
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacology, Progressive Education Society’s Modern College of Pharmacy, Nigdi, Pune-411044
The leading causes of death and illness worldwide are linked to heart and blood vessel diseases. A major contributing factor to atherosclerosis and related conditions is hyperlipidemia, characterized by abnormal blood lipid levels—especially elevated LDL cholesterol, triglycerides, and overall cholesterol. Both environmental and genetic elements shape this condition. Current management combines pharmacology, mainly statins, with lifestyle changes. Statins remain the most effective option for lowering LDL-C and reducing cardiovascular events, but some patients don’t reach target LDL-C levels even at the highest tolerated statin dose, necessitating additional therapies. Proprotein convertase subtilisin/Kexin type 9 (PCSK9) plays a crucial role in lipoprotein metabolism. Rare gain-of-function PCSK9 mutations raise LDL-C and increase the risk of premature coronary disease, while loss-of-function variants lower LDL-C and reduce coronary risk. Notably, statin therapy can raise PCSK9 levels via negative feedback, which promotes degradation of LDL receptors and can diminish the LDL-C–lowering impact of statins. This makes PCSK9 inhibition a rational strategy, and multiple approaches are being explored to target it [1,2].
Even with treatments that effectively lower LDL cholesterol (LDL-C), heart disease continues to top the list of causes for death and serious illness around the world. Proprotein convertase kexin/subtilisin type 9 (PCSK9) plays a key role in this by boosting LDL-C levels in the blood. It does so by interfering with the LDL receptor (LDLR)'s recycling process in cells, sending the receptor to lysosomes for breakdown instead. This blocks the liver's ability to clear LDL-C from circulation, resulting in high cholesterol buildup. PCSK9 blockers help cut cardiovascular risks by interrupting this harmful process. Developers have created options like monoclonal antibodies and antisense oligonucleotides, which either slash PCSK9 levels or stop it from latching onto the LDLR. Still, the holy grail might be small-molecule drugs that people can swallow easily and that potently block PCSK9 activity. Nature offers a treasure trove here—many blockbuster drugs trace their roots back to plant- or microbe-derived compounds, underscoring why screening natural substances for PCSK9-fighting potential remains a smart strategy [5].This research dives into PCSK9's inner workings, reviews the types and real-world applications of existing PCSK9 inhibitors, and spotlights the latest breakthroughs in the field. The goal? To offer clear guidance for clinicians prescribing these drugs and inspire smarter paths for developing the next generation of therapies [3,4].
Pathophysiology of Hyperlipidemia
Hyperlipidemia arises from a tangled mix of genetic and lifestyle factors that throw off the body's lipid balance, often ramping up production or slowing down removal—or both. Among the factors people can actually change are diets heavy in trans and saturated fats, cigarette smoking, sedentary habits, and excess weight. On top of that, various underlying conditions like type 2 diabetes, chronic kidney disease, hypothyroidism, high blood pressure, bile duct blockages, and certain medications (such as glucocorticoids or cyclosporine) can trigger it too. Problems clearing lipoproteins from the blood also fuel hyperlipidemia. Mutations in genes like LDLR, APOB, or PCSK9 impair LDL receptor function, slashing LDL uptake and driving up blood LDL-C levels. Weaker lipoprotein lipase (LPL) activity—or issues with its helpers like APOC2, APOA5, GPIHBP1, or LMF1—causes triglyceride-packed particles to pile up, sparking severe hypertriglyceridemia. HDL often falters too, especially amid inflammation or metabolic syndrome, hampering reverse cholesterol transport through lower APOA1 production or faster HDL breakdown. Insulin resistance worsens this picture, fueling atherogenic dyslipidemia by boosting fat breakdown, flooding the system with free fatty acids, curbing LPL, ramping up VLDL release, and shifting LDL toward small, dense particles while dropping HDL-C. Conditions like hypothyroidism, diabetes, kidney or liver disease, plus meds such as glucocorticoids, diuretics, or cyclosporine, pile on by tweaking lipid pathways. Genetic culprits—like familial hypercholesterolemia (LDLR, APOB, PCSK9 hits), familial combined hyperlipidemia (polygenic tweaks in USF1, APOA1, APOB, APOE), or familial hypertriglyceridemia (LPL pathway flaws)—jack up lipids early in life and skyrocket heart risks. A cholesterol-heavy diet reshapes liver cholesterol handling, LDLR control, and PCSK9 output. Gut-absorbed cholesterol hitches rides on chylomicrons to the liver, spiking intracellular stores. This dials down SREBP2, the master switch for LDLR and PCSK9 genes, curbing their production and slashing new LDLR synthesis alongside cholesterol-making enzymes. Lower PCSK9 follows suit, easing its attack on LDLRs and keeping more receptors on liver cells for LDL clearance. Even with fewer new receptors, this balance sustains LDL removal—but surplus liver cholesterol also cranks out more VLDL, bloating blood lipoprotein levels[1,5,6
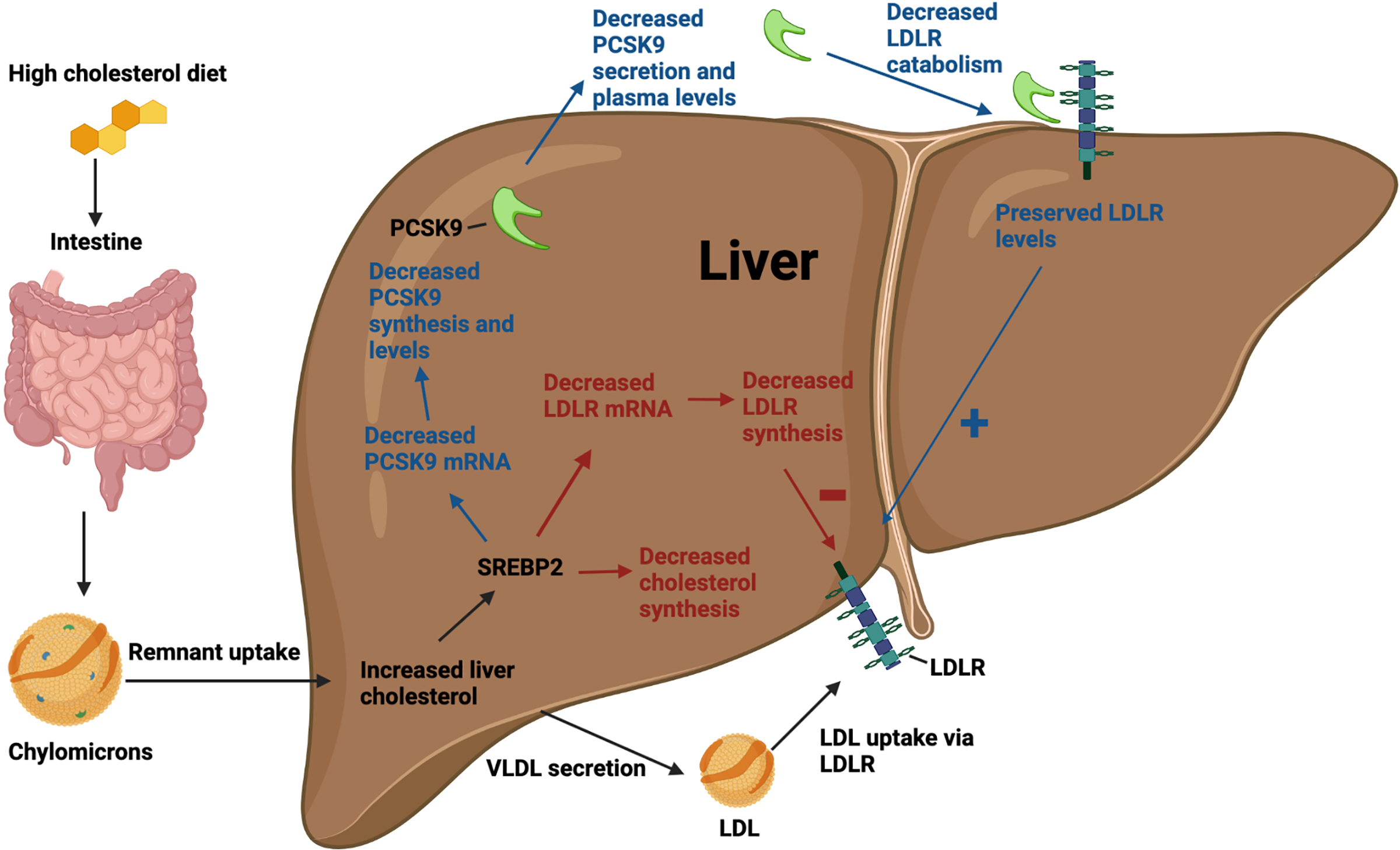
Figure 1. Pathophysiology of Hyperlipidemia
PCSK 9 Inhibitors
PCSK9 inhibitors represent a fresh wave of cholesterol-lowering drugs, tailored for people who can't hit LDL-C goals even on maxed-out statins, those battling familial hypercholesterolemia (FH), or anyone facing sky-high heart risks. As a serine protease churned out mainly by liver cells, PCSK9 latches onto LDL receptors (LDLR) and drags them into lysosomes for destruction. This slashes the liver's LDL-C scavenging power from the bloodstream. In everyday physiology, liver-made PCSK9 grabs LDLRs on hepatocyte surfaces, sending them to the shredder and leaving fewer receptors to mop up circulating LDL-C. Drugs like alirocumab and evolocumab—fully human monoclonal antibodies—swoop in to snag free-floating PCSK9, blocking its grip on LDLRs. This spares the receptors, letting them loop back to the cell surface in higher numbers for turbocharged LDL-C clearance. The payoff? Dramatic drops in blood LDL-C, far beyond what statins deliver solo [1].
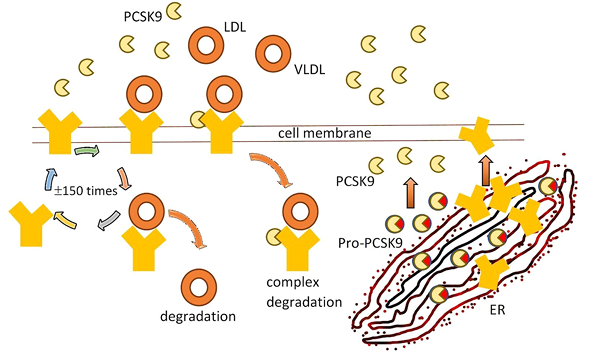
Figure 2. Circulation of receptors for LDL in the hepatocyte.
Structure and Interaction of PCSK9
PCSK9, a 692-amino-acid serine protease, features a prodomain, catalytic domain, and histidine-packed C-terminal region. It kickstarts with autocatalytic cleavage in the zymogen form before heading out of the cell, but the prodomain stays glued to the catalytic site, keeping the enzyme dormant—showing that PCSK9 doesn't need active protease chops to mess with LDL-C levels. Once secreted, PCSK9 zeroes in on the EGF-A patch of the LDL receptor (LDLR) via a broad hydrophobic patch, with binding supercharged in acidic, calcium-rich settings. At lysosomal pH, this grip tightens massively, hauling both PCSK9 and LDLR into destruction and starving the liver of LDL-clearing receptors. About 30–40% of circulating PCSK9 hitches to LDL particles, naturally dialing down its potency. Gain-of-function mutations linked to familial hypercholesterolemia weaken this LDL tethering, unleashing more free PCSK9 to spike LDL-C. A wiggly N-terminal stretch in the prodomain, forming an amphipathic α-helix, proves key for snagging LDL [3].
Mode of Action of PCSK9 Inhibitors
PCSK9 inhibitors hit different points in the protein's lifecycle, sorting into three main buckets. First up, blocking LDLR binding: monoclonal antibodies like alirocumab and evolocumab snag free PCSK9 in the blood, stopping it from grabbing LDL receptors. This keeps receptors safe from breakdown, letting them shuttle back to liver cell surfaces for better LDL-C cleanup. Second, they curb PCSK9 production itself—think gene-silencing tools like inclisiran, an siRNA that dials down translation right at the source. Third, some target the autocatalytic step, halting PCSK9's maturation and release from liver cells.
Normally, PCSK9 clamps onto LDLR's outer domain, and the duo gets pulled inside cells for lysosomal shredding, thinning out LDL-clearing receptors and letting LDL-C build up. Block PCSK9, and LDLR sticks to its healthy routine: it snags ApoB100 on LDL particles, dives into endosomes, releases LDL under acidic conditions (which gets trashed), and bounces back to the surface for round after round. This recycling boost supercharges blood LDL-C removal [3].
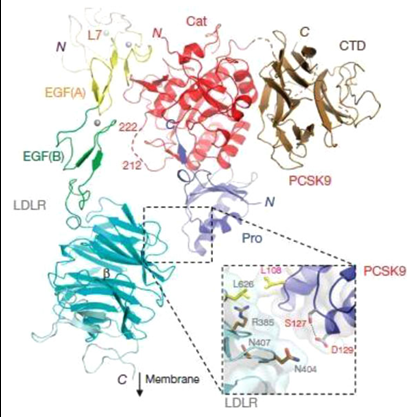
Figure 3. PCSK 9 structure
What PCSK9 Inhibitors Achieve
PCSK9 inhibitors deliver stunning LDL-C drops—typically 50–70%—far outpacing what statins or other lipid drugs can do solo. Trial after trial shows that layering them onto standard care not only sharpens lipid profiles but also slashes serious heart events like heart attacks and strokes, particularly in high-risk groups. They're game-changers for folks with familial hypercholesterolemia, where genetic glitches make conventional meds fall short on LDL control. The same goes for patients with established atherosclerotic cardiovascular disease (ASCVD) needing aggressive cholesterol cuts, or those who can't tolerate statins or hit targets even at max doses. The FDA has greenlit two main types: human monoclonal antibodies and small interfering (si)RNAs [1,3,7,8,16].
Types of PCSK 9 Inhibitors
1.Monoclonal Antibodies (mAbs):
Monoclonal antibodies (mAbs) stand out as the frontrunners in PCSK9-blocking therapies, ranging from murine and chimeric versions to humanized or fully human ones based on their makeup. They pack a punch solo or stacked with statins, driving even steeper LDL-C drops. Evolocumab kicked things off as the first PCSK9 mAb greenlit by the EMA in 2015, with FDA approval hot on its heels. This fully human powerhouse stops PCSK9 from latching onto LDL receptors. Trials like OSLER-1/2 and FOURIER showed steady ~59% LDL-C cuts, with side effects mostly mild skin reactions at injection sites. Alirocumab followed suit, landing FDA approval right after evolocumab's EMA nod. ODYSSEY LONG-TERM and ODYSSEY OUTCOMES trials revealed biweekly shots trimming LDL-C by 55–63%, holding gains long-term with safety on par with evolocumab—though injection-site issues edged a bit higher. Meta-analyses hint evolocumab might outpace alirocumab by 14–20% in LDL-lowering power. These mAbs shine without statins too, as DESCARTES proved: evolocumab alone slashed LDL-C by ~56%, a boon for statin-averse patients. Bococizumab, a humanized contender, started strong but fizzled when anti-drug antibodies cropped up in nearly half of users, tanking efficacy and halting development. Fresher faces like LY3015014 and 1B20 look promising—LY3015014 delivered up to 50% LDL-C drops with minimal immune pushback, while 1B20 hit 50–70% reductions in animal studies, amping up further with statins
a.Alirocumab
Alirocumab, a fully human monoclonal antibody in the PCSK9 inhibitor family, comes from Sanofi and Regeneron and earned FDA approval in 2015. Delivered via subcutaneous injections, it zeroes in on PCSK9 to slash LDL-C levels—making it a powerhouse for folks who can't get enough control from statins alone or skip them due to side effects. The ODYSSEY trial series spotlighted its chops, delivering 50–60% LDL-C drops alongside meaningful cuts in cardiovascular risks [9].
Mechanism of Action
PCSK9, a protein floating in the bloodstream and mostly made by liver cells, naturally hooks onto LDL receptors (LDLR) on hepatocyte surfaces—often with an LDL-C particle in tow. This duo gets pulled inside the cell via endocytosis, but instead of the receptor looping back out for reuse, PCSK9 reroutes it to lysosomes for destruction. With fewer LDLRs on duty, the liver struggles to scoop up circulating LDL-C, letting blood levels climb.Alirocumab, a fully human monoclonal antibody, swoops in to grab free PCSK9, blocking its attack on LDLRs. Freed from PCSK9's grip, those internalized receptors recycle smoothly back to the surface, boosting their numbers and ramping up LDL-C clearance from the blood. The result? Sharp, sustained drops in circulating cholesterol [10,11].
Clinical Uses
Alirocumab steps in for patients needing big LDL-C cuts. It tackles dyslipidemia when statins fall short, helping hit target levels more reliably. In folks with atherosclerotic cardiovascular disease (ASCVD)—think past heart attacks, strokes, or peripheral artery issues—the ODYSSEY OUTCOMES trial showed it cuts major heart events. Plus, it acts as a go-to first-line option for those who can't stomach statins due to side effects [12, 13].
b.Evolocumab
Introduction
Evolocumab, a fully human IgG2 monoclonal antibody from Amgen, falls into the PCSK9 inhibitor camp. It zeroes in on proprotein convertase subtilisin/kexin type 9 (PCSK9), the protein that controls LDL receptor recycling. Given as a subcutaneous injection—usually 140 mg every two weeks or 420 mg monthly, tailored to the patient—it tackles LDL-C reduction in diverse hyperlipidemia cases and cuts cardiovascular risks in high-stakes scenarios [14].
Mechanism of Action
Evolocumab works its cholesterol-lowering magic by zeroing in on PCSK9, the circulating protein churned out mostly by the liver. Normally, PCSK9 latches onto LDL receptors (LDLR) on liver cell surfaces, steering them toward breakdown instead of letting them recycle back out. This leaves fewer receptors to grab LDL-C from the blood, letting levels stay high.
With high-affinity precision, evolocumab snags free PCSK9, blocking its assault on LDLRs. Receptors dodge destruction, loop back to the surface in greater numbers, and ramp up LDL-C clearance from circulation—driving sharp drops in blood cholesterol [14].
Clinical uses
These PCSK9 inhibitors shine as add-ons to diet and standard lipid-lowering treatments when patients miss LDL-C targets on conventional regimens alone. They step up to further slash LDL-C in statin shortfalls, pair powerfully with other therapies for severe genetic hypercholesterolemia like familial forms, and cut risks of major cardiovascular hits—heart attacks, strokes—in folks already maxed on statins but needing more firepower. They also work solo or alongside non-statin options for those who can't tolerate or respond fully to statins [15].
Effect of Alirocumab and Evolocumab on Other Lipid Parameters
Beyond their powerhouse LDL-C drops, alirocumab and evolocumab also tweak other lipids in heart-friendly ways. They typically trim non-HDL cholesterol and apolipoprotein B (ApoB) by 80–85% as much as LDL-C—for instance, a 60% LDL-C cut pairs with 48–51% ApoB reduction—signaling a big purge of artery-clogging particles.Triglycerides dip 8–15% on average, with bigger wins in folks starting high. HDL-C edges up 6–10%, and lipoprotein(a)—that stubborn risk factor—falls 20–30%, scaling with dose. While these shifts aren't dramatic, they all point toward lower cardiovascular odds. The real star? That hefty ApoB and non-HDL slash, which likely packs serious punch against heart disease [19].
2. siRNAs
Small interfering RNAs (siRNAs) are short, double-stranded RNA snippets—usually 20–25 nucleotides—that dial down gene activity via RNA interference (RNAi). Each packs a guide strand and a passenger strand. Once inside cells, they team up with the RNA-induced silencing complex (RISC), which tosses the passenger and deploys the guide to hunt down matching messenger RNA (mRNA). The guide locks on, triggering RISC to unleash RNase that chops up the mRNA, blocking protein production. This pinpoint, sequence-specific silencing turns siRNAs into therapeutic heavyweights, zapping disease-linked genes with lasting impact, sharp precision, and low collateral damage. Inclisiran, which homes in on PCSK9 mRNA, stands out as a prime example powering cholesterol-lowering treatments. Inclisiran, a cutting-edge siRNA-based cholesterol buster, shuts down PCSK9 production by siccing the RNA-induced silencing complex (RISC) on its mRNA, slicing it up with RNase for prolonged knockdown. This double-stranded siRNA sports a guide strand tailored to PCSK9 mRNA, paired with N-acetylgalactosamine (GalNAc) tags that lock it onto liver cells for targeted punch. Its staying power means just two shots in year one (day 1 and 90), then every six months— a huge win for sticking with therapy over frequent monoclonal antibody jabs. Trials like ORION-1, -10, and -11 delivered steady 48–60% LDL-C drops lasting 6–12 months per dose, with meta-analyses hinting at fewer major ASCVD events. Side effects mirror placebo mostly, save for mild injection-site tweaks; occasional extras include UTIs, diarrhea, shortness of breath, or rare antibodies. It's greenlit for adults with primary hyperlipidemia, heterozygous familial hypercholesterolemia, or ASCVD needing extra LDL-C firepower beyond max statins—but flops in homozygous forms (per ORION-5). Watch for ORION-4 and VICTORION-2P results on long-haul heart benefits. All told, inclisiran offers potent, hassle-free LDL control, though its price tag still stings [3,15].
3. Vaccines
Developing a vaccine against PCSK9 is an attractive strategy because it could improve treatment adherence and provide long-lasting LDL-cholesterol reduction. However, producing antibodies against a self-protein like PCSK9 is challenging due to natural B-cell tolerance, so specialized vaccine approaches are required. One method uses virus-like particles (VLPs) that display multiple copies of PCSK9 antigens on their surface, enhancing immune recognition and generating a stronger antibody response. Another approach uses AFFITOPE® technology, which designs short peptides that mimic the N-terminus of PCSK9; these peptides are perceived as foreign by the immune system, stimulate antibody formation, and block PCSK9 from binding to LDL receptors. Animal studies show LDL-C reductions ranging from 10–50%, with effects lasting up to a year, and human clinical trials are currently underway [24].
Role of PCSK9 in Regulating Plasma LDL
Plasma LDL cholesterol hinges mostly on how many LDL receptors (LDL-R) dot the surface of liver cells. These receptors snag floating LDL particles, pull them inside, dump the LDL in endosomes, and usually recycle back out to keep clearing blood cholesterol. PCSK9 throws a wrench in this by shrinking receptor numbers. Made in liver cells, PCSK9 gets processed through the endoplasmic reticulum and spills into circulation. There, it clamps onto surface LDL-Rs, hitching a ride inside with them—but instead of recycling, it shunts receptors to lysosomes for destruction. Fewer receptors mean weaker LDL cleanup and rising blood levels. Twist: statins, which crank up LDL-R production, also boost PCSK9 as a pushback, blunting some of their cholesterol-lowering power. Evidence seals it—gain-of-function PCSK9 tweaks mimic familial hypercholesterolemia with sky-high LDL, while loss-of-function versions flood the surface with receptors and tank LDL. This sparked PCSK9 blockers: siRNAs, antisense oligos, and monoclonal antibodies that slash LDL dramatically while ramping up liver receptor levels. They supercharge statins too, unlocking even more clearance [20].
Safety of PCSK 9 Inhibitors
Phase 2 and 3 trials paint a glowing safety picture for alirocumab and evolocumab, even when LDL-C plunges below 15 mg/dL. Injection-site reactions top the list of side effects, but worries around steroid hormones, fat-soluble vitamins, brain fog, infections, or cancers haven't panned out as real threats. Neurocognitive hiccups like confusion, memory slips, or attention lapses popped up in reports, yet heavy-hitters like FOURIER and its EBBINGHAUS brain substudy found no meaningful differences versus controls across all ages. Genetic folks with lifelong PCSK9 loss-of-function mutations back this up—no cognitive woes there either. Long-haul checks kept fat-soluble vitamins (A, D, E, K), cortisol/ACTH balance, and sex hormones steady; vitamin E dips vanished after tweaking for LDL-C changes. Open-label extensions stretching 52–78 weeks keep watch, with no red flags yet. OSLER and ODYSSEY trials matched serious events, muscle issues, and liver enzymes between groups, though alirocumab nudged myalgia rates slightly higher. Those scrutinized neuro events? No link to ultra-low LDL-C. Clues from statin data and rare disorders like abetalipoproteinemia reinforce that rock-bottom cholesterol doesn't fry the brain. Bottom line: PCSK9 inhibitors stay safe and patient-friendly, with long-term eyes wide open [18, 26].
Cost Effectiveness of PCSK 9 Inhibitors
PCSK9 inhibitors' bang for the buck hinges on how well they work in targeted patient groups and how prices stack up across countries and insurance setups. Economic analyses zero in on folks with ASCVD and starting LDL-C of 70 mg/dL or higher, crunching incremental cost-effectiveness ratios (ICERs) against quality-adjusted life years (QALYs). FOURIER trial data flagged sky-high ICERs for evolocumab atop statins—needing a steep price slash to hit that $150,000-per-QALY sweet spot. Value climbs in patients who score bigger wins, like recent heart attack survivors, those with multivessel disease, or high Lp(a) levels. ODYSSEY Outcomes revealed alirocumab shining brightest in people kicking off at LDL-C 100 mg/dL or more, trimming major events and overall death rates enough to justify tailored pricing by risk tier. Bottom line: these drugs turn cost-effective in high-stakes crowds when prices drop. For MI patients ditching or dialing back statins, jacked-up hospital stays and costs rival PCSK9 bills. In primary prevention—say, familial hypercholesterolemia—a big discount could tip the scales toward routine use [18].
Future Directions
PCSK9 inhibitors have revolutionized heart risk management, sharpening the push in guidelines for aggressive LDL-C goals. While ramped-up statins and ezetimibe handle many cases, these drugs fill critical gaps for high-risk folks—though cost and access demand smart patient picks to maximize impact. Fresh options keep rolling out, like inclisiran—an siRNA that knocks down PCSK9 mRNA for half-year LDL-C control per shot—alongside vaccines, gene edits, and small molecules. Blockbuster trials (ORION-4, ODYSSEY OUTCOMES, FOURIER, SPIRE) probe lasting heart event cuts, with early wins showing deep LDL drops, plaque calming, and solid safety. European and U.S. nods for alirocumab and evolocumab broaden choices for familial hypercholesterolemia, mixed lipids, statin skippers, and ASCVD patients. Still, gaps linger: long-term safety, hard mortality wins, effect staying power, immune reactions, and value for money. As evidence builds and innovations ripen, PCSK9 blockers could mirror statins' path to everyday use [18,22,27].
CONCLUSION
PCSK9 inhibitors mark a game-changing leap in hyperlipidemia care, slashing LDL-C by blocking LDL receptor breakdown. Rock-solid genetic and trial data crown PCSK9 as prime target territory, with standouts like alirocumab, evolocumab, and inclisiran delivering deep, lasting drops that statins can't match alone. They shine brightest in high-risk cases, familial hypercholesterolemia, or statin no-gos, trimming cardiovascular threats while polishing other artery-unfriendly lipids—all with a clean long-term safety record.
REFERENCES


Ketaki Joshi*, Deepti Bandawane, “Pcsk 9 Inhibitors: A New Era in Hyperlipidemia”, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 2206-2215. https://doi.org/10.5281/zenodo.18333613
 10.5281/zenodo.18333613
10.5281/zenodo.18333613