
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Krishna School of Pharmacy and Research, Drs Kiran and Pallavi Patel Global University, Vadodara, 391240
Obesity is a rapidly growing worldwide health problem, estimated to be present in 2.7 billion adults by the year 2025, and is particularly associated with a multitude of comorbidities such as type 2 diabetes, cardiovascular disease, and metabolic disturbances. In the presence of available traditional lifestyle, pharmacologic, and surgical treatments, long-term control of obesity is poor because of their moderate efficacy, compliance, and patient heterogeneity. Over the past few years, nutraceuticals have also presented themselves as effective adjuncts to obesity prevention and treatment due to their varied bioactive molecules with desirable metabolic and anti-inflammatory actions. This review explores up-to-date evidence regarding the effectiveness of certain nutraceuticals—i.e., alpha-lipoic acid, marine algae, cinnamon, chromium, conjugated linoleic acid, bitter melon, and African mango—to modulate body weight, enhance insulin sensitivity, and improve inflammatory markers in subjects with overweight and obesity. Meta-analyses of clinical trials suggest that nutraceutical supplementation is able to record modest weight loss, enhance body composition, and positively influence metabolic parameters, although results are still heterogeneous between studies. The review also signals methodological limitations and regulatory issues in the research on nutraceuticals, such as ingredient heterogeneity, absence of global standardization, and limitations in clinical trial design and efficacy outcomes. In summary, combining evidence-based nutraceuticals with personalized nutrition, enhanced delivery systems, and stringent regulatory control presents a safer, more sustainable approach to complement traditional obesity treatments and counter the international obesity pandemic.
A. Global Burden of Obesity and Associated Comorbidities
Obesity is on the increase all over the world, and in 2025, the number of obese and overweight adults is projected to be 2.7 billion [1]. Obesity has been identified as a chronic, relapsing illness that is becoming more common in the lives of more and more individuals globally, and the prevalence of obesity is projected to rise to 18 percent in men and more than 21 percent in women by 2025. [2]
BMI can be used in children of the same sex and the same age in comparison in the paediatric population. An underweight BMI among children is below the 5th percentile, and an obese BMI is above the 95th percentile. [4].
Numbers and Classifications of Body Mass Index
Among these, it is estimated that 257 million adults globally (6% of men and 9% of women) will be living with severe obesity (herein referred to as a body mass index (BMI) >35 kg/m²), and this is projected to rise swiftly to an estimated 202 million in 2016. A BMI of 35 kg/m² is generally considered the point at which a person qualifies for medical treatment to mitigate the risk of severe consequential ill health. The comorbidity associated with it is significant, with impaired glucose tolerance, type 2 diabetes, hypertension, hepatic steatosis, cardiovascular disease, liver disease, and some cancers. Considerably, it is projected that 12 million children will develop impaired glucose tolerance, 4 million will develop type 2 diabetes, and 27 million will develop hypertension by 2025 [3, 4].
B. Limitations of Conventional Obesity Management Strategies
Obesity remains a highly prevalent major health concern globally, accounting for numerous chronic diseases, including type 2 diabetes (T2D), hypertension (HTN), dyslipidaemia, cardiovascular disease (CVD), non-alcoholic fatty liver disease (NAFLD), steatohepatitis (NASH), and obstructive sleep apnoea, leading to impaired quality of life and increased mortality [10, 11]. Weight loss of 5–10% is associated with prevention and amelioration of much obesity-related comorbidity, but long-term benefits are contingent upon sustainability of the initial weight loss [2, 3]. Intensive lifestyle interventions that combine diet, exercise, and behavior therapy are generally effective in the short term, but not all patients lose weight, and the majority of patients who achieve initial success are unable to maintain the weight loss during long-term follow-up, even with continued intervention [4, 5]. Since obesity can result from a myriad of causes, including genetic, epigenetic, physiological, medical, psychological, and environmental factors, not all patients benefit from any given therapeutic modality. Furthermore, patients who are severely obese and have made numerous prior unsuccessful weight loss attempts with dieting tend to believe that they have a biological illness and may show preference for medical or surgical interventions [6]. Currently, bariatric surgery is the most effective treatment for patients with severe obesity to achieve substantial long-term weight loss [7]. However, bariatric surgery is expensive, irreversible in most cases, and carries a small risk of serious complications, and thus is recommended only for patients with severe and complicated obesity. Therefore, for patients with obesity who have not achieved adequate benefit from lifestyle interventions, are unable to maintain the initial weight loss, and/or have other medical conditions that make it difficult for them to comply with lifestyle interventions, pharmacotherapy is the next logical step in clinical care before considering bariatric surgery as the tertiary option [8].
C. Emergence of Nutraceuticals: Definition and Scope
Nowadays, 315 million people worldwide suffer from obesity, making it a public health concern. Many illnesses, including high blood pressure, congestive heart failure, angina pectoris, hyperlipidaemia, respiratory conditions, osteoarthritis, cancer, renal vein thrombosis, and decreased fertility, are associated with obesity. [6].
The more readily available high-fat, high-energy meals are one of the main causes of obesity. Given how common obesity is around the world, diet and exercise are crucial for both preventing and treating it. Large-scale research is now being conducted on nutraceutical therapies as possible treatments for weight control and obesity. Potential antiobesity benefits are seen in nutraceuticals such as Psyllium fiber, Momordica charantia, and capsaicin conjugated linoleic acid. [7].
It has been demonstrated that calorie restriction and increased physical activity are only marginally effective in treating obesity, despite the fact that excessive consumption of energy-rich foods, such as snacks, processed meals, and beverages, causes weight gain. In order to prevent or treat obesity, researchers and obese people are turning to medications and nutraceuticals. For body weight loss, an efficient nutraceutical that can raise energy expenditure and/or lower calorie intake is preferred. Caffeine, ephedrine, chitosan, ma huang, guarana, and green tea are examples of herbal stimulants that can help people lose weight. [8] However, because they might have negative side effects, their usage is debatable. 5-hydroxytryptophan and green tea extract may help people lose weight; the latter reduces hunger, while the former raises energy expenditure. [8, 9]
"Nutraceutic" is a phrase that combines the words "pharmaceutics" and "nutrition." The phrase is used to describe items that are separated from herbal products, dietary supplements (nutrients), certain diets, and processed meals like cereals, soups, and drinks that are utilized as medicines in addition to being used for nourishment. [10,]
The phrase "nutraceutical" items are regulated in the United States as dietary supplements, medications, and food additives. Varied nations have varied definitions for the phrase, but generally speaking, it refers to a substance that is separated from food and marketed in medical forms that are not often connected to food. A substance that has physiological benefits or offers protection against chronic illnesses might be categorized as a nutraceutical product. [1] Nutraceuticals can be used to prolong life, prevent chronic illnesses, promote health, slow down the aging process, or support the body's structure or function. [11]
Unlike medicines, nutraceuticals are compounds that often lack patent protection. Although both pharmaceutical and nutraceutical substances may be used to treat or prevent illnesses, only pharmaceutical substances are approved by the government. [12]
D. Rationale for this Review Article
Obesity has emerged as one of the most critical issues facing the world in terms of health complications, cardiovascular diseases, loss of quality of life, and increased expenditure on health care. Although the conventional methods of diet adjustments, exercise, and drug therapy are also available, their overall results are quite dissatisfactory because of the lack of motivation, negative side effects, and individual variability. The latter just proves that more individual, safe, and efficient methods are needed.
Recent nutraceutical science and precise nutrition advances offer an excellent basis to build such approaches. Nutrigenomics and nutrigenetics insights can be used to tailor dietary advice based on an individual genomic profile, and multi-omics techniques can be used to identify dysfunctions of certain metabolic processes. Meanwhile, the stability, absorption, and activity of bioactive compounds that have demonstrated anti-obesity effects are increased by novel nano-carrier delivery systems like liposomes and solid lipid nanoparticles.
Also accompanying these scientific inventions, the controlling agents are also reforming to make the products available and to make false claims and defenses for the consumer. But things like misleading marketing, low consumer awareness, and uneven international regulations remind me of the significance of harmonization and education. The responsible inclusion of nutraceuticals in the management of obesity is further enhanced by the participation of healthcare professionals in evidence-based product development, clinical validation, and post-marketing surveillance.
Thus, to find out how nutraceuticals may help as a complementary means of managing obesity is timely and worthy. Nutraceuticals have the potential to offer safer, more efficient, and more sustainable long-term solutions to obesity prevention and care by integrating precision nutrition, standardized delivery technologies, effective regulation, and consumer education.
Adipose tissue may collectively release over 50 hormones and signaling molecules known as adipokines, according to several studies. These adipokines are essential for glucose metabolism and immunity [13]. IL-1 receptor antagonist (IL-1Ra), apelin, adiponectin, transforming growth factor-beta (TGF-beta), interleukins (IL)-10, IL-4, and IL-13 are among the anti-inflammatory adipokines released by the adipose tissue of a lean individual. On the other hand, an obese person's adipose tissue mostly secretes pro-inflammatory cytokines such as TNFs, IL-6, resistin, visfatin, leptin, angiotensin II, and plasminogen activator inhibitor-1 [14]. Pro-inflammatory cytokines, including tumor necrosis factor-alpha (TNF-alpha) and leptin, a hormone involved in the regulation of appetite and energy balance, are secreted by adipose tissue cells [15]. Leptin secretion is influenced by the quantity of fat stored in adipose tissue. The body's fat stores are directly correlated with adiponectin, another hormone produced by adipose tissue [16]. The cardiovascular risk profile is linked to both adiponectin and leptin. Adipose tissue dysfunction has been linked to the ratio of leptin to adiponectin. Resistin, a pro-inflammatory adipokine that functions as an insulin antagonist, is another hormone released by adipose tissue [17]. One study's findings demonstrated that obese diabetic mice had higher levels of resistin than lean, non-diabetic mice [18]. Previous research has shown that exogenously delivered resistin causes mice' endogenous glucose production to increase, as well as their total plasma glucose levels [19]. One notable difference in resistin production between species is that humans only produce adipokines through mononuclear cells, such as macrophages and peripheral blood mononuclear cells. In rodents, both macrophages and adipocytes can generate resistin [20]. Found a new unique adipose tissue cytokine named visfatin [21]. This cytokine, a protein mediator secreted by fat cells (high expression levels in visceral fat cells), operates similarly to nicotinamide phosphoribosyl transferase (Nampt), an enzyme engaged in the nicotinamide adenine dinucleotide (NAD+) salvage process. It was first identified as the pre-B cell colony-enhancing factor (PBEF) released by human peripheral blood cells [22]. Visfatin was first identified as a growth factor for B lymphocyte precursors in the liver, skeletal muscle, and bone marrow. The growth factor for B lymphocyte precursors in the liver, skeletal muscle, and bone marrow was initially discovered to be visfatin. It has an impact similar to that of insulin. There is a positive correlation between the quantity of white adipose tissue (WAT) and the level of visfatin in the blood. Adipose tissue also produces a variety of other hormones and cytokines. The connection between obesity and elevated cytokine production is currently unknown. In the event of excessive energy storage, we can only hypothesize that there must be systems functioning both inside and outside the adipose cell to preserve or return energy balance. These cytokines should be produced locally as part of a regulatory system that prevents lipid-loaded adipocytes from accumulating additional lipids. When the inflammatory response cannot be controlled because of persistent obesity, the issue occurs when this local reaction develops into a systemic chronic state. Although the exact processes behind the relationship between obesity and chronic inflammation remain unclear, several plausible ideas have been put forth [23].
Numerous redundant and reciprocal pathways govern food intake and energy expenditure. Communication between the brain and peripheral tissues, including the stomach and adipose tissue, lies at the heart of these processes. Energy intake is regulated by enteric sensory pathways, which in turn set off vagal afferent signals and endocrine cascades that, among other things, activate brain regions that regulate hunger and feeding behavior. Energy expenditure is moderated by many of the same processes. The resting metabolic rate accounts for around 70% of total energy expenditure and is closely linked to fat-free mass [24]. The thermal effect of meals and exercise accounts for the remaining energy expenditure. These areas of energy expenditure are mediated by particular hormonal and neurological processes, which may play a significant role in obesity [25].
When food enters the duodenum, different nutrients activate nutrient-specific receptors on enteroendocrine cells, which causes the production of hormones that control food intake and affect motility, including GE. [26]. As has been well described elsewhere, some of these hormones, like ghrelin, are orexigenic (they stimulate hunger), while others, like peptide YY (PYY), glucagon-like peptide 1 (GLP-1), oxyntomodulin, cholecystokinin (CCK), and amylin, are anorexigenic (they promote satiety) [27]. These peptides penetrate the bloodstream to operate on distant places, activate autonomic neuronal circuits, and affect the activity of nearby cells. The specific action of GLP-1, which is released by L-cell enteroendocrine cells in the colon and small intestine in response to intraluminal nutrients, specifically fat and glucose, is a good example of these general mechanisms. By encouraging insulin secretion and suppressing glucagon secretion, GLP-1, like other incretion hormones, also affects how nutrients are used. GLP-1 lowers the GE rate by activating myenteric neurons and vagal afferent nerves. This process encourages satiety and reduces calorie intake, leading to an anorexigenic effect. Similar effects are achieved by other enteroendocrine-derived peptides, such as CCK, which slows GE, increases meal termination, and stimulates vagal afferents [28]. Although it is known that circulating meal-related peptides, including amylin, can reach the bloodstream and directly affect the nucleus tractus solitarii (NTS) and postrema of the central nervous system (CNS), not just through vagal afferent transmission [29]. It is unclear if GLP-1 and CCK, two additional important enteroendocrine hormones, act similarly. P/D1 enteroendocrine cells release the orexigenic peptide hormone ghrelin. It stimulates food intake and changes in a number of gastrointestinal processes by activating the vagus nerve. Rat models demonstrate that ghrelin injection significantly reduces physical activity in addition to changing calorie intake [30]. The direct role of several hormones, including PYY and CCK, in obesity remains unknown. Studies have shown mixed outcomes with reduced postprandial secretion and inconsistently decreased baseline hormone levels in obese patients, despite the obvious mealtime-related roles of PYY and CCK. Weight loss is clearly influenced by other hormones, such as GLP-1. According to physiological research, post-meal GLP-1 levels in obese people are suppressed and essentially return to normal following weight loss [31]. Despite this, these studies fail to differentiate between correlation and causality. Nonetheless, GLP-1 receptor agonism is frequently linked to considerable weight loss in pharmacological trials. Like GLP-1, gastric inhibitory polypeptide (GIP) is an incretion hormone, albeit it hasn't been shown to have much of an impact on weight [32]. However, a combination of GIP and GLP-1 agonism causes significant weight loss, which may be connected to GIP's special changes in the lipid cycling of adipose cells. However, a combination of GIP and GLP-1 agonism causes significant weight loss, which may be connected to GIP's special changes in the lipid cycling of adipose cells [33]. This combination's action highlights how these hormones work in dynamic biological systems. To elucidate the function of meal-related peptides in feeding and energy control, more physiological research is required.
Adipose tissue itself is a significant modulator of energy control and a possible cause of obesity. Among the most significant and well-understood adipose-derived signals are leptin and adiponectin. Adipocytes are the primary, though not the only, source of leptin. There is a strong correlation between its production and white adipose mass [34]. Leptin's physiological function is to signal nutritional status, especially when energy is being depleted. A decrease in leptin levels is thus linked to weight reduction and fasting. Leptin's capacity to influence neuroendocrine changes to reduce calorie intake has been demonstrated in human and animal models [35]. Through its binding to receptors in the brainstem, hypothalamus, and arcuate nucleus, leptin regulates energy expenditure and satiety. Severe obesity is caused by homozygous loss-of-function mutations that change signaling through the leptin receptor or reduce leptin synthesis, secretion, or biologic activity [36]. Moreover, leptin seems to change energy consumption. Reduced thermogenesis occurs in rat models when leptin signaling pathways in the arcuate nucleus are disrupted. When these pathways are stimulated, thermogenesis rises [37]. This data demonstrates how changes in energy intake and expenditure caused by leptin may counteract weight gain and a positive energy balance. Exogenous leptin therapy's effects on metabolism and weight loss provide scientific evidence of its effectiveness [38]. However, current research indicates that exogenous leptin does not significantly aid in weight loss in obese people, even if leptin resistance and hyperleptinemia are common in these patients. Although the underlying physiological mechanisms and clinical ramifications are yet unknown, research is currently being conducted on other hormones associated with similar signaling pathways, including amylin, which may augment leptin signaling [39]. Only adipocytes make adiponectin, which is essential for maintaining weight homeostasis and for metabolic processes like fatty acid oxidation, lipid control, and insulin sensitivity. Both visceral adipose load and obesity are linked to lower plasma adiponectin levels [40]. In actuality, elevated adiponectin levels are linked to diet and weight loss [41].
Both local and systemic inflammation are caused by obesity. Measures of obesity and cardiometabolic risks are closely linked to markers of inflammation [42]. Lipid pathway malfunction and adipokine changes that stimulate strong immunological and inflammatory pathways may be the main causes of this inflammation. Increased intracellular lipid loads seem to overpower oxidative pathways, leading to the accumulation of fatty acids and fatty acid intermediates, including ceramide, even though the triggering mechanisms are still mostly theoretical [43]. Additionally, obesity is linked to hypoxia and changed adipose tissue shape, both of which may exacerbate metabolic and inflammatory disorders [44]. Research has shown that people with obesity-related insulin resistance had higher levels of interleukin 6 and tumor necrosis factor α secreted in their adipose tissue [45]. Additionally, tissue-specific immunogenic changes are indicative of obesity. Toll-like receptor 4 receptors and immune cell recruitment may be triggered by free fatty acids and their intermediates [46]. Both innate and adaptive immunological responses are evident in obese patients' adipose tissue, with elevated macrophage and T-cell [47].
Trillions of microorganisms, including yeast, bacteriophages, and fungi, which are all outcompeted by bacteria, make up the gut microbiome and interact with the host's physiology. By examining the bacterial genes and products isolated from intestinal biopsies or fecal samples, advanced methods known as omics (i.e., metagenomics, meta-transcriptomics, meta-proteomics, and metabolomics) can now determine this interaction in more detail. The identification of more bacterial diversity in healthy persons was made possible by technological advancements in the study of the gut microbiome [48]. The pathophysiology of obesity may be significantly influenced by changes in the composition of the gut microbiota. In a leptin-deficient (ob/ob) obese mouse model, Ley and colleagues used 16S rRNA gene sequencing to find a large rise in Firmicutes levels and a decrease in Bacteroidetes phylum abundance [49]. A few months later, Turnbaugh from the same group used the shotgun metagenomics sequencing technique to demonstrate that the cecal bacterial DNA of this obese murine model had a higher Firmicutes vs. Bacteroidetes ratio than that of lean, healthy mice. In comparison to control mice, ob/ob mice also showed greater concentrations of Archaea in the cecal microbial population [50]. Deeper studies of gut microbiota in humans and other obesity models have been prompted by these changes in bacterial abundance. Consequently, additional research on obesity has linked it to a decrease in Bifidobacteria and an increase in some bacteria, such as Halomonas or Sphingomonas [51]. Even though healthy people's gut microbiota makeup is rather varied, low bacterial gene counts are linked to high levels of obesity, insulin resistance, and dyslipidemia—all of which are characteristics of obese patients [52]. Indicating a comparatively weak intestinal flora. Obese patients have also been found to have higher amounts of Firmicutes and a lower proportion of Bacteroidetes [53]. It was demonstrated, for example, that people with a Firmicutes/Bacteroidetes ratio of ≥1 were 23% more likely to be overweight than people with a ratio of <1 [54]. Additionally, it is important to remember that thinking solely in terms of bacterial phyla—that is, the Firmicutes/Bacteroidetes ratio—is essentially inaccurate. In fact, Faecalibacterium prausnitzii, one of the most prevalent bacteria in the Firmicutes phylum in the healthy human colon, is reduced in obesity, whereas Firmicutes, such as Clostridium, Lactobacillus, or Ruminococcus, are elevated [55]. There are differences even among certain bacterial genera, such as Lactobacillus. For example, Million and associates found that the stool of obese individuals had higher amounts of Lactobacillus reuteri (L. reuteri) and Lactobacillus gasseri (L. gasseri) and lower levels of Lactobacillus paracasei (L. paracasei) and Akkermansia muciniphila (A. muciniphila) [56]. Additionally, different species of Lactobacillus and Clostridium have been linked to women's insulin resistance [57]. Insulin resistance in women has also been connected to several species of Lactobacillus and Clostridium [58]. All of these findings point to a particular role for gut bacteria in the development or maintenance of obesity. No particular bacterial signature has been found in obesity, despite increased study efforts. The variety of results found in the populations under study may be reflected in the countries, dietary patterns, levels of physical activity, and methods employed to examine the gut bacteria makeup. Notably, numerous studies have documented quick changes in the composition of gut microbes after dietary changes [59]. Additionally, engaging in modest physical activity may result in positive changes to the gut microbiome, which could improve mental health [60]. Additionally, as people age, their gut flora becomes less diverse, which could lead to bias in clinical research [61]. Additionally, a high-fat diet and the dysbiosis that occurs with obesity lead to a decrease in the expression of the cystic fibrosis transmembrane receptor (CFTR) gene in mouse ileal enterocytes, which lowers the mucus density and increases intestinal permeability. These factors also contribute to an impairment in mucus production and an enrichment in species that disrupt the barrier [62]. As a result, a variety of circumstances might alter the gut microbiota's makeup, which can result in serious biases in analysis. Furthermore, the methods utilized to analyze the microbiota (qPCR, 16s rRNA sequencing, shotgun metagenomics) have advanced significantly and could be extrinsic factors contributing to the reported variety of results [63]. In clinical investigations, it seems crucial to carefully define the phenotype of obese individuals (context, lifestyle, anthropometry, medicine, and comorbidities) in order to minimize bias. Despite their potential for improvement, these investigations demonstrate the part gut bacteria play in the etiology of obesity. The following section discusses potential mechanisms by which gut bacteria may influence the pathophysiology of obesity.
The colon has the highest bacterial density in the human gastrointestinal tract. Carbohydrates and proteins from dietary components that remain undigested in the upper portion of the gut are the primary sources of carbon and energy [64]. For the gut microbiota to bioconvert these diverse substrates, a range of metabolic bacterial activities that produce an energy source and metabolites must be present. Bacterial metabolites are absorbed and then distributed to various organs, where they come into direct contact with host cells and can have a systemic and local impact on physiological processes. They may therefore have a major impact on the host's metabolic phenotype and increase the risk factors for a number of illnesses, including obesity. Of the 40–60 g of carbs that enter the colon daily, the majority are polysaccharides from grains, fruits, and vegetables [65]. Gut microbes break down non-digestible polysaccharides, commonly referred to as fiber. Microbes—likely anaerobes in the gastrointestinal tract—can ferment food and prevent the conversion of carbs by producing metabolites like SCFAs, thanks to a class of hydrolytic enzymes. The community of fibrolytic bacteria includes species from the genera Bacteroides, Roseburia, Ruminococcus, Bifidobacterium, Lactobacillus, and Eubacterium. Most colonic bacterial species exhibit fermentation and the subsequent synthesis of SCFAs, including acetate (produced by Bifidobacteria, for instance) [66]. Some Firmicutes species, including Roseburia spp., Faecalibacterium prausnitzii, and Eubacterium rectale and Hallii, produce butyrate [67] and propionate (for instance, produced by Bacteroides, Prevotella, and Veillonella) [68]. As a result, the makeup of the microbial populations determines the kind of SCFA [69]. A recent investigation found that the microbiota in the gut of obese people contains more catabolic genes, suggesting a greater ability to get energy from food (and, in turn, to produce more SCFAs) than that of non-obese participants [70]. Increased SCFA synthesis may give the host more calories, which could result in weight gain, according to experimental research conducted on obese humans and animals [71].
While only a tiny portion of these metabolites are eliminated in feces, the majority of generated SCFAs are rapidly absorbed by colonocytes. SCFAs change the colon's microbiota and lower the luminal pH, which promotes the growth of bacteria that produce butyrate. SCFAs, especially butyrate, contribute to anaerobic conditions by consuming oxygen and serving as a major energy source for the host colonocytes [72]. In actuality, butyrate and propionate have a dose-dependent ability to regulate proinflammatory activation of myeloid and epithelial cells, and they are more effective at lower concentrations than acetate and lactate [73]. The intestine, skeletal muscle, liver, and pancreatic organs all express G-protein-coupled receptors (GPRs) 41 and 43, which are ligands of SCFAs. It's interesting to note that these receptors, also known as free fatty acid 3 and 2 (FFA3 and FFA2) receptors, mediate leptin secretion in response to SCFA stimulation and are also found in white adipose tissue. This implies that the gut microbiota may have a remote impact on host physiology. While butyrate interacts with GPR41 (FFA3), acetate mostly binds to GPR43 (FFA2). GPR41 and GPR43 can both be bound by propionate [74]. Obesity may reduce the amount of SCFA that binds to these receptors, which could lead to hepatic lipogenesis and an energy imbalance [75]. Through a variety of ways, SCFAs may help regulate host homeostasis. Indeed, acetate and propionate may enhance fat oxidation and energy expenditure while decreasing lipolysis, according to experimental research conducted on obese humans and animals.
Furthermore, by influencing glucose homeostasis and lipid metabolism, acetate also enhances insulin sensitivity [76]. By modifying other anorexigenic hormones, SCFAs can also cause satiety in addition to the release of leptin. For example, butyrate stimulates the release of glucagon-like peptide-1 (GLP-1), an anorexigenic incretion generated by enteroendocrine L cells [77]. Similar to GLP-1, intestinal L cells create peptide YY (PYY) by activating GPR41 and 43 with SCFAs. PYY is primarily released during the postprandial phase and aids in the satiety process [78]. Obese persons have been found to have lower plasma GLP-1 concentrations than healthy people [79]. Similarly, compared to lean people, obese patients produce less PYY [80]. Gut dysbiosis has been linked to incretion impairment in obesity and its correlation with type 2 diabetes [81]. However, acetate can also enter the brain and directly affect the hypothalamic circuits, causing agouti-related peptide (AgRP), an orexigenic neuropeptide, to have its mRNA expression decreased and α-melanocyte-stimulating hormone (α-MSH, an anorexigenic neuropeptide) to have its mRNA expression increased [82]. Lastly, the abundance of Bacteroides and Prevotella levels, which are both elevated in the microbiota of obese patients, was positively connected with the plasma concentration of the orexigenic hormone ghrelin [83]. And had a negative correlation with Lactobacillus and Bifidobacterium abundance [84]. The contradiction between the elevated fecal amount of SCFAs and the ineffective satiety signaling in obesity requires more research into the metabolic function of SCFAs. For example, it has been proposed that obesity may reduce the ability of SCFAs to bind to their receptors, which could lead to hepatic lipogenesis and an energy imbalance [85, 86]. It's also important to remember that elevated fecal SCFA concentrations may be a sign of either increased SCFA production or decreased absorption [87]. This might not accurately represent the host's complete availability [88]. For instance, compared to control mice, obese diabetic mice had much reduced overall plasma concentrations of SCFAs [89, 90]. Furthermore, one study discovered that, in contrast to circulating SCFAs, the quantities of SCFAs in feces were not linked to human insulin sensitivity, lipolysis, or GLP-1 levels [91]. A recent meta-analysis found that "compared to the non-obese subjects, obese individuals had significantly higher SCFA concentrations of butyrate (SMD = 0.78, 95% CI = 0.29–1.27) in feces, propionate (SMD = 0.86, 95% CI = 0.35–1.36) in feces, and acetate (standardized mean difference (SMD = 0.87, 95% CI = 0.24–1.50) in the blood and feces)." As previously mentioned, the release of leptin from mesenteric adipocytes is one way that circulating acetate contributes to anorexigenic effects. Despite the fact that leptin levels are higher in obese individuals, leptin resistance reduces the effectiveness of leptin's anorexigenic impact [92, 93]. According to a different study, non-digestible carbohydrates in the diet encourage the development of L cells in the rat colon [94].
The pathophysiology of obesity and its associated comorbidities, including insulin resistance and the ensuing cardiovascular disease, has been linked to low-grade inflammation [95] and T2D [96]. By a variety of methods, gut dysbiosis can exacerbate low-grade inflammation. First, it is widely known that Gram-negative bacteria emit lipopolysaccharide (LPS), which can penetrate the intestinal epithelium via entering chylomicrons or through broken tight junctions [97]. Tight-junction protein structures are also altered by changes in the gut microbial composition associated with obesity and a high-fat diet (HFD) [98], resulting in improved LPS passage [99]. The CD14 receptor is activated when LPS interacts with the LPS-binding protein (LBP) in the systemic circulation. The latter attaches itself to the toll-like receptor 4 (TLR4) on macrophages in various organs, including the liver and adipose tissue. Macrophages infiltrate adipose tissue as a result of the robust expression of genes encoding proinflammatory agents (factor nuclear Kappa B; NF-κB) brought on by this gut bacteria TLR4 activation [100]. When compared to saline-infused animals, LPS infusion replicates the characteristics of HFD-fed mice in terms of weight gain, visceral and subcutaneous adiposity, elevated fasting glycemia, insulinemia, liver triglyceride content, and body weight [101].
Aside from its impact on satiety, SCFAs increase the expression of important adipogenesis mediators called peroxisome proliferator-activated receptors (PPARs) [102]. Other studies have shown that butyrate and propionate, but not acetate, can speed up lipolysis in vitro by blocking histone deacetylase (HDAC) [103]. Furthermore, gut flora seems to have a significant impact on fatty acid oxidation. The liver and skeletal muscles of germ-free mice given an HFD actually had higher levels of phosphorylated adenosine monophosphate kinase (AMPK) than mice raised normally and given an HFD. Additionally, these germ-free mice gained significantly less weight than conventionalized mice. Actually, AMPK is a crucial enzyme that plays a big role in energy management. Increased AMPK levels lead to stronger fatty acid oxidation [104], and the inhibition of this enzyme by the gut microbiota promotes the production of triglycerides and cholesterol, which raises lipogenesis and causes obesity by storing excess fat [105]. O'Neill and colleagues discovered that obesity is associated with lower AMPK activity without altering AMPK expression in a large-scale population [106]. It is intriguing to consider that a certain "obesogenic" gut microbial makeup may reduce AMPK function and raise the host's susceptibility to obesity [107]. Another protein implicated in the obesity process, fasting-induced adipose factor (FIAF), also called angiopoietin-like 4 protein (ANGPTL4), was suppressed when recipient germ-free animals were given gut microbiota from conventionally grown mice. This implies that triglyceride buildup in adipose tissue may be restricted by the microbiome [108]. The liver, adipose tissue, skeletal muscle, and gut all produce FIAF/ANGPTL4 in response to fasting. The main job of FIAF/ANGPTL4 is to inhibit lipoprotein lipase (LPL), which lowers triglyceride accumulation in adipocytes [109]. On the other hand, intestinal FIAF inhibition increases LPL activity, which in turn stimulates fatty acid intake. Nevertheless, there is ongoing discussion over the ultimate impacts of various microbiome compositions on the stimulation or inhibition of FIAF [110]. It requires more research to verify the significance of this pathway for the gut microbiota's control of fat storage
The breakdown and absorption of fatty acids in the small intestine depend on the bile acids generated by the hepatocytes, among other factors. Hepatocytes produce the two primary bile acids, chenodeoxycholic acid (CDCA) and cholic acid (CA), from the breakdown of cholesterol. These acids are then excreted in the bile as conjugates with taurine or glycine. In the intestinal lumen, the gut microbiota deconjugates, dehydrates, and dehydroxylates CA and CDCA to produce deoxycholic acid and lithocholic acid, respectively. After being reabsorbed farther down in the ileum by both active and passive diffusion, these secondary bile acids are returned to the liver via the portal vein [111]. Therefore, it is expected that the distribution and pool of bile acids will be impacted by changes in the composition of gut bacteria. Swann et al. found that mice's distinct gut microbiota makeup affected their bile acid profile and energy metabolism [112]. Additionally, bile acids can bind to the nuclear Farnesoid X receptor (FXR), which is involved in the liver's metabolism of lipids and glucose [113], hence promoting metabolic liver dysfunction, which leads to obesity, insulin resistance, and non-alcoholic fatty liver disease (NAFLD). In fact, NAFLD occurred when recipient germ-free animals were given the gut microbiota of HFD-fed mice, leading to hepatic lipid levels that were similar to those of donor mice [114]. Furthermore, G-protein-coupled bile acid receptor 1 (GPBAR1), also known as TGR5, is abundantly expressed throughout the intestine, particularly in the colon and ileum, and can be activated by bile acids. TGR5 activation contributes to glucose homeostasis by producing GLP-1 [115]. Interestingly, bile acid profiles are changed in people with obesity, T2D, and NAFLD [116]. Generally speaking, obesity, type 2 diabetes, and non-alcoholic fatty liver disease seem to be positively connected with elevated plasma bile acid levels. Through additional signaling pathways (such as GLP-1 expression or enzyme modulation), gut microbiota may also affect bile acid metabolism and ultimately host metabolism (thermogenesis), ultimately leading to an elevated risk of obesity [117]. The identification of dysbiosis in a number of diseases, including obesity, through gut microbiota analysis has sparked interest in the creation of treatment plans based on intestinal microbiota reshaping. Therefore, traditional probiotics, also known as first-generation probiotics, are often derived from fermented foods and have been recommended based on the differences in gut microbial composition between patients and healthy volunteers. Numerous naturally occurring beneficial bacteria have been recognized as potential probiotics in this setting. More recently, new technologies that identify particular changes during obesity or mechanistic investigations that show mechanisms of action helpful for insulin sensitivity or food intake regulation have brought attention to novel probiotic candidates, also known as next-generation probiotics [117].

Figure 1: The pathophysiology of obesity is influenced by environmental and genetic factors and includes hormonal dysregulation, chronic inflammation, and alterations in the intestinal microbiota. Energy imbalance, influenced by dietary patterns and metabolic responses, leads to weight gain. Leptin, ghrelin, and insulin are key hormones for energy homeostasis and appetite. Moreover, intestinal dysbiosis exacerbates metabolic disorders, emphasising the complexity of obesity [436].
A. Nutraceuticals Targeting Appetite and Satiety
Dietary fibers are carbohydrates that human stomach enzymes are unable to break down [118]. Their physical characteristics within the digestive system are linked to their main modes of action.
It is a viscous, water-soluble fiber from the psyllium seed of the Plantago ovata plant. It is less readily fermented, and hence it might not induce bloating or other GI-related dysfunction, and it is highly prescribed for weight loss, lower CVD risk, and hypertensive and hypolipidemic properties [120].
Anti-obesity mechanism: Increase gastric transient time (delay gastric emptying) and favor satiety (alter Gut-Brain Axis) by upregulating GLP-1/2 and CCK hormones as well as inhibiting ghrelin secretion. Possess a lesser glycemic index and hence revert insulin resistance and enhance the thermogenesis process to maintain energy homeostasis. [121, 122] Similar to probiotics, it can also produce SCFA by fermentation as they indirectly act as prebiotics and thus bind to PPAR to exhibit lipolysis by upregulating the activity of LPL as well as improve insulin sensitivity [119].
Glucomannan, which comes from the Amorphophallus konjac tuber, is well-known for its remarkable capacity to absorb water, which helps with weight loss by improving satiety and postponing stomach emptying [123, 124].
Oats are obtained from a cereal plant, Avena sativa, family Poaceae. It is high in protein, lipids, vitamins, and minerals. In addition, oats have been regarded as a functional food due to the increased content of β-glucan (soluble fiber). Several studies have established that the intake of oats is inversely related to CVD risk. Also help reduce lipids and manage hypertension and hence reduce the risk of the metabolic disorder. [126] But few studies are conducted to study anti-obesity activity compared to psyllium, but several trials were conducted with oats against hyperlipidemia and hyperglycemia. β-glucan is the active constituent of oat bran that is accountable for several biological properties, such as antioxidant, anti-inflammatory, hypolipidemic, hypocholesterolemia, and hypoglycemic [127].
Anti-obesity action: β-Glucan-rich oats may increase gastric emptying and raise bile acid excretion and thereby modulate cholesterol homeostasis (HMG-CoA reductase). β-Glucan is known to raise postprandial CCK and PYY hormones and reduce insulin response and thereby suppress appetite [128, 129]. Like psyllium, they can also yield SCFA through fermentation, since they indirectly serve as prebiotics and bind to PPAR to promote lipogenesis by increasing LPL activity [125].
The biological plausibility of observational associations is supported by the antihyperlipidemic, antihypertensive, anti-hyperglycemic, antioxidant, anticancer, anti-inflammatory, antiobesity, and neuroprotective properties of soy proteins and soy isoflavones. Clinical trial data clearly show that soy protein ingestion lowers human blood cholesterol [130].
Garcinia cambogia is a non-official anti-obesity (appetite suppressant) plant widely cultivated in the majority of Southeast Asian countries like India, Nepal, and Sri Lanka. Garcinia cambogia belongs to the Clusiaceae family, and for decades its fruits have been employed in traditional medicine for the treatment of constipation and hemorrhoids [131]. Its main active phytocomponent is hydroxycitric acid (HCA), garcinol. Both garcinol and HCA have been reported to exhibit a wide range of biological activities, including antioxidant, anti-inflammatory, anti-hyperlipidemic, anti-diabetic, and anti-obesity activities [132, 133]. HCA, however, is extremely concentrated in the anti-obesity activity.
Anti-obesity mechanism: Indirectly inhibit the production of Acetyl Co-A and mitochondrial enzyme citrate lyase and thereby halt the process of lipogenesis. Enhance the degree of availability of serotonin and thereby suppress the appetite as well as regulate adipocyte differentiation by way of the mammalian Target of Rapamycin (mTOR) pathway. [134, 135] Further, it can regulate carbohydrate (glycolysis and glycogenesis) and lipid metabolism (altering lipid-metabolizing enzymes), both oxidation and synthesis, via upregulation of AMP-related protein kinase (AMPK) and serine protein kinase B/phosphatidylinositol-3-kinase (Akt/PI3K) pathways [136].
B. Nutraceuticals Enhancing Energy Expenditure and Thermogenesis
Curcumin, green tea extract, psyllium fibre, and omega-3 fatty acids are among the compounds that have demonstrated encouraging results in weight management through their ability to control hunger, improve insulin sensitivity, increase metabolism, and decrease inflammation [137].
Camellia sinensis, a member of the Theaceae family, is utilized to prepare various teas. Green tea is prepared by mild oxidation of Camellia sinensis leaves (herb). Green tea is the most widely used beverage after water worldwide, and therefore great attention was provided by a lot of researchers [138]. Several investigators have established that catechins are in very high concentration in green tea, and epigallocatechin-3-gallate (EGCG) is the predominant catechin responsible for most of the biological activities, such as anti-inflammatory, antioxidant, anti-cancer, anti-diabetic, and anti-obesity (thermogenic) as well as cardioprotective and neuroprotective activities [139, 140].
Anti-obesity mechanism: Raise the level of GLP-1 and enhance insulin resistance, pancreatic lipase inhibitor, enhance thermogenesis, enhance satiety (promote serotonin/dopamine uptake through modification of the gut-brain axis), and reduce protein expression of insulin resistance-linked adipokine resistin through the extracellular signal-related kinase (ERK½) signaling pathway and the NF-κB pathway [141,142] It also increases fat oxidation (β oxidation), blocks intestinal absorption of glucose, increases glucose uptake, increases glycolysis/glycogenesis enzymes through the AMPK/PPAR pathway, and enhances fecal excretion of lipid [143, 144].
Capsicum, commonly called chili pepper, is a common spice in many different cuisines. It has a distinct flavor, color, and biological properties that are good for your health. Capsaicinoids—which include capsaicin, dihydrocapsaicin, homocapsaicin, and nordihydrocapsaicin—are among the several health advantages of cayenne chili peppers. These substances have anti-inflammatory, anti-cancer, anti-obesity, and analgesic (painkiller) properties [145–147].
Anti-obesity mechanism: The capsicum (capsaicin/dihydrocapsaicin) increases energy expenditure via SNS in brown adipose tissue (BAT) or exhibits thermogenic properties by positively regulating several mitochondrial uncoupling proteins (UCP2 and 3) [148]. It has also been demonstrated that capsicum suppresses adipogenesis, induces pre-adipocyte apoptosis, and controls adipocyte differentiation through altering c-Jun N-terminal kinases (JNK), extracellular signal-regulated kinases (ERK½), AMPK, and the NF-κB signaling pathway. Capsicum is well documented to enhance the production of adiponectin (via upregulating PPARα) and upregulate the mRNA expression of hormone-sensitive lipase (HSL) [149, 150].
Caffeine is another substance that could aid in managing obesity. Coffee consumption has been found to be negatively correlated with the prevalence of metabolic syndrome [151]. Coffee-drinking participants, regardless of gender, had better anthropometry results and consumed more calories overall. Additionally, there is evidence that consuming one to four cups of coffee can lower the risk of developing cancer [151]. However, excessive consumption of coffee might raise blood pressure. Patients with the G allele of the gene COMT should avoid raising their blood pressure by consuming no more than 3 mg of caffeine per kilogram of body weight each day [152, 153]. Thus, it remains difficult to rule out the possibility of interindividual variation in the response to bioactive components, and the study's findings cannot be extrapolated without the proper patient follow-up [154].
C. Nutraceuticals Modulating Lipid Metabolism and Adipogenesis
Fatty acids that contain many double bonds make up polyunsaturated fatty acids (PUFA). Docosahexaenoic acid (DHA), eicosapentaenoic acid (EPA), conjugated linolenic acid (CLA), and arachidonic acid (ALA) are the main PUFAs. Nonetheless, ALA, DHA, and EPA are categorized as omega-3 fatty acids (ω-3 FA) and have been shown to have a variety of biological characteristics. 155 Rich in ω-3 FA, flaxseed and fish oil (salmon) are the main sources of ALA and CLA. The ALA/CLA and ALA/DHA/EPA found in flaxseed and fish oil, respectively, make them useful foods. ALA, CLA, DHA, and EPA exhibit a variety of advantageous qualities, such as immunomodulatory, antithrombotic, anti-inflammatory, anti-diabetic, anti-obesity, anti-hyperlipidaemia, anti-arrhythmic, and antioxidant effects.[156, 157]
Anti-obesity mechanism:
Curcuma longa, or turmeric (rhizome), is a common spice in the tropics widely applied as a colorant (yellow) and for flavoring, especially in Indian dishes. Turmeric has found application in Chinese and Indian food for decades because of its medicinal properties, such as anti-stress, antidepressant, antimicrobial, and dermaprotective activity. [160] In recent times, turmeric has been applied in Western and Middle Eastern food due to its biological characteristics and as commercial functional food/nutraceutical products. Curcuminoids (curcumin, bisdemethoxycurcumin, and turmerin) are the major active components of turmeric. [161] Turmeric (tetrahydro-curcumin active metabolite) has several therapeutic activities, such as antioxidant, anti-inflammatory, anti-apoptotic, anti-hyperlipidaemic, anti-obesity, anti-atherosclerotic, anticancer, and anti-diabetic activities. [162, 163].
Anti-obesity mechanism: It has strong antioxidant (upregulating Nrf2 signalling pathway), anti-inflammatory, anti-hyperlipidaemic (downregulating SREBP, LXR), and thermogenic (upregulating UPC1, PGC-1α) activities. Besides, it inhibits differentiation-adipogenesis conversion of pre-adipocytes into adult or mature adipocytes, as well as inhibits pre-adipocyte proliferation through the AMPK-PPAR signalling pathway. Also, it enhances lipolysis (reduced FFA circulation), inhibits lipogenesis, and increases the apoptosis of adipocytes through the MAPK and ERK ½ pathways [164-166].
Resveratrol is a polyphenolic stilbene that is a member of the phytoalexin superfamily. Red grapes (red wine), pomegranates, and berries are the main food sources of resveratrol. [168] The antioxidant, anti-inflammatory, and hypolipidemic properties of resveratrol have been utilized to treat a number of conditions, including diabetes, cardiovascular disease, cancer, and neurological disorders. [169]
Anti-obesity mechanism: Boost GLP-1 levels to lower blood glucose levels, prolong stomach emptying (which changes the gut-brain axis), and increase food intake. [170] apoptosis in matured adipocytes and adipogenesis inhibition in conjunction with quercetin. [161] Downregulate the expression of the genes for leptin, resistin, FAS, and ACC that are linked to insulin resistance by inhibiting the expression of different signaling molecules such as steroid regulating element binding protein 1c (SREBP-1c), liver X receptor (LXR), and PPAR. This is achieved by downregulating toll-like receptor 2 (TLR2). [172] Furthermore, it has been observed that resveratrol increases leptin sensitivity by downregulating the NF-κB pathway and improves thermogenesis by activating the AMPK signalling system. [167, 173]
A flavonoid (flavanol), quercetin is frequently found in fruits and vegetables such as berries, apples, grapes, and onions. Aglycone and glycosidic forms of quercetin are both accessible; rutin is the most prevalent glycosidic form. [174] Along with its cardioprotective, neuroprotective, and hepatoprotective qualities, quercetin has anti-inflammatory, anti-hyperlipidaemic, anti-hypertensive, anti-cancer, and anti-diabetic qualities. [175, 176]
Anti-obesity mechanism: Antioxidants (through nuclear factor erythroid-derived 2-like 2, or Nrf2 pathway) reduce oxidative stress; anti-inflammatory (by downregulating the NF-κB pathway); hypolipidemic; thermogenesis (by upregulating UPC-1 and PPAR gamma coactivator 1 alpha, or PGC1α); improve insulin sensitivity by raising adiponectin levels; lower nitrate levels (iNOS); reduce lipid metabolizing enzymes such as fatty acid synthase (FAS) and acyl-CoA carboxylase (ACC); and inhibit adipogenesis by inhibiting the mRNA expression of PPARγ, CCAAT-enhancer binding protein alpha (C/EBPα), and LPL. [177] Also, use the mitogen-activated protein kinase (MAPK; negatively regulated) and AMPK (positively regulated) signaling pathways to trigger apoptosis (mature adipocytes) and glycolysis (carbohydrate metabolism). [ 178, 179]
L-carnitine, a conditionally essential nutrient [180] playing an important role in carbohydrate and lipid metabolism [181, 182], has been extensively ingested as an OTC weight loss agent because of its claimed health-beneficial effects, such as potential anti-obesity [183, 184], antidiabetic [185], and lipid-enhancing activity [186, 187]. Evidence has documented L-carnitine's weight-reducing efficacy [183,184]; furthermore, earlier research showed the beneficial effects of L-carnitine on cardiometabolic risk factors, such as lipid [186,188] and glycemic indexes [185,189], perhaps by enhancing fatty acid ß-oxidation [180,190]; augmenting energy expenditure through regulating the acetyl-CoA/CoA ratio [191], thereby enhancing insulin sensitivity and stimulating the glycolytic pathway [180,182]; or activating adipocyte lipolysis, as well as inhibiting adipogenesis in adipocytes, through the regulation of lipolytic/adipogenic gene expression [192,193].
In addition, the essential contribution of gut microbiota dysbiosis as an underlying cause of obesity has raised tremendous attention [194-196]. Metabolic disorders, including obesity and its associated complications, have been correlated with changes in gut microbiota diversity and composition, according to evidence [195]. Gut microbiota is thus seen as a potential therapeutic target to improve dysbiosis-induced metabolic disorders, i.e., obesity [197].
Anti-obesity mechanism: Various possible mechanisms are suggested for ameliorative effects of pro/pre/synbiotics on anthropometric/metabolic parameters, such as, but not restricted to, regulating gut microbiota dysbiosis and hence inhibiting adipogenesis and promoting lipid oxidation [198]; enhancing short-chain fatty acid (SCFA) production [199-201], thereby correcting energy homeostasis and fat accumulation through increasing fatty acid oxidation [198]; improving glucose homeostasis and inhibiting insulin resistance [199, 201]; and eventually inhibiting gut permeability and metabolic endotoxemia, hence disrupting proinflammatory signaling pathways [202, 203].
D. Nutraceuticals Targeting Inflammation and Oxidative Stress
Nutraceutical interventions have become well-known as successful substitutes for standard therapies, which have not been very successful in addressing complex metabolic problems. By strengthening the body's natural antioxidant defenses and lowering the generation of reactive oxygen species, polyphenols, resveratrol, and antioxidants like vitamins C and E have been demonstrated to reduce oxidative stress in metabolic diseases. (ROS).
As potent antioxidants, vitamins C and E have been extensively discussed in the literature on oxidative physiology. An increasing amount of evidence demonstrates their value in preventing oxidative stress and its related clinical symptoms [204, 205]. Together, ascorbic acid (the water-soluble form of vitamin C) and alpha-tocopherol (the primary fat-soluble form of vitamin E) shield endothelial cells, which are structures that frequently malfunction in response to metabolic insults and are a major indicator of endothelial pathology [206]. Vitamin E inhibits oxidative instability of the lipid bilayer, while vitamin C neutralizes reactive oxygen species that are present in the cytosol [207]. When reactive oxygen species and antioxidant treatments are out of balance, endothelial cells are vulnerable to both structural and functional degradation [208, 209]. Antioxidant vitamins therefore provide enormous therapeutic promise for the treatment of endothelial dysfunction.
Polyphenols are among the most researched nutraceutical agents and can be found in large quantities in a wide range of foods and beverages, such as fruits, vegetables, tea, and red wine.
Plants contain polyphenols, which have a variety of biological functions. In order to reduce the production of ROS, they either bind trace elements that contribute to the formation of free radicals or block the enzymes that create them. Moreover, they stimulate the body's antioxidant defenses and actively scavenge ROS. Particularly, polyphenols target enzymes that are essential for the production of ROS, such as glutathione S-transferase, mitochondrial succinoxidase, microsomal monooxygenase, and NADH oxidase.
Ubiquinone, another name for coenzyme Q10 (CoQ10), is a fat-soluble, vitamin-like molecule that is found naturally in all of our body's cell membranes. This enzyme is also produced endogenously, but it is also a regular part of our food. It is necessary for the synthesis of energy within cells. It is also an effective antioxidant [210].
Mechanism of action:
E. Nutraceuticals Modulating Gut Microbiota
Probiotics operate by three central mechanisms of action in obesity treatment: antagonistic impact on the development of pathogenic microbiota and competitive adhesion to the epithelium and intestinal mucosa and diminished intestinal permeability and enhanced production of the intestinal mucus layer (barrier function), and modulation of the gastrointestinal immune system (immunomodulation) [213].
The probiotic strains of bacteria Bifidobacterium longum, Lacticaseibacillus casei, Levilactobacillus brevis, Lacticaseibacillus rhamnosus, Lactobacillus delbrueckii, Lactobacillus helveticus, Lactococcus lactis, and Streptococcus thermophilus can contribute to weight loss among obese persons through mechanisms of action that vary widely [212, 213]. These strains are able to modulate the fat metabolism, maximizing their degradation, decreasing the absorption from the intestine, excluding them from storage in adipose tissue, and enhancing their utilization as a source of energy [214]. Another interesting effect is the capacity to modulate the intestinal inflammatory response, decreasing low-grade intestine inflammation involved in obesity, and this can be beneficial for metabolic control and body weight regulation [215]. In addition to this, probiotic strains can influence satiety and hunger signals by regulating the release of hunger-related hormones, including ghrelin, which enhances feelings of fullness. Consequently, these mechanisms can curtail the urge for high-calorie and unhealthy foods [216].
Probiotics are living bacteria that live in the host intestine and are responsible for the healthy system of the host. While prebiotic (inulin, fructans, and fructose/galacto-oligosaccharides food ingredients) non-digestible components promote probiotic (bacteria) growth and lead to healthy intestinal microbiota and are therefore classified as functional food. Primarily Bifidobacterium and Lactobacillus spp. (multiple strains) are the most frequently cited probiotic bacterial strains and are termed beneficial bacteria, which live in the gut (microbiota). The co-administration of both pre- and probiotics is known as "synbiotic" and accordingly assists in enhancing the health status of the host. Both pre- and probiotics exhibit a wide array of pharmaceutical activities, such as anti-inflammatory, antioxidant, immunomodulatory, anti-cancer, anti-hyperlipidaemic, and anti-obesity.
Anti-obesity mechanism: Probiotics are capable of trapping cholesterol independently and have bile acid hydrolase activity and therefore help in the binding of cholesterol with deconjugated bile and excretion. Therefore, in two mechanisms, probiotics can control the cholesterol level either by excretion or utilization and hence indirectly reduce obesity and CVD risk. Probiotics convert oligosaccharides (galacto/fructo) into short-chain fatty acids (SCFAs) by the process of fermentation and activate PPAR and change the activity of the lipolytic enzyme lipoprotein lipase (LPL) and thus stop lipogenesis. In addition, SCFA increases GLP-2, PPY, and CCK production by activating POMC and leads to satiety as well as increased insulin sensitivity.
F. Nutraceuticals Improving Insulin Sensitivity and Glucose Metabolism
A potent antioxidant that the body naturally produces and that can be found in some foods is alpha-lipoic acid. Its ability to work in almost every part of the body due to its dual solubility in fat and water makes it special [217].
Mechanism: It has the ability to absorb glucose. GLUT4 transporters are more likely to translocate to the cell membrane when ALA is present. A protein called GLUT4 serves as a "doorway" for glucose to enter fat and muscle cells. More glucose can be taken up from the bloodstream when there is more GLUT4 on the surface. Moreover, antioxidant defense ALA shields the pancreas and other tissues from harm by lowering oxidative stress, which may assist in maintaining the function of beta-cells that produce insulin. [218] AMP-activated protein kinase (AMPK), a master regulator of energy metabolism, can also be stimulated by ALA. AMPK activation improves insulin sensitivity by increasing glucose absorption and fatty acid oxidation [217].
Ascophyllum nodosum and Fucus vesiculosus are edible brown seaweeds found at sea that have been eaten by coastal people in Asia, Britain, and other countries since ancient times [219]. Because they contain numerous bioactive chemicals, including polyphenolics, phlorotannins, and fucoidans [220, 221], these nutraceuticals are now proved to effectively treat metabolic diseases like obesity and type 2 diabetes [222, 223].
Mechanisms of Action: In vitro investigations indicated the possible hypoglycemic molecular effects of bioactive compounds contained in Ascophyllum nodosum and Fucus vesiculosus. These molecules can reduce blood glucose levels through (1) inhibition of carbohydrate digestive enzymes, α-amylase, and α-glucosidase, thereby slowing and reducing intestinal glucose absorption; (2) inhibition of the hepatic enzymes [glucose-6-phosphatase (G6Pase) and phosphoenolpyruvate carboxykinase (PEPCK)], stimulating glycogen synthesis and glucose uptake at the cellular level; and (3) activation of adenosine monophosphate-activated protein kinase (AMPK), acetyl-CoA carboxylase (ACC), and serine/threonine kinase (AKT), leading to an increase in the number of glucose transporter 4 (GLUT4) on the cell membrane and enhancing glucose uptake at the cellular level [224].
The family Lauraceae consists of the genus Cinnamomum and consists of Cinnamomum zeylanicum or Cinnamomum verum, which is also referred to as Ceylon Cinnamon, and Cinnamomum cassia or Cinnamomum aromaticum, commonly referred to as Chinese Cinnamon, and are regarded as the primary species. The latter is of poorer quality because of its weaker scent and darker color, and Ceylon cinnamon is brown in color with a softly perfumed smell and a warm, sweet flavor. Chinese cinnamon is different from Ceylon cinnamon also due to the presence of a greater amount of coumarin (0.8 to 10.63% for Chinese cinnamon and about 2% for Ceylon cinnamon), a compound which, if taken in large quantities, poses the risk of toxicity to the liver. Cinnamomum, aside from being added in food, is also employed to cure certain illnesses, including diabetes mellitus and obesity primarily because of the cinnamaldehyde (65–80%) and eugenol (70–95%) obtained from bark and leaves, respectively. Phenolic compounds such as quercetin, rutin, and catechins found in leaves and bark of Cinnamomum are other compounds possessing hypoglycemic activity [225].
Mechanisms of Action: Cinnamomum was demonstrated to enhance insulin sensitivity by means of multiple potential biochemical mechanisms, including (1) activation of GLUT4 location and expression; (2) increase in expression of insulin receptor (IR), insulin receptor substrate type 1 (IRS-1), and insulin receptor substrate type 2 (IRS-2) [226,227]; (3) enhancement of the activity of AKT and PI3K (phosphatidylinositol 3-kinase) [226,227]; and (4) increased activation of PPAR-α/γ [228].
The metabolism of fats and carbohydrates is influenced by this vital trace mineral. Numerous foods, including potatoes, broccoli, and whole grains, contain it. It is also a typical component of several blood sugar-supporting products. It is frequently promoted as a weight-loss supplement due to the fact that it is thought to improve the way insulin works, which can help control blood sugar levels. Reducing cravings and avoiding the "sugar crash" that frequently results in overeating are two benefits of stable blood sugar. Its usefulness as a strong appetite suppressant, however, is supported by conflicting and typically weak evidence [229]. A prior study showed that in overweight and obese people with type 2 diabetes, a combination of Cr and biotin could enhance glycemic management by lowering FBG and HbA1C [230].
G. Other Emerging Nutraceuticals for Obesity
Conjugated octadecadienoic acid is a class of conjugated linoleic acid isomers that are produced from linoleic acid. By biohydrogenating linoleic acid, microbes in ruminant animals' digestive tracts produce various types of CLA [233, 232]. Alkaline conditions are used to produce commercial formulations of CLA from the linoleic acid of sunflower or safflower oils.
After this kind of processing, a CLA combination with roughly 40% of the 9,11 isomer and 44% of the 10,12 isomer is produced [231]. Research has demonstrated that CLA has anti-obesity characteristics [232, 233]. CLA's use as a weight-loss aid has grown. Several studies on animals and some on humans have shown that supplementing with a CLA combination (i.e., equal amounts of the 10,12 and 9,11 isomers) or the 10,12 isomer alone reduces body fat mass (BFM) [232]. Of the two major isomers of CLA, the 10, 12 isomer specifically is responsible for the antiobesity effects [234-236].
Mechanisms
Adaptive thermogenesis, physical activity, and basal metabolic rate (BMR) all influence energy consumption. By increasing energy expenditure through enhanced BMR, thermogenesis, or lipid oxidation in animals, CLA has been suggested to decrease adiposity [238, 239-243]. It is unknown how CLA modulates BMR or LBM and how this helps people lose body fat or other body weight.
By inhibiting the expression of PPARγ, C/EBPα, sterol regulatory element binding protein 1c (SREBP-1c), liver X receptor (LXRα), and adipocyte fatty acid binding protein (aP2), CLA therapy has been shown to particularly decrease adipogenesis and lipogenesis [237, 245–249].
In human subjects, 10,12 CLA supplementation also increases the levels of inflammatory prostaglandins (PGs) [250, 244].
The scientific name for bitter melons is M. charantia, and they contain phytochemicals such as glycosides, saponins, phenolic constituents, fixed oils, alkaloids, reducing sugars, resins, and free acids, as well as nutritionally significant vitamins, minerals, and antioxidants [252]. Vitamin C is also abundant in the immature fruits, which also supply iron, phosphate, and vitamin A [252].
Bitter melon extracts may ameliorate high-fat-diet-induced obesity and hyperlipidemia in animal models. Most findings related to obesity and hyperlipidemia also showed that the plant extracts may modulate fat-metabolizing kinases such as AMPKs, genes, and nuclear factors like PPARs, LXRs, and PGC-1α in liver and skeletal muscle and affect adipocyte differentiation, while several review papers suggest the antidiabetic mechanism [251] and various pharmaceutical effects of the plant [252] and emphasize its efficacy and safety aspects.
Mechanisms for Obesity:
Seeds of the African mango tree, which are taken as a weight-loss supplement. Ethnomedicinal therapy involves the bark, kernels, leaves, or roots for treatment of different ailments [258]. The bark is blended with palm oil to treat diarrhea as well as to shorten the breastfeeding period. Shavings of the stem bark are taken orally to cure hernias, yellow fever, and dysentery and to alleviate the effects of poison in French Equatorial Africa. [259] The antibiotic activity of the bark cures scabby skin, and boiled bark cures toothache. [258] In Sierra Leone, the bark is ground into a paste with water by the Mende tribe and put on the skin for pain relief. [259], [260] In some areas of Africa, the bark extract is taken orally to cause an analgesic effect. [260] Powdered kernels serve as an astringent and are also used on burns. [259] The stems of the tree have been utilized as chewing sticks in order to clean teeth. [258]
There are several studies on the industrial possibility of African mango usage in food, cosmetic, and pharmaceutical products [261, 262, 263, 264]. Initiatives on phenotypic variation, amino acid profile [262], soil conditions [261, 263] and economical potential of the plant species report further commercial interest. The kernel oil can serve as a binder in food or pharmaceutical products [264] or industrial gum [265].
The pulp is utilized in the preparation of jam, jelly, and juice and is eaten as a dessert in western and central Africa. The farmers utilize the leaves as animal feed. The wood is utilized in the preparation of walking sticks and supports for roofing [258].
Mechanisms for Obesity:
Summary of Key Human Clinical Trials
Several clinical trials and meta-analyses involving thousands of subjects have evaluated the weight-reducing potential of numerous nutraceuticals in adults with overweight or obesity. Meta-analyses indicate that the average weight loss from nutraceutical supplementation is usually modest, typically between approximately 0.2 and 3.7 kg based on the particular nutraceutical, dosage, and study duration. Among the nutraceuticals, psyllium (mean difference ~ -3.7 kg), Nigella sativa (-2.1 kg), spirulina (-1.8 kg), chitosan (-1.7 kg), green tea extract (-1.3 kg), glucomannan (-1.4 kg), and curcumin (-0.8 kg) have yielded small but significant body weight reductions compared to controls or placebo. Nonetheless, the clinical relevance of such findings is controversial because the magnitude of weight loss is generally less than the 5% body weight reduction that is accepted as significant in the treatment of obesity. Control groups receiving lifestyle interventions also experience weight loss, making it challenging to separate the real efficacy of nutraceuticals. Various studies highlight significant heterogeneity in study designs, populations, intervention length, and study quality, resulting in variability. In general, despite the fact that some nutraceuticals can contribute modestly to weight loss as an adjunct to diet and exercise, they cannot substitute for extensive lifestyle or medical treatments of obesity [271].
Nutraceuticals have a variety of impacts on both lean mass and fat mass, which affect body composition in the management of obesity. The following information is revealed by clinical studies and meta-analyses:
Fat Mass Reduction: Among people who were overweight or obese, L-carnitine supplementation showed a statistically significant decrease in body weight (average -1.2 kg) and fat mass (-2.1 kg); however, no significant change was observed in waist circumference or body fat percentage. In recent randomized controlled trials, pyruvate and Gymnemasylvestre decreased body mass, waist-to-hip ratio, and overall body fat ratio [272]. [273] In individuals with obesity, the Mediterranean diet, when protein-enriched and energy-restricted, resulted in significant decreases in weight, visceral adiposity, and fat mass while maintaining lean body mass. [274]
Lean Mass Effects: There were no appreciable changes in body weight or body fat, and protein supplementation during endurance training had only a minor impact on lean body mass growth (SMD = 0.13, 95% CI: −0.01, 0.28; p = 0.07). The fifth lean mass (43.6 kg vs. 39.0 kg in controls) and appendicular muscle mass adjusted for weight were both improved by nutritional intervention, particularly with increased protein consumption, according to a 2024 RCT. Additionally; there was a notably lower percentage of fat mass. The positive change was supported by plasma branched-chain amino acids (BCAA), which correlated positively with lean mass and negatively with body fat. [275]. Other supplement meta-analyses, like those of branched-chain amino acids, revealed similar muscle mass outcomes for the intervention and control groups, with notable but mild effects in particular subgroups. [276].
Comparative Results: Most nutraceutical therapies reduce fat mass and perhaps spare lean muscle, especially when paired with strength training and sufficient protein consumption. Supplements like pyruvate and L-carnitine, as well as higher protein diets, are primarily responsible for the significant variations in fat mass reduction and lean mass preservation; extracts from licorice and capsicum, for example, showed neutral or non-significant effects on body composition [275].
Body composition improvements can be supported by nutraceutical techniques; however, the extent of the effects is usually small and frequently dependent on how well they are integrated with dietary and exercise changes.
Weight and BMI
Findings from a meta-analysis of 15 RCTs showed that, in obesity, treatment with 2.7*1010 Colony Forming Units (CFU)/day of Lactobacilli probiotics for 2–3 months reduced body weight (kg) by −0.54 (95% CI −0.83, −0.25; p < .001); when BMI (kg/m²) was used as a marker, reduction in the Lactobacilli arms was −0.43 (95% CI −0.67, −0.20; p = .005). Conversely, following probiotic supplementation, there was a slight gain in body weight in children (+0.20 kg; 95% CI 0.04, 0.36) and infants (+0.30 kg; 95% CI −0.01, 0.62; p = 0.05) [Citation92]. A further meta-analysis involving four RCTs failed to show any significant changes in body weight, BMI, and visceral fat of obese persons caused by probiotics [Citation 93].
Based on the results above, a null or weak (<3%) effect of probiotics on body constituents [Citation94], among obese individuals with heightened cardiovascular risk, probiotic supplementation reduced BMI by 0.52 kg/m² (95% CI −0.81, −0.25; p < .001) and waist circumference by −2.11 cm (95% CI −3.54, −0.68; p = .004) [Citation95]. Another work on this complex subject has been provided by a meta-regression analysis reporting that the effect of probiotics on BMI varies with intervention duration (≥ 8 weeks), number of probiotic species, and baseline BMI ≥ 25 kg/m², thus reflecting the effectiveness of probiotics in reducing BMI, especially in obese or overweight patients.
Evidence from controlled trials and thorough reviews indicates that nutraceuticals have a variety of effects on metabolic parameters, including blood glucose, lipids, and insulin sensitivity.
Glucose Regulation in Blood: Clinical studies have demonstrated that supplementing individuals with overweight and obesity with novel nutraceutical formulations, such as yeast β-glucan, prebiotics, and essential minerals, can maintain or marginally improve fasting glycemia, fasting insulin, and HOMA-IR values over a period of 90 to 180 days. [277] In numerous randomized trials, components of nutraceuticals such as chromium, berberine, and specific botanicals (such as bitter melon) have shown statistically significant improvements in overall glycemic management and decreases in fasting blood glucose. [278]
Improvement of Lipid Profile: In clinical settings, nutraceuticals containing bioactive substances like red yeast rice, berberine, policosanol, and specific plant-based fibers have been shown to continuously reduce LDL cholesterol, total cholesterol, and triglycerides. In some cases, these products have also been shown to improve HDL cholesterol [279]. The atherogenic index, a composite indicator of cardiovascular risk derived from the ratio of triglycerides to HDL cholesterol, has also been positively impacted by nutraceutical therapies.
Insulin Sensitivity: Clinical trials suggest that nutraceutical supplementation can enhance insulin sensitivity, as reflected by decreases in fasting insulin and the HOMA-IR index. This effect was seen in animal models as well as in humans during intervention times ranging from several months, particularly for multi-supplement products. [279] Adiponectin, a hormone associated with enhanced insulin sensitivity, is also often elevated after nutraceutical interventions, lending further support for metabolic health effects. [280] Probiotic ingredients in some nutraceuticals have proved to have more benefits on insulin and glucose metabolism by enhancing gut function and decreasing systemic inflammation. [278]
Figure 2: Representative figure of “Metabolic Disorders”, featuring conditions like diabetes type I and II, hyperlipidaemia, hypertension, and other diseases.
Additional Endocrine and Metabolic Factors: Nutraceuticals have also been demonstrated to positively affect liver function enzymes, lower C-reactive protein and other indicators of hepatic and systemic inflammation, and alter endocrine hormones in people with metabolic syndrome and obesity, in addition to the standard lipid and glucose markers [280]. A potential benefit in non-alcoholic fatty liver disease and a decreased risk of cirrhosis or fibrosis following nutritional supplements are indicated by improvements in ALT/AST ratios. In [277] Based on the nutraceutical, dosage, length of supplementation, and participants' preexisting health, different metabolic markers can improve to varying degrees. Nutraceuticals are frequently used as supplemental treatments in conjunction with dietary and lifestyle changes to improve metabolic health in obese and overweight people. [279]
Obesity is marked by induced, chronic low-grade inflammation as a consequence of the enlargement of adipocytes (hypertrophy) and by adipogenesis (hyperplasia) of visceral adipose tissue [282]. In the past, adipose tissue was reported to be the primary location of energy storage, protection of organs, and insulation from cold [283-285]. However, over the last decades this context has been altered due to the identification and understanding of the various functions of the adipose tissue. Adipose tissue is now recognized as a metabolically active endocrine organ that releases mediators and adipokines, makes contributions in cellular and tissue communication, and participates in the inflammatory processes on the local and systemic levels. [285] Adipose tissue is a heterogeneous tissue and consists mainly of adipocytes and preadipocytes, but other cell types are also found, such as fibroblasts, pericytes, macrophages, lymphocytes, neutrophils, and T cells [286]. The immune system cells, together with the adipocytes, are crucial for the upkeep of the physiology and metabolism of adipose tissue. [287].
In obesity, the macrophage infiltration in the adipose tissue is increased. In reality, there exists a great correlation between the macrophage amounts and adipocyte number and size. [288] The evidence obtained from murine models is that macrophages in lean mice make up about 5% of adipose tissue cells, while in obese mice, macrophages account for as much as 50% of all adipose tissue [289]. Adipose tissue macrophages display alternate phenotypes based on diverse conditions. In this regard, macrophages are typed as classically activated macrophages (M2), or anti-inflammatory phenotype, and alternatively activated macrophages (M1), or pro-inflammatory phenotype. [288]
The polarization of macrophage M0 (precursor) to M1 is done through the activation of the classical pathway where pro-inflammatory cytokines of type 1 T-helper cells like interferon-gamma (IFN-γ) and tumor necrosis factor alpha (TNF-α), along with components of bacteria like lipopolysaccharide (LPS), stimulate the production of pro-inflammatory cytokines like TNF-α (cytokine inducing lipolysis in the adipose tissue), interleukin (IL) 6, IL-1, IL-12, monocyte chemoattractant protein-1 (MCP-1), CXC chemokine ligand (CXCL) 1-3, CXCL-5, and CXCL8-10. [290-292]
M1 macrophages are primarily found during times of obesity and are associated with the development of type 2 diabetes and insulin resistance. On the other hand, type 2 T-helper cells create M2 macrophages, which are driven by cytokines such as IL-4 and IL-13. These cells also increase the expression of anti-inflammatory cytokines such as IL-1 receptor agonist (IL-RA), IL-10, IL-12, and arginase-1. [293]. Lean adipose tissue is where M2 macrophages are primarily found, as opposed to M1 macrophages.
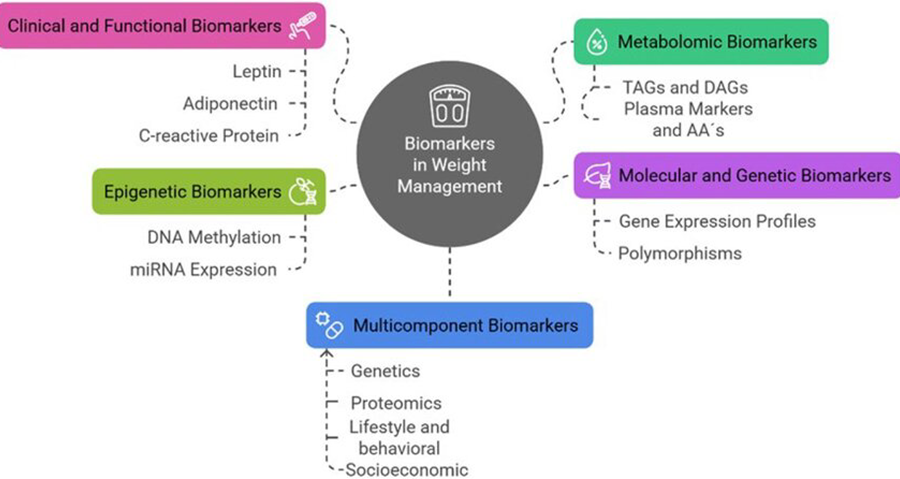
Figure 3: Novel and traditional biomarkers could assist in knowledge gaps on treatment variability and long-term adherence in the management of obesity and provide promising instruments for tailored strategies, improving precision medicine and enhancing results. TAGs: triacyclglycerols; DAGs: diacylglycerols; AA´s: amino acids; miRNA: microRNA [437].
There are several mechanisms in the process of developing obesity-induced inflammation, among which include hypoxia [294], augmented levels of free fatty acids (FFA) [295], LPS [296], reactive oxygen species (ROS) [297], and pro-inflammatory cytokines [298]. Yet, up to now, it is not certain what causes this inflammatory process. The interaction of the above factors with adipose tissue (hypoxia, FFA, ROS, pro-inflammatory cytokines, and LPS) leads to the transcription of the genes encoding for pro-inflammatory cytokines like TNF-α and IL-1β through the activation of transcription factors like NF-κB, hypoxia-inducible factor 1 (HIF-1), interferon regulatory factor 3 (IRF-3), and activator protein 1 (AP-1). Hypoxia and TNF-α suppress adiponectin (adipocyte-derived adipokine) production that, in non-obese individuals, is present in high levels, exhibits anti-inflammatory effects, and is associated with anti-atherosclerotic activity. [299]
Key Nutraceuticals with Anti-Inflammatory Effects
Clinical Aspects to Consider
Nutraceuticals typically have mild anti-inflammatory benefits that take time to show up in the body (usually 4–12 weeks or more).
Those with higher metabolic risk and baseline inflammatory indicators experience more severe effects.
Nutraceuticals may help reduce systemic inflammation and related metabolic dysfunction in obesity when used in conjunction with lifestyle changes like diet, exercise, and medication.
Limitation and challenges in clinical research of Nutraceuticals
Dietary clinical trials (DCTs) have been successfully prolonged throughout the last three decades to ascertain dietary needs and establish persuasive evidence for dietary guideline formulation. The DCTs, being "controlled changes in diet intakes or lifestyles in people in order to assess their possible impact on specific outcomes," establish cause-and-effect relationships and offer compelling evidence for actual clinical practice.
One of the greatest challenges in DCTs is a baseline exposure to the food under investigation and dietary history. Insufficient detail in the information regarding the background dietary intake and baseline status of participants restricts the generalizability of findings. In instances of nutrient supplementation, baseline dietary status (e.g., deficiency vs. adequacy of a nutrient) will decide the success of intervention. Also, background consumption of the food component will influence the result within the control group, particularly with the supplement administered in higher doses in foods as opposed to within pharmacological doses. The relevance of the study subjects' baseline nutritional status (normal-nourished versus malnourished) will be further emphasized in NCTs measuring the treatment effect of the intervention on hard clinical endpoints and survival, particularly in critical illness.
Many natural substances used in nutraceuticals have different potencies, compositions, and bioavailabilities based on how they are sourced, processed, and formulated. For clinical trials, this lack of standardization makes it more difficult to ensure consistency between batches and has an impact on the reproducibility of outcomes. Unlike pharmaceuticals, which are manufactured to strict quality standards, variability in active compounds in nutraceuticals can impact efficacy assessment [304].
Rather than having distinct, singular pharmacological targets, nutraceuticals typically have complex, nuanced impacts. Selecting accurate, validated biomarkers or clinical objectives becomes challenging as a result. Effects are frequently mild, subject-specific, and lifestyle-related, which makes trial design and interpretation even more challenging [305].
The positive expectations that participants have for "natural" products sometimes result in high placebo reactions. Nutraceuticals that have unique tastes, scents, or looks may be challenging to blind. These elements make it more difficult to discern real effects from placebo and raise the danger of bias [304].
Many nutraceuticals consist of complex mixtures or are part of multi-ingredient supplements, making it difficult to attribute observed outcomes to specific components. Interactions between different nutraceuticals or with diet can confound effects. Unlike single-compound drugs, the food matrix and co-nutrient interactions introduce complexity in study design and interpretation [304].
Generally healthy or mildly ill people are frequently recruited for nutritional trials, which dilute quantifiable effects. Response heterogeneity is increased by significant variation in genetics, lifestyle, gut flora, and baseline nutritional condition. Due to the requirement that participants maintain lifestyle factors that impact findings, recruitment and retention might be difficult [304].
Because of financial and practical limitations, nutritional research typically has shorter trial durations, which makes it more difficult to evaluate long-term safety and efficacy. Many chronic condition benefits require extended observation periods, which are rarely met in nutraceutical trials [305].
National regulations governing nutraceuticals vary greatly and are frequently less strict than those governing pharmaceuticals. This diversity makes it difficult to construct trials that satisfy various foreign marketing claims and compliance criteria [305].
Nutraceutical trials frequently base outcomes on subjective results and self-reporting, thereby enhancing bias and variability. Inefficient randomization, absence of double-blinding, limited sample size, and incomplete statistical reporting are frequent methodological flaws [305].
These contribute to lowering the strength and the generalizability of evidence. Overall, nutraceutical clinical research is confronted with several inherent and practical limitations—variance in ingredients, sophisticated interventions, and methodological issues to regulatory divergence and placebo responses. Meeting these necessitates strict quality control, properly crafted protocols with correct biomarkers, proper blinding, proper sample size, more extended study duration, and lifestyle factor control in populations. These issues account for why consistent, high-quality evidence for the efficacy of most nutraceuticals continues to be limited and why trial design and standardization continue to improve.
The most widely utilized nutraceuticals include fruit and vegetable compounds. They have been suggested to offer protection against a number of chronic illnesses, such as diabetes, cancer, osteoporosis, and cardiovascular disease. They are often substances with anti-inflammatory or antioxidant properties [306]. Plant pigment flavonoids, especially anthocyanins in berries, flavonols in dark chocolate, polyphenols like resveratrol in red grapes, catechins in tea, and quercetin, are widely consumed nutraceuticals. Too little information reveals that all of these compounds can be cytotoxic. Nonetheless, epigallocatechin gallate metabolites, the active catechol found in green tea extract and what is believed to be imparting the antioxidant properties of green tea, are thought to increase oxidative stress and are implicated in liver injury [307]. Neither is it altogether self-evident that the intake of one of these dietary supplements has any actual health advantages, considering that there have been no big clinical examinations [306]. The soy-based daidzein metabolite equol and the isoflavones genistein and daidzein are the nutraceutical flavonoids most intensively studied. As opposed to other flavonoids, the purified form of the isoflavones has been found to exhibit estrogenic activities in vitro and in animal models, including causing uterine hypertrophy or malformations of the reproductive tracts, small sizes of testes, inhibition of androgens, thereby causing sterility, and proliferation effects of estrogen-dependent tumors [309-316].With the advent of evidence that has shown the health hazards that occur after undertaking hormone replacement therapy in women after menopause, menopausal women have resorted to taking dietary supplements to address some symptoms that they experience, such as hot flashes, depression, and loss of bones. Up to 42% of these women may have been taking soy products, such as extracts of isoflavones and refined isoflavones like genistein, according to recent surveys [307]. These have the ability to reach far greater quantities in the plasma than the isoflavones found in SPI or soy meals, which are a complex combination of over a hundred phytochemicals and bioactive proteins or peptides [317, 314]. Endometriosis cases have been seen in women who take supplements containing isoflavones [308], and, since the estrogenicity of the products seems so prevalent, a risk of development of estrogen-sensitive cancers in individuals consuming the products appears probable.
B. Recommended Dosages and Formulations
Suggested Doses and Formulations of Nutraceuticals in Obesity
The overview of significant nutraceuticals that are used to manage obesity is based on the data of systematic reviews and clinical experiments. The listed dosages represent the dosages applied in human studies with either clinically relevant or encouraging weight loss effects. [318]
Table 1: Dosages applied in human studies with either clinically relevant or encouraging weight loss effects [318]
|
Nutraceutical |
Recommended Dose |
Formulation |
Typical Duration |
|
Portulaca oleracea |
10g/day (seeds, powdered) |
Powder/Capsule |
8 weeks |
|
Garcinia cambogia |
300–2,800mg/day (HCA) |
Capsule/Tablet |
8–12 weeks |
|
Green Tea |
540–625mg/day (extract) |
Extract/Capsule/Tea |
6–12 weeks |
|
L-Carnitine |
1,000–2,000mg/day |
Capsule |
8–12 weeks |
|
Irving gabonensis |
150mg x2/day |
Capsule |
10 weeks |
|
Pyruvate |
50mg/kg/day |
Capsule/Tablet |
8–12 weeks |
|
Chitosan |
750–3,200mg/day |
Capsule/Tablet |
8–12 weeks |
|
Chromium |
400–1,000μg/day |
Capsule/Tablet |
12–24 weeks |
|
Gymnemasylvestre |
300–600mg/day |
Capsule |
8–12 weeks |
|
Turmeric (curcumin) |
500–1,500mg/day |
Capsule/Tablet |
8–12 weeks |
|
CLA |
3–4.5g/day |
Capsule |
8–24 weeks |
C. Regulatory Landscape for Nutraceuticals (e.g., FSSAI in India, FDA in USA, EFSA in Europe)
India
However, India has come to be a prospective international provider of nutraceutical ingredients, particularly phytochemicals; however, the nutraceutical idea remains obscure among Indian people, newborn to India. The Indian government passed the Food Safety and Standard act (FSSA) in 2006, which regulates foods, dietary supplements, and nutraceuticals. It includes major clauses in the Prevention of Food Adulteration Act 1954, and they are founded on international legislation and the Codex Alimentarius Commission [319]. In 2015, Food Safety and Standard Authority of India (FSSAI) framed regulations that are referred to as the Food Safety and Standards, 2015. They control production, marking, selling, packaging, distribution, and marketing of food or health supplements, nutraceuticals, foods of special dietary use, foods of special medical use, functional foods, and novel foods. Prior to this, the Food Safety and Standards Regulations, 2011 were introduced in India regarding nutraceuticals, functional foods, and dietary supplements [320]. Regulations of nutraceuticals are formulated in India, and when completed, it will increase foreign investment.
USA:
In 1994, the United States of America introduced DSHEA. DSHEA provided some leeway in the distinction between food and medicines, and under this act, the manufacturing firm has the responsibility to verify the safety of nutraceuticals before marketing, and once in the market, the FDA has the responsibility to act in case they are identified to be unsafe. In the USA, two primary federal food regulating organizations, the United States Department of Agriculture (USDA) and the FDA, emerge in the regulation, investigation, evaluation, inspection, and sanction. In 1862, USDA was formed with the aim of preventing the importation of adulterated food. In 1906, still further, Food It was laid down to meet the misbranded and adulterated food, drinks, and drugs under the Drugs Act. This was followed by the Food, Drug, and Cosmetic Act (FDCA), which was enacted in 1938 in an effort to control food, drug, and cosmetic safety. Since that time a lot of amendments have been done to the FDCA, and also other supporting laws regarding food safety have been adopted [321]. Both dietary supplement products, which are complete, and dietary regulations come under different sets of regulations by the FDA. Both should follow the current Dietary Supplement Good Manufacturing Practices (cGMPs) and the national and international manufacturing companies' quality control of the dietary supplements. The manufacturers are not required to have the premarket approval by the FDA to employ the structure/function claims. The manufacturer or distributor of the dietary supplement, however, is the one obliged to disclose the report of serious adverse effects of the product to the FDA [322].
Europe:
In the EU there is harmonization of food standards under the European Food Safety Authority (EFSA), established in 2002. It acts as an independent body in giving a piece of advice to the member states, in gathering the data to foresee risk, and in offering a scientific evaluation. Nevertheless, it does not deal with risk management. EFSA excludes foods made out of nutrients, e.g., vitamins, minerals, etc., known as food supplements, a subject matter of focus.
Proteins and vitamins will be present there. Directive 2002/46/EC [323] is the key regulation concerning food supplements in the EU. The EU has set up a list of restrictions based on allowed vitamins or minerals, and the marketing of the product not on the list must apply to the European Commission. European nutraceutical products must meet the stringent European development and quality standards that new products must meet. The products are known to be products of high quality. There are stringent regulations that deal with product assertions in Europe. But these rules are not similar in various countries of Europe. The nutrition companies in the EU formed Food Supplements Europe (FSE), which controls the quality of the products [324].
D. Quality Control and Standardization of Nutraceutical Products
Quality Control Measures
Standardization in Nutraceuticals for Obesity:
A. The Concept of Multi-Targeting in Obesity Management:
Demonstrate how a multi-omics strategy can be essential for the application of precision obesity management by examining genomes, epigenomics, transcriptomics, proteomics, and metabolomics.
Genomics:
Finding genetic variations linked to illness and prognosis is the main goal of genomics, the most developed of the omics technologies [331]. Obesity is often assumed to be caused by diet and sedentary lifestyles; however, genomic studies show that genetics plays a significant influence in the development of obesity. Knowing a person's phenotype may help develop tailored treatments to stop the obesity pandemic.
Fat mass and obesity (FTO) was the first gene linked to obesity to be identified. The function of FTO in food intake and its main consequences on obesity and diabetes mellitus have been demonstrated by evidence [332-334]. The FTO locus is strongly linked to higher BMI and a higher risk of metabolic syndrome, according to a large-scale GWAS analysis conducted among individuals of European ancestry [335]. The melanocortin 4 receptor gene (MC4R), which is linked to weight, fat mass, and obesity, was also identified as a significantly connected locus due to the finding of FTO [334, 336]. The primary cause of monogenic obesity was found to be the MC4R gene, and phenotypes linked to obesity are linked to the interplay of the FTO and MC4R genes on specific pathways.
Gender variations in body form, fat distribution, and vulnerability to obesity development have also been revealed by earlier genome research. Given that genes have a role in energy homeostasis and hence influence energy intake and expenditure through regulatory mechanisms, there is evidence that genetic variables modulate fat distribution [337, 338].
Furthermore, because of the same environmental influences, family history was formerly thought to be a decent proxy for the genetic risk of acquiring obesity. Several twin studies that estimated the genetic heritability of BMI in adults and children to be between 46 and 72 percent have supported this notion [339, 340].
Epigenomics:
The study of chemical modification and heritable alterations is known as epigenomics. Chemical substances and DNA-associated proteins make up the epigenome, which can influence gene activity preserving the DNA sequence [334]. The biological process known as imprinting is mediated by a variety of epigenetic markers, including DNA methylation, histone acetylation, and non-coding RNAs (e.g., miRNAs) [342]. Chronic diseases can arise as a result of imprinting failure, and obesity is frequently associated with imprinting abnormalities.
According to one theory, environmental variables might result in epigenetic change early in life, which might have a lasting impact on metabolism and the risk of chronic diseases later in life. Recent epigenomic research looked at how pregnancy-related malnutrition affected the offspring's DNA methylation [343]. Stress, malnutrition, or overnutrition during pregnancy can "affect DNA methylation and histone post-translational modification as well as gene expression involved in insulin signalling and fatty acid metabolism," according to the scientists' conclusion. Based on the study, the children will be more likely to be obese and have secondary disorders linked to fat. The Dutch Hunger Winter research supports this assertion even more [344].
Additional epigenome-wide association studies (EWASs) have also yielded fresh lines of evidence that link illnesses to epigenetic changes in a broader research population. Seventy CpG sites were linked to BMI, for example, in the REGICOR research, which was based on samples of 641 persons and 2515 participants in the Framingham Offspring consortium [345].
Transcriptomics:
Circulating microRNAs are a significant finding in transcriptomic biomarkers linked to the risk of obesity and its associated comorbidities (cmiRNAs). They are important communicators between cells and tissues and are secreted into the blood and cerebrospinal fluid [341]. 33 cmiRNAs were found to have dysregulated expression in serum or plasma among obese people in recent research; several of the genes found are involved in the phosphoinositide 3 kinase (PI3K-Akt) and fatty acid metabolism pathways [346]. The research emphasizes how miRNAs regulate adipose tissue and how they may be used to diagnose and treat obesity and associated secondary disorders.
Metabolomics:
Metabolomics is a popular analytical method that quantifies alterations in the metabolite profile of a cell, tissue, or organism [347]. It examines several tiny molecule kinds, including organic acids, fatty acids, amino acids, carbohydrates, and lipids, that are involved in cellular metabolism. Metabolomics has already been utilized to identify a number of clinical illnesses, and these new biomarkers have improved our knowledge of how diseases advance and how their metabolic pathways work [348].
Six metabolic pathways are implicated in order to better understand and predict the likelihood of becoming obese. These include lipid/fatty acid metabolism, bile acid metabolism, choline metabolism, amino acid metabolism, creatine metabolism, glucose metabolism, and the citric acid cycle [349, 350].
Proteomics
Large-scale analysis and quantification of proteins found in biological samples made up of cells or tissue is known as proteomics [351]. The characterization of the proteome and a deeper comprehension of disease mechanisms are major areas of research. Approximately 10% of the human genome expresses secreted proteins, for example, making the serum/plasma proteome a valuable tool for tracking the molecular processes underlying pathogenic alterations associated with obesity [352].
The authors found 43 proteins that were differentially expressed, including those that have been connected to metabolic traits in body mass index and insulin sensitivity and have been linked "to lipid and glucose metabolism, lipid transport, protein synthesis, folding inflammation, and the cellular stress response." Omental adipose tissue is a form of visceral adipose tissue (central obesity), which is an excessive buildup of fat in the abdominal area and is frequently linked to metabolic dysfunction [334]. Subcutaneous adipose tissue is defined as "fat found under the skin and largely around the hips, thighs, and buttocks."
In a multi-omics approach, the various approaches are integrated to investigate the impact of the human body's metabolites, microbiomes, proteomes, transcriptomes, epigenomes, and genomes in order to shed light on the fundamental processes behind the development of obesity. Thus, the many omics biomarker types "investigate changes at different molecular levels, examine the interplay between the molecules, and the roles of different factors involved in the metabolic health deterioration" [332].
B. Combining Nutraceuticals for Enhanced Efficacy:
Nutraceuticals and functional foods have garnered a lot of attention from researchers in recent years for managing body weight, obesity, and associated issues since they offer numerous positive impacts with few or no negative ones [355,357]. Adipocyte lifecycle (adipocytokines from aberrant adipocytes), lipid metabolism (lipase inhibition), food intake (gut-brain axis), and energy expenditure (energy homeostasis-thermogenesis) can all be regulated by genetic or epigenetic mechanisms through the use of functional foods or nutraceuticals, as shown in numerous studies [358,359]. The dose (safety), span of time, and bioavailability are yet unknown, though, as most research focuses on preclinical studies (animal and cell line studies), and very few randomized clinical trials (RCTs) are carried out. [356, 360]
Fatty acids with many double bonds are compressed to form polyunsaturated fatty acids (PUFA). Among them, the main PUFAs are eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), arachidonic acid (ALA), and conjugated linolenic acid (CLA). ALA, DHA, and EPA, on the other hand, are classified as omega (ω)-3-fatty acids (ω-3 FA) and are claimed to have a number of biological properties. [361], ALA and CLA are mostly found in flaxseed, while ω-3 FA is abundant in salmon oil. Both fish oil and flaxseed are considered beneficial foods since they include ALA/DHA/EPA and ALA/CLA, respectively. Antioxidant, anti-inflammatory, anti-diabetic, anti-obesity, anti-hyperlipidaemia, immunomodulatory, and anti-arrhythmic and thrombotic effects are only a few of the beneficial properties that ALA, CLA, DHA, and EPA exhibit [362, 363.]
Anti-obesity mechanism: Through the Akt/PI3K and AMPK pathways, regulate adipocyte proliferation and differentiation by activating PPAR-α, lowering leptin expression, inducing thermogenesis in the BAT, and changing adipocytokine expression. [354]. By downregulating the JNK signaling pathway, PUFAs are said to decrease adipogenesis/lipogenesis and enhance fat oxidation (thermogenesis) [364]. By reducing the amount of FFA in the blood and increasing β oxidation, DHA and EPA prevent the formation of TG (triglycerides) [365].
Clinical trial: Consumption of up to 6.8 g of CLA is said to lower fat mass, LDL-c (low-density lipoprotein cholesterol), TG (triglycerides), and TC (total cholesterol) in obese individuals when compared to a placebo (olive oil). CLA may change how certain adipocytokines are expressed, which lowers oxidative stress and the lipid profile. [366] Pre-treatment ω-3 PUFA supplementation may promote weight reduction and a lower BMI in obese women, according to another clinical study. [367] Individuals who consume fish oil or ω-3 PUFA (DHA and EPA) for 4–12 weeks saw notable decreases in body weight, BMI, and waist circumference when compared to the control group. These results were verified by the comprehensive review and meta-analysis by Bender et al., which comprised 15 different studies. According to a recent meta-analysis of RCTs by Zhang and colleagues (2017), supplementation with ω-3 PUFA (fish oil) may considerably reduce triglyceride levels and waist circumference (WC) in overweight and obese adults without affecting body weight or BMI. [368], As a result, fish oil could be suggested as a more potent functional food to combat obesity and its related problems.
Probiotics are live bacteria that live in the host's gut and are essential for the host’s system of health. On the other hand, prebiotics (inulin, fructans, and fructose/galacto-oligosaccharides) are non-digestive substances that support the production of a healthy gut microbiota and the growth of probiotics (bacteria); hence, they are categorized as functional foods [369]: The most often used probiotic bacterial strains are mostly Bifidobacterium and Lactobacillus spp. (plural strain), which are referred to as helpful bacteria that live in the gut (microbiota). Synbiotics are used in combination with probiotics to improve the health of the host. [370]. Anti-inflammatory, antioxidant, immunomodulatory, anti-cancer, anti-hyperlipidemic, and anti-obesity benefits are only a few of the many therapeutic properties that prebiotics and probiotics display [371].
Anti-obesity mechanism: Probiotics have the ability to absorb cholesterol on their own and have bile acid hydrolase activity, which helps the cholesterol attach to deconjugated bile and be riddled. Probiotics can therefore indirectly reduce the risk of obesity and cardiovascular disease by controlling cholesterol levels through either excretion or utilization. [372] Probiotics inhibit lipogenesis via binding to PPAR, altering the activity of lipoprotein lipase (LPL), and fermenting oligosaccharides (galacto/fructo) to produce short-chain fatty acids (SCFA) [370]: By inducing POMC, SCFA also increases the synthesis of GLP-2, PPY, and CCK, which leads to satiety and improves insulin sensitivity. [353]
Clinical trials: When compared to the control group, obese participants who received the probiotic Lactobacillus gasseri (SBT2055) for 12 weeks showed concomitant decreases in body weight, BMI, and waist circumference, as well as an increase in serum adiponectin levels, suggesting that this treatment may considerably reduce abdominal adiposity [373]. By administering Bifidobacterium breve B-3, another well-known probiotic strain, to adult obese subjects for 12 weeks, Minami and his colleagues also conducted another clinical trial that demonstrated a significant decrease in body weight, body fat percentage, and the eradication of several inflammatory indicators [374]. In a 12-week clinical trial, healthy obese subjects who took probiotic yogurt (Bifidobacterium lactis-BB12 and Lactobacillus acidophilus-LA5) orally showed no change in body weight but a significant decrease in body fat, total cholesterol, low-density lipoproteins, and glycemic markers (insulin/HBA1c) when compared to low-fat conventional yogurt [375] In 2018, Borgeraas and colleagues conducted a systematic review and meta-analysis that included 15 RCTs and suggested that probiotic supplementation, compared to the placebo group, resulted in a notable drop in body weight and fat percentage over the course of 3–12 weeks [376]: Overall, pro/prebiotic therapy significantly improves fat metabolism (by changing the gut microbiota-SCFA) and controls the lipid profile in an obese individual.
Psyllium seeds from Plantago ovata are the source of this viscous, water-soluble fiber. It could not result in bloating or other gastrointestinal issues since it ferments more slowly. It also has hypotensive and hypolipidemic effects, lowers the risk of CVD, and is highly recommended for weight loss. [377]
Anti-obesity mechanism: By increasing the hormones CCK and GLP-1/2 and inhibiting ghrelin production, it increases the transitory time of the stomach (delays gastric emptying) and promotes satiety (alters the Gut-Brain Axis). Reduce your glycemic index to reverse insulin resistance and boost your thermogenesis to keep your energy balance. [378, 379] Like probiotics, they can also ferment and create SCFA because they subtly function as prebiotics and bind to PPAR to demonstrate lipolysis by increasing LPL87 activity and enhancing insulin. Read the article online at sensitivity [353].
Clinical trial: According to a clinical study, giving psyllium fibers to people with cardiovascular disease for seven weeks caused their levels of triglycerides and total cholesterol to significantly fall. They also saw a little decrease in body weight and BMI [380] Compared to the placebo group, patients who were overweight or obese and took 2 g of psyllium daily for three months saw a significant decrease in body weight, BMI, and total body fat [381]. In different randomized clinical research, Pal and his colleagues (2016) found that soluble fiber supplements, such as psyllium (15 g/day), significantly reduced body weight, waist circumference, and body fat percentage when compared to the placebo group after 12 months. Overall, psyllium therapy has shown more anti-obesity action than short-term treatment, and because it has fewer side effects than other fibers, it is a superior option for managing obesity. [378]
C. Integration with Diet and Exercise Programs:
In other research, a combined therapy approach was employed. These trials include the usual care approach taken by Tapsell et al., which included three interventions and general guidance from a nurse. Dietitians negotiated changes in certain food choices following assessments, exercise physiologists advised participants to increase physical activity and decrease sedentary behavior following assessments, and psychologists created a workbook for participants and trained health coaches to conduct 15-minute scripted calls [382]. They also incorporated dietary supplements and intervention.
Katzmarzyk et al. employed the usual-care and intensive-lifestyle intervention regimen. While the usual-care regimen included regular, usual care from the primary care team for 24 months, three newsletters per year on specific topics, and a list of health promotion events available in their community, the intensive-lifestyle regimen included an increase in physical activity up to 175 minutes per week, portion-controlled foods (e.g., bananas, apples, soups, and frozen entrees), prepackaged foods, and meal-replacement shakes during the first month [383]. Training in strength (S), endurance (E), and strength & endurance (SE) was employed by Benito et al. Shoulder presses, squats, barbell rows, lateral splits, bench presses; front splits, biceps curls, and French presses for the triceps were all part of the S group. The E group engaged in running, cycling, or elliptical workouts, whereas the SE group included elliptical, treadmill, or cycle ergometry activities with front split exercises, squats, bench presses, and a rowing machine (15 lifts per set or 4500 SE endurance phase). At least 200–3000 minutes of moderate-intensity physical activity (30–60 minutes every day) per week were performed by the C individuals [384]. A low-calorie diet (LCD) and an energy-matched LCD combined with interval exercise training (LCD + INT) were employed by Francois et al. A meal replacement shake with 160 kcal of protein and carbohydrates for breakfast and lunch, a prudent supper choice that didn't surpass 600 kcal (such as lean protein with vegetables or salad), and two 100 kcal snack alternatives made up LCD (1000-1200 kcal/day). A 12-session interval workout program with one day off comprised the LCD + INT regimen. Ten repeats of 50% and 90% heart rate peak (HR peak) were performed in a 60-minute session that alternated three-minute cycling intervals under supervision. [385]
Table. 2: 60-minute session that alternated three-minute cycling intervals under supervision
|
Study |
Dietary and exercises intervention |
Groups |
Outcomes |
|
Tapsell et al. [382] |
A nurse assisted the normal care group in giving general guidance. The intervention counselling session involved a dietitian negotiating changes to certain food choices following assessment, an exercise physiologist advising participants to increase physical activity and decrease sedentary behaviour following assessment, a psychologist creating a workbook for participants, and trained health coaches making prescribed calls. (15 minutes). |
Interdisciplinary guidance vs. usual care (C general advice) vs. intervention + dietary supplement (IW, I+30 g walnuts/day)
|
Weight loss was more substantial and clinically significant with the multidisciplinary regimen than with normal care (1.2 kg, p = 0.045 I; 1.3 kg, p = 0.025); after six months, IW (2.1 kg, p = 0.010)
|
|
Katzmarzyk et al. [383] |
Weekly meetings (six held over the phone and sixteen in person): For the first month, the intensive-lifestyle group will be given prepackaged meals and meal replacement drinks, portion-controlled items (bananas, apples, soups, and frozen dinners), and training on how to buy, prepare, and package food. They will also be encouraged to increase their physical activity to 175 minutes per week. The usual-care group receives normal, routine treatment from their primary care physician for the whole year, as well as three newsletters a year covering specific subjects and a schedule of community health promotion activities |
Comparison between the usual-care groups with the intensive-lifestyle group.
|
There was a mean difference of 4.51% points (95% CI, 5.93 to 3.10) between the groups (P < 0.001), with 51% of patients maintaining at least 5% weight loss at 24 months and the intensive-lifestyle group having considerably larger weight loss of 5%.
|
|
Benito et al. [384] |
A customized, balanced hypocaloric diet with 25% less calories has been recommended for each participant (50%–55% carbs, 30%–35% fat). The S, E, and SE groups all received the same volume and intensity of exercise training three times a week. The exercises in the S group comprised biceps curls, barbell rows, lateral splits, bench presses, front splits, shoulder presses, squats, and French presses for the triceps. While the SE group engaged in a mix of cycle ergometry, treadmill, or elliptical workouts intercalated with squats, rowing machines, bench presses, and front split exercises (15 lifts per set or 4500 SE endurance phase), the E group engaged in running, cycling, or elliptical activities. The C individuals committed to engaging in moderate-intensity physical activity for at least 200–3000 minutes per week (30–60 minutes each day). |
Strength training group (S) vs endurance training group (E), strength þ endurance training group (SE), and the group that adheres to physical activity guidelines (control; C)
|
A balanced, customized, hypocaloric diet was followed; however the SE exercise regimen significantly reduced total fat mass more than other exercise regimens.
|
|
Francois et al. [385] |
LCD (1000 1200 kcal/day): two 100 kcal snack alternatives, a dinner option that didn't surpass 600 kcal (such as lean protein with vegetables or salad), and meal replacement drinks for breakfast and lunch that include 160 kcal of protein and carbohydrates. LCD INT: 12 interval training sessions plus one day off. Ten repeats of 50% and 90% of the heart rate peak (HR peak) were performed in a 60-minute session of supervised exercise that alternated three-minute cycling sessions. The length increased from 30 minutes on the first day to 45 minutes on the second and then to 60 minutes on the third. A mixed meal shake (350 kcal, 13 g protein, 11 g fat, and 50 g carbohydrate) was given after every workout. |
Energy-matched LCD combined with interval exercise training (LCD + INT) vs a low-calorie diet (LCD)
|
Compared to LCD alone, LCD + INT decreased glucose and total-phase glucose-stimulated insulin secretion more. Both treatments lowered blood glucose levels and muscle and body mass.
|
D. Personalized Nutrition Approaches:
Before proposing guiding principles, it is crucial to first define the scope of PN. The lack of a consensus or authoritative definition for "personalized nutrition" in the context of rapid innovation has led to misunderstandings in terms of both technology for information gathering and technology for creating foods, ingredients, and dietary recommendations that use this information. This is seen by the wide variety of PN-handling products on the market. These new potentials are frequently referred to by the term "personalized nutrition," but other terminology, such as "precision nutrition," is also used, which adds to the confusion [386]. Given the challenges in establishing causation and the complexity of physiological networks in the treatment of health and illness, the advantages of PN and other tailored approaches to health have come under examination [387]. This is happening concurrently with a growing market, not all of which may be supported by scientific evidence. There is little data that explicitly shows how effective PN strategies are over the long run when compared to population-based recommendations.
Finding a definition for PN is essential since different parties and goals use different terms related to individualization interchangeably, which contributes to misunderstandings. In particular, [387] mention data that may be utilized to create customized recommendations, goods, or services. While "customized nutrition" has been used to refer to addressing dietary choices and accessibility/delivery alternatives, "precision nutrition" is primarily focused on disease intervention [388]. Definitions were expanded by [389] to encompass physical activity and eating habits. Whatever the nomenclature, they all have the same fundamental components: adjusting dietary recommendations to take into consideration individual differences in phenotype, genetics, lifestyle choices (exercise, food, etc.), goals, and preferences. The purpose of the 2018 panel was to refine the practical working definition of PN that was developed by the 2017 ILSI North America expert group.
The following definitional terminology is suggested by the 2018 panel:
Individual-specific information based on evidence-based research is used in personalized nutrition to encourage dietary behavior changes that might have quantifiable health advantages.
The following describes the elements that make up this definition:
Measurable health benefits: PN's benefits need to be measured with accurate methods and metrics. Weight and body composition (e.g., increased bone mineral density or weight status), modifications to a specific nutritional marker (e.g., enhanced micronutrient status), or measurements of blood glucose control (e.g., improved haemoglobin A1c or fasting glucose) are examples of quantifiable, validated health indicators. According to a new definition, health is the body's capacity to adjust and control itself when faced with emotional, physical, and social difficulties [394]. In other words, the ability to cope with daily or ongoing stressors might be considered a health indicator. The ability to adapt to continuously changing conditions is known as "phenotypic flexibility" [395], and monitoring the biological response may offer a sensitive way to monitor changes in an individual's health status over time [396]. According to the PN definition, "function" also refers to phenotypic modifications that improve quality of life or individual performance (such as mobility, cognition, or other outcomes), independent of the conventional notion of "health."
VII. Future Directions and Research Gaps
A. Need for More Robust and Long-Term Clinical Trials
Recent draft guidance published by the FDA in January 2025 for developing drugs and biological products for weight reduction to establish standards for clinical trials stipulates that clinical trials need to reflect the age, sex, race, and ethnicity of obese populations in clinical practice for the US population [397].
An analysis of major obesity trials was conducted to understand the representativity of recruited populations. Seven trials each recruited over 1,000 participants: Novo Nordisk’s SELECT, SCALE, FLOW, STEP 1, and STEP 2; and Lilly’s SURPASS trial and SURMOUNT-CVOT (Figure 1). These trials measure the effect of GLP-1 receptor agonists (or tirzepatide, a dual GIP-GLP-1 receptor co-agonist) on weight loss in overweight or obese populations or related comorbid populations. The analysis, however, found that the recruited trial populations are not representative of the US obese population [398, 399, and 400]. Of course, the agents in these trials are not being developed for the US population alone, but the US is, and is likely to remain, the single biggest commercial opportunity for AOMs, with recent regulatory draft guidance proposing that trial demographics should reflect the US obese population. Whilst it is possible to compare trial populations for age and sex to demographics outside of the US and UK, it is unfortunately not possible to compare race demographics in other EU countries due to sensitivity in reporting and collecting of these data [401].
The Long-term Effectiveness of the Anti-obesity Medication Phentermine (LEAP) trial, a placebo-controlled, randomized trial, will be conducted at 5 clinical sites across the United States. All participants will be provided with an evidence-based online lifestyle intervention, and participants receiving 24 mg/day of phentermine vs. a placebo for up to 24 months will be compared in an intent-to-treat fashion. The co-primary outcomes of percent weight loss and change in systolic blood pressure at 24 months will be examined. Also, between-group changes in drivers of energy balance, including resting metabolic rate, caloric intake and physical activity, and dietary composition, will be compared. ClinicalTrials.gov. (n.d.). Long-term Effectiveness of the Antiobesity Medication Phentermine (LEAP)
B. Personalized Nutraceutical Interventions (Nutrigenomics, Nutrigenetics)
Recent advances in genomic research provide evidence that focusing these efforts on individual variations in abilities to metabolize nutrients (nutrigenetics) and exploring the role of dietary compounds on gene expression (nutrigenomics and nutri-epigenomics) can lead to more meaningful personalized dietary strategies to promote optimal health. [402]
Precision Nutrition encompasses a wealth of data, including agri-genomics, nutrigenomics, nutri-proteomics, and nutri-metabolomics. It integrates genomic information with phenotypic, cultural behavioural, and lifestyle preferences to provide both general guidance and personalized health recommendations [403]. However, motivating individuals to change their eating habits remains a major challenge. Individual motivation is essential for the success of personalized diets [404]. Factors like psychosocial aspects can influence eating behavior. Nutrigenomic advice is generally better understood, more likely to be adhered to [405], and supports long-term weight management [406].
Advancements in laboratory techniques, such as mass spectrometry, chromatography, electrophoresis, microarrays, and magnetic resonance spectroscopy, have enabled a comprehensive approach to enhance nutritional interventions based on individual nutritional and metabolic considerations. This allows for precise dietary adjustments according to individual needs and the identification of those who would benefit from specific intervention strategies [403]. Omics technologies, like proteomics, lipidomics, and metabolomics, are used for biomarker testing and the analysis of bioactive compounds and food components to develop tailored diets.
Nutritional genomics comprises two key components: nutrigenomics and nutrigenetics [407]. This field, often called 'nutrigenomics,' bridges genome research, biotechnology, and molecular nutrition to enhance our understanding of how nutrition impacts health. It provides insights into how food affects the body's balance, offering information on potential benefits and adverse effects even before disease onset [403]. Nutrigenomics utilizes cutting-edge omics technology to define 'dietary signatures' that capture nutrient effects on the human genome, gene expression, and health. These signatures encompass observable changes at genetic (genomics and epigenomics), gene transcript (transcriptomics), protein (proteomics), and metabolic (metabolomics) levels [407]. Conversely, nutrigenetics identifies genetic factors contributing to individual responses to diet and their role in diet-related disease development. It focuses on minor genetic sequence alterations influencing specific metabolic pathways. Studies have explored common gene polymorphisms like single nucleotide polymorphisms (SNPs) in conditions such as obesity, metabolic syndrome, and cardiovascular risk [407].
Obesity is a complex condition influenced by genetic, environmental, and social factors. Recent advances in human genetics have identified over 600 gene markers and chromosomal regions linked to obesity. These genes are involved in vital processes, especially appetite regulation, impacting obesity development. While there are rare genetic syndromes related to obesity, they are exceptions and not representative of most obese individuals. Modern genetic technology enables parallel genotyping analysis of numerous single nucleotide polymorphisms (SNPs) from a single sample, although there are about 10 million SNPs in the human population. By examining groups of related SNPs, called 'haplotypes,' researchers can gain valuable insights into genetic variation patterns within a region. The International HapMap Project aims to define these haplotype blocks and identify reliable tag SNPs for genetic research [408].
C. Development of Novel Nutraceutical Formulations and Delivery Systems
Building on these recent findings, this review explores cutting-edge advancements in lipid-based nano-carrier systems for delivering anti-obesity natural compounds. We highlight how these innovative platforms address limitations of conventional therapies, opening avenues for targeted and personalized obesity treatment. Key classes of bioactive phytochemicals such as polyphenols, alkaloids, terpenoids, and saponins are examined for their therapeutic potential, alongside challenges like poor bioavailability and stability. Advanced delivery systems, including liposomes, solid lipid nanoparticles (SLNs), and nanostructured lipid carriers (NLCs), are discussed for their roles in enhancing solubility, targeted delivery, and sustained release. We also look into recent strides in precision therapeutics, emphasizing nanotechnology’s promise in tissue-specific targeting and stimuli-responsive drug release.
Lipid-based nano-delivery systems
Lipid-based nanocarriers have become a revolutionary giant method of obesity treatment that promises to provide alternative remedies to conventional treatment challenges. Besides the ability to encapsulate drug molecules and natural barrier penetration features, the nanocarriers possess high biological tolerance. At the nanoscale level, engineers have created lipid-based nanocarriers that enhance the efficiency of active agent delivery by addressing efficiency issues related to obesity treatment, such as low bioavailability and unspecific targeting. These systems are primarily composed of lipids, as this group of molecules is naturally attracted to the membranes of cells which allows an improved absorption of drugs, a controlled release of medications, and increased therapeutic efficacy.
Table. 3: Different Lipid-based nano-delivery systems
|
No. |
Lipid-based Nanocarrier |
Structural Characteristics |
Advantages Over Others |
Advantages for Natural Compounds |
Disadvantages/ Limitations |
References |
|
1 |
Liposomes |
Spherical vesicles with phospholipid bilayer |
High biocompatibility, suitable for hydrophilic/ hydrophobic drugs, targeted delivery |
Protects compounds (e.g., curcumin, catechins) from degradation, improves bioavailability |
Prone to instability/leakage, costly, limited shelf life |
[409, 410] |
|
2 |
Solid Lipid Nanoparticles (SLNs) |
Solid lipid core with surfactant coating |
Better stability than liposomes, controlled drug release, high bioavailability |
Protects lipophilic compounds from degradation, enhances solubility |
Low drug loading, risk of drug expulsion during storage |
[411, 412] |
|
3 |
Nanostructured Lipid Carriers (NLCs) |
Mix of solid & liquid lipids, imperfect crystalline matrix |
Higher drug loading than SLNs, better stability, less premature release |
Suitable for poorly soluble phytochemicals, maintains active stability |
Complex formulation, possible cytotoxicity at high dose |
[413, 414] |
|
4 |
Lipid Micelles |
Self-assembled amphiphilic lipid spheres |
Improves solubility, increases absorption of poorly soluble drugs |
Raises bioavailability of polyphenols/flavonoids |
Limited payload, risk of instability in biological fluids |
[415, 416] |
|
5 |
Exosomes/ Biomimetic Nanocarriers |
Natural/ synthetic lipid bilayer vesicles |
High biocompatibility, efficient cell uptake, minimal immunogenicity |
Delivers anti-obesity drugs to adipose tissue, enables targeted delivery |
Complex production, regulatory hurdles for clinical use |
[417, 418] |
|
6 |
Self-Emulsifying Drug Delivery Systems (SEDDS) |
Oil-based, forms emulsions in GI tract |
Improves oral bioavailability, enhances lipid drug stability |
Facilitates absorption of lipid-soluble phytochemicals (e.g., resveratrol) |
Requires surfactants, risk of GI irritation |
[419, 420] |
D. Nutrivigilance, Phytovigilance, and its importance
Because of our limited information about nutraceuticals and herbal products, we tend to misuse them. Irrational use of these products prevails in our nation. Nutraceuticals, herbal products, and health supplements are used indiscriminately without a clear channel to report the related adverse effects. It creates a big problem of detecting such adverse effects and taking the necessary corrective measures for the same. [421-423]
FSSAI should take a proactive approach towards nutrivigilance. Tighter regulation must be implemented for nutraceutical and health supplement approval. A plan for monitoring the long-term impact of the products should be there. The absence of strong clinical trials with such products is one of the key limitations in an existing regulatory environment. Healthcare providers can have a significant contribution towards nutrivigilance through actively detecting the consumption of such products and any untoward effects. There should be a provision for education at the primary care level regarding the appropriate use of nutraceuticals and the potential limitations of the products. Special groups must make use of such products cautiously; for instance, sportspersons and athletes must be cautious about the composition of health supplements or sports beverages they consume so that they do not fall into inadvertent doping. [424, 425] It should be started by FSSAI with the help of digital platforms to teach the common population about the potential effects of unthinking consumption of nutraceuticals. It is the time to define the indications of complex nutraceutical products as the same is defined for pharmaceutical products. It is also important to stop unsubstantiated and spurious claims and advertisements at the mass level. Need to regulate the promotional matter of nutraceuticals strictly.
E. Regulatory Harmonization
Anti-obesity nutraceuticals fall under differing regulatory systems across the globe, usually leading to market uncertainty and possible danger to consumers. Harmonization initiatives seek to guarantee product safety, effectiveness, and openness:
The market for nutraceuticals, including functional foods, dietary supplements, and drugs, has experienced unprecedented growth worldwide as consumers grow more curious about health and wellness products. International harmonization is, however, hampered by the vast disparities in the regulation regimes that cover such products. As dietary supplements, nutraceuticals are regulated in the US mainly under the Dietary Supplement Health and Education Act (DSHEA) of 1994. Pre-market and post-market regulations, including advertising and labeling statements, are overseen by the Federal Trade Commission (FTC) and the U.S. Food and Drug Administration (FDA). Conversely, the Food Safety and Standards Authority of India (FSSAI) regulates nutraceuticals in India under the Food Safety and Standards Act (FSSA), 2006; guidelines for nutraceutical foods and health supplements were made available in 2022. This work aims to enlighten on the challenges faced by industry stakeholders and the potential for global regulatory harmonization through a review of the regulating frameworks of both countries, paving the way for a more harmonized global nutraceutical market. [426]
Governments in the Asia-Pacific region, the US, and India are updating their rules on supplementation for efficacy claims, acceptable ingredients, safety cautions (e.g., for certain herbal extracts), and labelling of large dosage forms.
The Food Safety and Standards Authority of India (FSSAI) currently regulate the standards of health supplements and nutraceuticals. FSSAI established regulatory standards for the approval of nutraceuticals in India. The standards include eight categories of functional food. To prevent mix-ups between categories of nutraceuticals, FSSAI released a guidance note on August 28, 2020. It explains that health supplements are meant to supplement the ordinary diet of an individual with one or more nutrients that are known to be beneficial. Special dietary use foods (FSDU) are processed or formulated specially to meet dietary needs for particular diseases. Special medical purpose foods (FSMP) are meant for exclusive or partial feeding to individuals suffering from digestive diseases. [9] Nutraceuticals are those naturally occurring substances that are extracted, isolated, and purified from food or non-food items, which, upon consumption, offer physiological advantages and help maintain the good health of the recipients. Health food supplements and nutraceuticals are aimed at the healthy population aged over five years and over two years, respectively. Yet, FSDU and FSMP are for individuals with certain needs, with the age being over two years. [427]
The Food Safety and Standard (FSS) rules were released by FSSAI in 2011. Such regulations involved food product licensing and registration, food business requirements, methods for packaging and labeling, food product standards, and food product additives. The FSS regulations were implemented in August 2011. FSS regulations of 2015 issued guidelines for nutraceuticals and food/health supplements, foods for special dietary use, foods with medicinal use, and functional and novel foods. According to these regulations, the nutraceuticals shall include any of the ingredients mentioned in the "Food Act Schedule" as provided in Table 1. [430] According to these regulations, the following information must be provided in any claimed novel food: chemical composition of the food that has been engineered, surface modification/surface chemistry, primary particle size, solubility, digestibility, quantity of nanomaterial, if any, present in the food product, and specific claim, if any. [430]
In 1990, the Nutrition Labeling and Education Act (NLEA) established what food is labeled, including nutrition labels, according to definitions laid down by the FDA that have been modified with the "Food Safety and Standards (Packaging and Labeling) Regulation, 2011." These regulations provided more legal security and a more certain climate. It encourages innovation and avoids unjust competition by manufacturers relying on false or misleading statements. If a positive statement cannot be made, the regulation does not compel anyone to issue a negative statement regarding the product. [430, 431] In 2018, the Food Safety and Standards (Advertising and Claims) Regulations were enacted. It was primarily to regulate the advertisements and claims by food business operators regarding their foodstuffs [432]. All significant regulations and amendments are available on the FSSAI website (https://www.fssai.gov.in/cms/food-safety-and-standards-regulations.php).
Regulations for manufacturing, registration, advertising, and claims are evolving. Primary requirements now are clinical substantiation, transparent labeling, honest advertising, and obligatory safety warnings on listed ingredients.
The Food Safety and Standards Act (FSSA) of 2006 comprises 21 chapters, and in that, Article Fourth of the act governs nutraceuticals, dietary supplements, and other functional foods and their production, manufacture, marketing, sale, distribution, and import. For a very long time, the Food and Drug Administration (FDA) regulated dietary supplements as food to ensure that they were safeguarded and that their labeling was truthful and non-misleading. In 2006, FSSA was enacted by the Indian government to consolidate and simplify the various controls of nutraceuticals, fortified food, and dietary supplements. [428]
The FSSAI act was enacted by the parliament in 2006, but FSSAI was launched in 2008. On September 5, 2008, the Indian government recommended the establishment of the FSSAI as a senior administrative specialist, consisting of a chairperson and 22 members. [429]
Consumer Education
Enhanced consumer awareness is a turning point for the safe and informed consumption of antiobesity nutraceuticals:
Consumers are confronted with deceptive marketing and inflated claims, which may result in abuse or unreasonable expectations. Lack of information regarding product guidelines and risk from ingredients continues, particularly with natural substances and high-dosage products.
Unambiguous labeling including dosage, safety notices (e.g., liver damage from specific herbal ingredients), and mandated disclaimers.
Educational campaigns for the consumer to assess efficacy and scientific evidence, translate health and nutritional claims, and comprehend the position of supplements as part of a healthy life.
Policies against misleading promotion provide assurance that claims are factual, meaningful, and backed by science. Particular emphasis on special groups (children, seniors) in order to avoid excessive intake or incorrect use.
Changing role of the medical affairs/ pharmaceutical physician for nutraceuticals and consumer healthcare products:
The medical affairs function is a bridging interface between commercial functions like sales and marketing with research and development and with external stakeholders like healthcare professionals and the public. It, therefore, has a key function to pass on valuable and scientifically sound information on nutraceutical products to commercial functions and healthcare professionals, that is, to internal and external stakeholders. Medical affairs must engage with key opinion leaders or key medical experts (KME) to learn about the unmet needs and to communicate key scientific messages regarding the products. Since regulatory standards are becoming more stringent for promotional and use purposes of nutraceutical products, the function of medical affairs also becomes vital. There is growing attention to nutraceutical promotional materials and claims, for which these need to be robustly supported by scientific data. Medical affairs can facilitate the claim substantiation with evidence generation through proof of concept and clinical trials for nutritional products as evidence-based practice. Real-world evidence of product use in a large population can be created. The economic value of the products with health economics and outcomes research (HEOR) data can be justified. [433-435] Developing an understanding of unmet needs and shaping the future of new and innovative products is also an integral function of medical affairs. The small innovation cycle with such nutraceutical products has a need to keep exploring new formulations, innovative ingredients, and/or delivery mechanisms supported by strong scientific rationale. Sharing the evidence-based information on nutraceuticals in an ethical and scientific way is the foundation of medical affairs. There is a growing expectation for the medical affairs team to encourage the responsible use of nutraceuticals and nutrivigilance. This contributes to the continually evolving role of pharmaceutical physicians [433-435].
CONCLUSION
Regulatory-wise, nutraceuticals have various and occasionally vague standards across nations, and it seems opportune to develop more harmonized frameworks. In America, labeling and safety are mandated by the Dietary Supplement Health and Education Act (DSHEA), but in India, the Food Safety and Standards Authority of India (FSSAI) has been constituted and charged with the responsibility of regulating nutraceuticals under the Food Safety and Standards Act. China and the US are both headed in the direction of more rigorous regulation, with more clinical evidence, clearer labeling, and stricter control of health claims. Another factor in transparency and consumer trust is the third-party certifications, including GMP, NSF, and USP.
Nevertheless, consumer awareness is one of the greatest issues. Quick-fix promises attract many people and thus may be abused, particularly when products are advertised with exaggerated or false claims. Education is the most critical and is to be imparted later on, just as labeling, the truth, and the need to take nutraceuticals and healthy lifestyle habits. Children and older adults are the most vulnerable, and they must not be given incorrect doses or formulations that could harm them. In this case, medical practitioners, such as pharmaceutical physicians, play an increasingly significant role in safe use, evidence-based product development, and safety surveillance in post-marketing, or nutrivigilance. Engagement helps to secure the gap between innovation and responsible consumer use.
Consistently, the future of obesity treatment using nutraceuticals is shifting towards increased accuracy due to personalized nutrition, new delivery methods, more stringent regulations, and knowledgeable consumer interaction. These advances, when integrated with lifestyle and behavioral interventions, can provide safer, more efficient, and more sustainable solutions to address obesity in the general population.
REFERENCES





Dhruvi Patel, Tisha Thakkar, Meshwa Trivedi, Disha Patel, Harshangi Parmar, Dhaiyashree Kher, Nutraceuticals for Obesity: A Comprehensive Review of Mechanisms, Efficacy, and Future Prospects, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 1584-1664. https://doi.org/10.5281/zenodo.17580292
 10.5281/zenodo.17580292
10.5281/zenodo.17580292