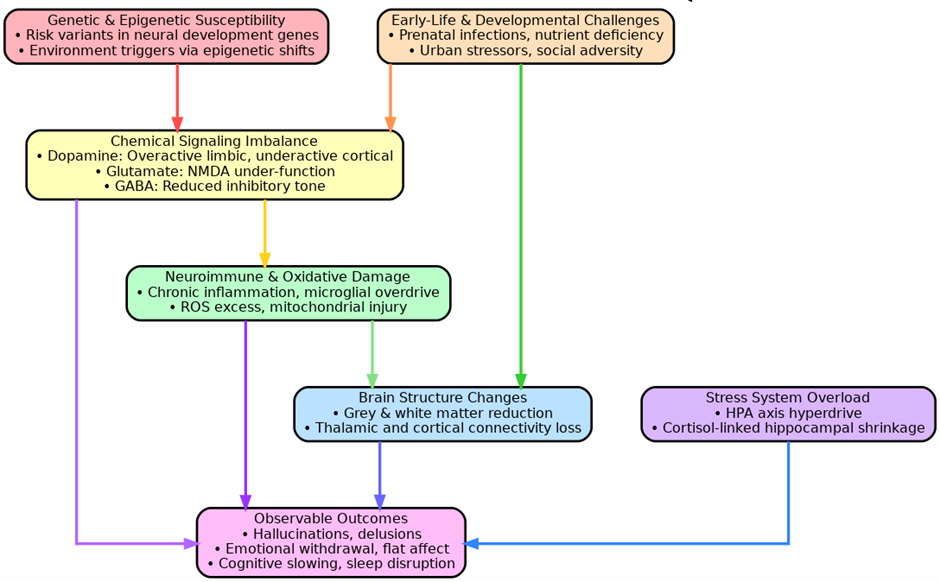
Figure.1 Neurobiological Pathways and Herbal Therapeutic Strategies in Schizophrenia
Table 2: Core Pathogenic Domains of Schizophrenia and Herbal Therapeutic Correlates
|
Pathogenic Domain |
Mechanistic Insight |
Herbal Correlates |
REFRENCES |
|
Neurodevelopment & Neurodegeneration |
Early neurodevelopmental defects with later neurodegeneration during psychosis result in synaptic loss and cognitive deficits. |
Withania somnifera, Centella asiatica support neuroplasticity and cognitive preservation. |
[30] |
|
Structural Brain Abnormalities |
Reductions in grey/white matter in frontal, temporal, thalamic areas even before treatment onset. |
Ginkgo biloba, Bacopa monnieri enhance cerebral circulation and support structural integrity. |
[31] |
|
Neurotransmitter Dysregulation |
Dopaminergic imbalance, NMDA receptor hypofunction, and GABAergic dysfunction underlie core symptoms. |
Valeriana officinalis, Rhodiola rosea regulate dopaminergic and GABAergic signaling. |
[32] |
|
Neuroinflammation & Oxidative Stress |
Elevated cytokines, microglial activation, and ROS damage mitochondrial and synaptic function. |
Curcuma longa, Panax ginseng possess anti-inflammatory and antioxidant mechanisms. |
[33] |
|
Gene–Environment & Epigenetic Modulation |
Genetic predispositions interact with environmental insults, inducing maladaptive epigenetic changes. |
Resveratrol, Curcumin modulate DNA methylation and histone acetylation. |
[34] |
|
HPA Axis Dysregulation & Chronic Stress |
Chronic cortisol elevation from stress impairs hippocampus and neuroplasticity, worsening disease trajectory. |
Ashwagandha, Rhodiola rosea reduce cortisol, modulate HPA axis, and build stress resilience. |
[35] |
SIGN AND SYMPTOMS
Table3: Symptom Clusters in Schizophrenia and Herbal Therapeutic Interventions – Mechanistic & Clinical Insights
|
Symptom Cluster |
Core Clinical Features |
Herbal Intervention |
Mechanistic Action |
DOI |
|
Positive Symptoms |
Hallucinations, paranoid delusions, conceptual disorganization |
Withania somnifera (Ashwagandha) |
Attenuates dopaminergic hyperactivity (mesolimbic pathway), modulates NMDA receptor function |
[36] |
|
Negative Symptoms |
Avolition, anhedonia, affective flattening, social withdrawal |
Panax ginseng |
Enhances BDNF signaling and synaptic plasticity; augments dopaminergic and serotonergic tone in the prefrontal cortex |
[37] |
|
Cognitive Impairment |
Attention deficit, impaired working memory, reduced executive function |
Bacopa monnieri |
Facilitates acetylcholine transmission, protects hippocampal neurons from oxidative injury, supports learning and memory |
[38] |
|
Affective Dysregulation |
Depression, anxiety, irritability, low motivation |
Rhodiola rosea |
Modulates HPA axis; restores monoaminergic balance (serotonin, norepinephrine); reduces neuroinflammatory signaling |
[39] |
|
Sleep Disturbances |
Insomnia, disrupted circadian rhythm, non-restorative sleep |
Valeriana officinalis (Valerian) |
Potentiates GABAergic neurotransmission, enhances sleep onset latency and quality, reduces hyperarousal |
[40] |
|
Psychomotor Abnormalities |
Motor retardation or agitation, catatonic features |
Ginkgo biloba |
Improves cerebral perfusion, scavenges reactive oxygen species, supports neuronal energy metabolism and mitochondrial function |
[41] |
|
Mood Instability |
Rapid mood fluctuations, dysphoria, lability |
Curcuma longa (Curcumin) |
Inhibits pro-inflammatory cytokines (e.g., TNF-α, IL-6), modulates serotonin pathways and NF-κB signaling |
[42] |
HERBAL MEDICINES OF SCHIZOPHRENIA
Schizophrenia is a psychiatric disorder that is characterized by chronicity and is characterized by the experience of delusions, hallucinations, cognitive, and social dysfunctions; therefore, it should be treated in the long-term using clinical management methods that are usually limited due to the adverse effects of the medication[43]. It is highlighted in recent scientific studies that herbal medicines hold vision in underlying therapeutic intension with regard to being used as an adjunct treatment that will cause greater effect coupled with antipsychotic induced side effects[44].
1. WITHANIA SOMNIFERA (ASHWAGANDHA)
The herb Withania somnifera (Ashwagandha) has been found to produce antipsychotic-like effects by regulating oxidative stress levels, GABAergic systems and neuroinflammation in animal models as well as clinical trials[45]. In one recent randomized, placebo-controlled and double-blind trial, it was shown that when Ashwagandha, an herbal supplement, was used as an adjunct treatment on patients with schizophrenia, measurable improvements in both magnitude and negative symptomatology was observed[45].
2. GINKGO BILOBA
Ginkgo biloba is a botanical species, commonly associated with large flavonoid and terpenoid content, which has been linked to cognitive improvement in human beings and loss of tardive dyskinesia signs in patients with schizophrenia[46]. Another 8-study meta-analysis randomized controlled trial shows that when taken together with antipsychotic drug, Ginkgo biloba has a significant positive outcome with regard to improvement of positive symptoms and also in ridding of overall psychopathology. The finding lends to the expanding body of knowledge pointing toward adjunctive Ginkgo biloba supplementation being a potentially efficacious adjunct to traditional, pharmacotherapy of schizophrenia[47].
3. PANAX GINSENG
Panax ginseng is an adaptogenic herb proven to have antipsychotic and neuroprotective effects in preclinical studies, including its ability to modulate dopamine as well as act as an antioxidant[48]. Based on the current evidence, it suggests that conventional Chinese formulas like Wendan decoction, and Anshen Dingzhi Wan are in the clinical trials to determine their effectiveness as drugs that can improve emotional regulation and reduce psychotic symptoms in those who already experienced a first episode[49]. Most often, herbal preparations trigger their pharmacological effects due to the modulation of neurotransmitter systems, namely dopaminergic, glutamatergic, and GABAergic pathways, as well as restore the neuroinflammatory process and promote neuroplasticity. Such features relate to the characteristics of schizophrenia pathophysiology [50]. Even though it has gathered strong empirical results, most studies are limited by their small sample size, lack of standardised formula and poor blinding guidelines. In turn, such large-scale and multicentric trials are of utmost importance in the development of evidence-based clinical guidelines[51].
4. BACOPA MONNIERI
The allostatic stability has been found to be increased by bacopa monnieri (Brahmi) via its neuroprotective effects and support cognitive abilities, since it regulates the antioxidant defense against the antagonism and controls dopaminergic neurotransmission. This effect deserves more research with regards to cognitive impairment manifested in schizophrenia[52].
5. CURCUMA LONGA (TURMERIC)
Curcumin as the major component of curcuma longa (turmeric) exhibits anti-inflammatory, antioxidant as well as neuroprotective properties and have the capability to reduce the oxidative stress and neuroinflammation typical of schizophrenia[53].
6. RHODIOLA ROSEA
Rosea affects the mind with psychotropic effects that increase mental output, counter fatigue and modify stress mechanism mechanism by affecting serotoneric and dopaminergic transmissions making it a potentially relevant adjunctive agent in the treatment of mood-related symptoms in schizophrenias[54].
7. GASTRODIA ELATA
The traditional Chinese herb Gastrodia elata (Tian Ma) has neuroprotective and anticonvulsant properties and displays potent antioxidant properties mediated through changes in GABAergic pathways. They can be used in treatment of psychotic symptoms using such properties[55].
8. MELISSA OFFICINALIS (LEMON BALM)
Melissa officinalis ( Lemon Balm ) has both anxiolytic and mood-stabilizing properties that are mediated with help of cholinergic and GABAergic transmission. The mechanism has the potential to offer symptomatic support to anxiety and agitation that is related to schizophrenia[56].
9. ZIZIPHUS JUJUBA
Traditionally, Ziziphus jujuba (popularly referred to as jujube seed) has been used in the traditional medicine because of its anxiolytic, anti-anxiety, and cognitive-enhancing effects. Recent pharmacological studies suggest that at least part of those effects are due to activity on γ-aminobutyric acid (GABA) receptors and to the increased expression of neurotrophic factors[57].
10. SCUTELLARIA BAICALENSIS
Flavonoids presented in Scutellaria baicalensis (Chinese skullcap) including baicalin in particular have been shown to have neuroprotective and anti-inflammatory effects hence treatment in schizophrenia via the regulation of glutamate induced excitotoxicity[58].
CENTELLA ASIATICA (GOTU KOLA)
Gotu Kola- Centella asiatica is a demonstrated to carry strong neuro regenerative and cognitive enhancement functions through its positive association effects on BDNF expression, and antioxidant processes, both of which can be used to compensate the cognition shortcomings of Schizophrenia[59].
TABLE 4 : PROMISING HERBAL MEDICINES IN SCHIZOPHRENIA – MECHANISMS AND EVIDENCE-BASED FINDINGS
|
Herbal Medicine |
Key Actions |
Mechanisms Involved |
Reference (DOI / PMID) |
|
Withania somnifera (Ashwagandha) |
Reduces oxidative stress, inflammation, and improves negative symptoms |
GABAergic modulation, anti-inflammatory, antioxidant |
[60] |
|
Ginkgo biloba |
Enhances cognition, reduces antipsychotic-induced side effects |
Flavonoids & terpenoids; antioxidant and neuroprotective |
[61] |
|
Panax ginseng |
Improves emotional regulation, antioxidant, antipsychotic-like effects |
Dopaminergic modulation, neuroprotection |
[62] |
|
Bacopa monnieri |
Enhances memory, cognition, and neuronal protection |
Antioxidant activity, modulation of dopaminergic system |
[63] |
|
Curcuma longa (Turmeric) |
Attenuates neuroinflammation and oxidative stress |
Curcumin-mediated anti-inflammatory & antioxidant mechanisms |
[64] |
|
Rhodiola rosea |
Alleviates stress-induced symptoms, improves fatigue and mood |
Modulates serotonergic and dopaminergic pathways, adaptogenic effects |
[65] |
|
Gastrodia elata |
Neuroprotective and anticonvulsant; enhances GABAergic activity |
Enhances GABA transmission, antioxidant properties |
[66] |
|
Melissa officinalis (Lemon Balm) |
Provides anxiolytic and mood-stabilizing effects |
Cholinergic enhancement, GABA receptor agonism |
[67] |
|
Ziziphus jujuba (Jujube) |
Improves cognition and reduces anxiety |
GABA receptor activity, upregulation of neurotrophic factors |
[68] |
|
Scutellaria baicalensis |
Reduces glutamate excitotoxicity, exhibits anti-inflammatory effects |
Flavonoids (baicalin), NMDA receptor inhibition |
[69] |
|
Centella asiatica (Gotu Kola) |
Enhances cognition and supports neurogenesis |
Upregulates BDNF, antioxidant and neurotrophic modulation |
[70] |
Table 5 Marketed Formulation
|
Sr. No. |
Product Name |
Main Ingredient |
Dosage Form |
REFRENCES |
|
1 |
KSM-66® Ashwagandha |
Withania somnifera root extract |
Capsule |
[71] |
|
2 |
Tebonin® |
Ginkgo biloba leaf extract (EGb 761) |
Tablet |
[72] |
|
3 |
Ginsana® |
Panax ginseng extract (G115) |
Capsule |
[73] |
|
4 |
Brahmi Mind® |
Bacopa monnieri whole plant extract |
Capsule |
[74] |
|
5 |
CurcuWIN® |
Curcuma longa (Curcumin) standardized extract |
Capsule |
[75] |
|
6 |
Rhodiolife® |
Rhodiola rosea root extract |
Capsule |
[76] |
|
7 |
Tian Ma Wan® |
Gastrodia elata tuber extract |
Tablet |
[77] |
|
8 |
Melissa Dream® |
Melissa officinalis leaf extract |
Tablet |
[78] |
|
9 |
Jujube Seed Formula® |
Ziziphus jujuba seed extract |
Capsule |
[79] |
|
10 |
Baicalin Plus® |
Scutellaria baicalensis root extract |
Capsule |
[80] |
CONCLUSION
The now top-priority management of schizophrenia requires a multidimensional approach that would encompass the symptomatologic and long-term quality-of-life aspects. Nature remedies, which are based on the traditional healing paradigm, offer one path that needs further investigation and may become promising supplemental treatments that recruit a variety of neurobiological processes engaging in the condition. Empirical evidence suggests that special botanicals can complement the use of standard pharmacotherapies by improving cognitive performance, dampening negative symptoms, alleviating pharmacies-mediated adverse outcomes and enhancing stress resistance. However, integration into everyday clinical use is inhibited by the influence of variables that include variability in dosage prescribed, lack of regulatory supervision, and a comparative sparsity of bigger-scale experiments. Consistent formulas, high-quality clinical testing, and strict evaluation of the safety profiles will be the key requirements before the addition of the herbal treatment to the general psychiatric services. Current studies have a potential in the development of more patient-centered and holistic approach to treatment of schizophrenia with the use of herbal medicine.
REFERENCES


Amar Saxena, Shrestha Saxena,Yash Saxena, Pramod Kumar Mishra, Ashita Jain, Ankit Kumar, Sanjeev Kumar, Prabhat Goyal, Neuroprotective Potential of Medicinal Plants in Schizophrenia: Mechanisms, Efficacy, and Future Pathways, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 2523-2539. https://doi.org/10.5281/zenodo.16932838
 10.5281/zenodo.16932838
10.5281/zenodo.16932838
