Koringa College of Pharmacy, Korangi, Kakinada, Andhra Pradesh
Alzheimer’s disease (AD) is the most prevalent cause of dementia worldwide, posing immense medical, social, and economic challenges. Despite decades of research, pharmacological management has largely remained limited to symptomatic treatments, with cholinesterase inhibitors and NMDA receptor antagonists providing modest benefit. However, recent advances in understanding AD pathophysiology—particularly amyloid-? aggregation, tau pathology, neuroinflammation, and vascular contributions—have led to the development of disease-modifying therapies (DMTs). Monoclonal antibodies such as aducanumab, lecanemab, and donanemab have shown potential to slow cognitive decline, though challenges of safety, cost, and accessibility persist. Parallel research into anti-tau strategies, immunotherapies, multi-target drugs, and precision medicine approaches holds further promise. In addition to pharmacological interventions, non-pharmacological strategies—including lifestyle modifications, dietary interventions, physical activity, cognitive training, and psychosocial support—remain essential for holistic management of AD. Looking forward, advances in biomarker-guided therapy, stem cell research, gene editing, and artificial intelligence are shaping the future landscape of AD treatment. While curative therapies remain elusive, the convergence of pharmacological innovation with preventive and supportive strategies offers renewed hope for patients and caregivers. This review synthesizes current knowledge, highlights recent pharmacological advances, and explores future directions in the management of Alzheimer’s disease.
Alzheimer’s disease (AD) has emerged as one of the most pressing neurological disorders of the 21st century. First described in 1906 by Alois Alzheimer in a patient with profound memory loss, emotional instability, and neuropathological hallmarks of amyloid plaques and neurofibrillary tangles, the disease has since become a global health challenge. Currently, over 55 million individuals are living with dementia, of which 60–70% are attributable to AD¹. This number is projected to triple by 2050 due to aging populations, particularly in low- and middle-income countries².The burden of AD extends beyond patients to families, caregivers, and health systems. Annual global costs are estimated to exceed USD 1 trillion, with both direct medical expenses and indirect costs such as lost productivity and caregiver stress³. Importantly, AD is not merely a neurobiological condition but also a deeply human disease that strips individuals of memory, identity, and independence, creating emotional suffering for patients and loved ones.Pharmacological interventions, although essential, remain limited in their ability to halt or reverse disease progression. Current therapies primarily offer symptomatic relief, modestly improving cognition and daily functioning. However, recent scientific breakthroughs — including monoclonal antibodies targeting amyloid-β — represent a paradigm shift toward disease-modifying treatments?. Despite controversies, these innovations signal a hopeful transition from palliative symptom control to potentially altering the disease trajectory.This review aims to provide a comprehensive, detailed exploration of the pharmacological landscape of AD. It integrates historical context, molecular insights, current and emerging drug therapies, adjunctive approaches, and future directions. In doing so, it highlights not only scientific progress but also the urgent need for compassionate, patient-centered strategies that preserve dignity and quality of life.
2. Historical Background of Alzheimer’s Disease
The story of Alzheimer’s disease began in 1906, when Alois Alzheimer presented the case of Auguste Deter, a 51-year-old woman with progressive memory loss, paranoia, and cognitive decline. Upon her death, postmortem examination revealed hallmark neuropathological features — extracellular “senile plaques” and intracellular “neurofibrillary tangles.” These observations laid the foundation for identifying AD as a distinct neurodegenerative disorder¹.
Over the decades, advances in neuropathology, biochemistry, and genetics deepened understanding of the disease. In the 1970s, researchers highlighted the cholinergic deficit hypothesis, noting significant reductions in acetylcholine levels in AD patients. This led to the development of cholinesterase inhibitors, the first class of FDA-approved drugs for AD². The 1980s and 1990s brought two landmark discoveries: the amyloid cascade hypothesis, which proposed amyloid-β accumulation as a key driver of pathology, and the tau hypothesis, which focused on abnormal tau hyperphosphorylation and tangle formation³.
The late 1990s and early 2000s witnessed approval of memantine, an NMDA receptor antagonist, as well as large-scale clinical trials targeting amyloid-β. Despite repeated trial failures, these efforts shaped the modern research landscape. By the 2010s, genetic insights — particularly the role of the APOE ε4 allele — underscored the interplay between genes and environment?.
The 2020s marked a turning point with the controversial approval of aducanumab in 2021, followed by promising results for lecanemab and donanemab. For the first time, therapies aimed not just to relieve symptoms but to modify the underlying disease process?. Though debates continue regarding efficacy, safety, and affordability, these approvals represent historic milestones in the century-long fight against AD.
Table 1: Key Historical Milestones in Alzheimer’s Disease Research
|
Year |
Milestone |
Impact |
|
1906 |
Alois Alzheimer describes plaques & tangles in Auguste Deter |
First identification of AD pathology |
|
1970s |
Cholinergic hypothesis proposed |
Led to development of cholinesterase inhibitors |
|
1984 |
Amyloid-β protein identified |
Foundation of amyloid cascade hypothesis |
|
1986 |
Tau protein abnormalities described |
Birth of tau hypothesis |
|
1993 |
APOE ε4 identified as genetic risk factor |
Opened doors to pharmacogenomics research |
|
1996–2003 |
Donepezil, rivastigmine, galantamine, and memantine approved |
First pharmacological treatments for AD |
|
2021 |
Aducanumab FDA approval |
First disease-modifying therapy (controversial) |
|
2023 |
Lecanemab& donanemab trials show positive outcomes |
Renewed hope for disease modification |
3. Epidemiology, Burden, and Risk Factors
Alzheimer’s disease (AD) is the leading cause of dementia, accounting for 60–70% of cases worldwide¹. According to the World Health Organization, more than 55 million people live with dementia in 2023, a number projected to rise to 139 million by 2050 due to aging populations². This makes AD not only a medical challenge but also a global public health crisis.
3.1 Global Prevalence
Prevalence rates vary significantly across regions. In North America and Europe, where life expectancy is higher, prevalence of AD in individuals above 65 years ranges from 5–8%. In Asia, rapid aging, especially in China and India, is expected to contribute to a majority of global dementia cases by mid-century³. Meanwhile, in Africa and low-income countries, prevalence data remain limited, but underdiagnosis is common due to poor healthcare infrastructure?.
3.2 Socioeconomic Burden
The economic burden of AD is staggering. The global cost of dementia was estimated at over USD 1 trillion in 2020 and is expected to double by 2030?. Direct medical costs include diagnosis, hospitalizations, and medications, while indirect costs include caregiver time, lost productivity, and social support. Importantly, up to 80% of dementia care is provided by unpaid family caregivers, leading to financial strain, emotional exhaustion, and health issues?.

Figure-1
3.3 Risk Factors
AD arises from a complex interplay of non-modifiable and modifiable risk factors.
Table 2: Global Prevalence and Burden of Alzheimer’s Disease
|
Region |
Prevalence in ≥65 years |
Estimated Patients (2023) |
Projected Patients (2050) |
Notes |
|
North America |
6–8% |
~7 million |
~14 million |
High healthcare expenditure, advanced diagnostics |
|
Europe |
6–7% |
~10 million |
~18 million |
Aging population, high prevalence in women |
|
Asia |
4–6% |
~22 million |
~70 million |
Rapid demographic shift, underdiagnosis in rural areas |
|
Africa |
2–4% |
~4 million |
~10 million |
Data gaps, limited resources |
|
Global |
~5–7% |
~55 million (all dementias) |
~139 million |
Major economic and social burden |
4. Pathophysiology of Alzheimer’s Disease
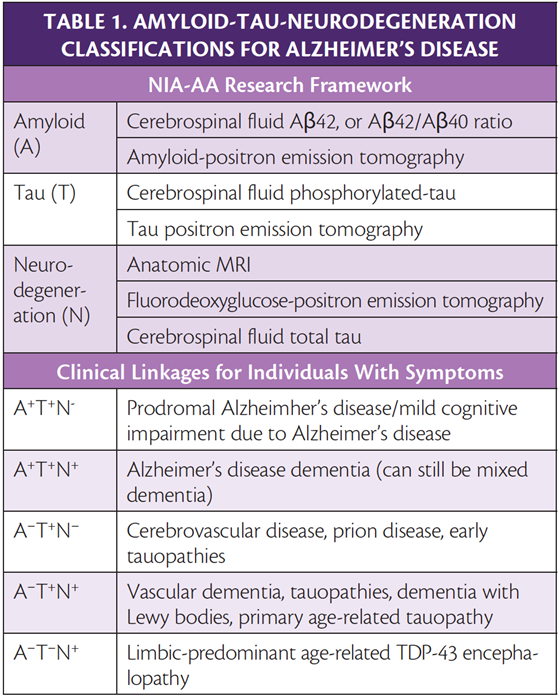
Alzheimer’s disease (AD) is characterized by progressive neurodegeneration involving multiple molecular and cellular pathways. While the amyloid cascade and tau hypotheses remain central, it is now understood that AD arises from a multifactorial process involving oxidative stress, mitochondrial dysfunction, neuroinflammation, synaptic failure, and even systemic factors such as metabolic dysfunction and the gut–brain axis¹.
4.1 Amyloid Cascade Hypothesis
The amyloid cascade hypothesis suggests that the overproduction or impaired clearance of amyloid-β (Aβ) peptides, derived from amyloid precursor protein (APP), leads to extracellular plaque accumulation². Oligomeric forms of Aβ are considered highly neurotoxic, disrupting synaptic transmission, inducing oxidative stress, and triggering neuroinflammatory responses³.
Key evidence supporting this hypothesis comes from genetic studies: mutations in APP, presenilin-1, and presenilin-2 genes (familial AD) result in increased Aβ production?. In sporadic AD, impaired clearance mechanisms, including reduced proteolytic degradation and dysfunction of the glymphatic system, contribute to accumulation?.
4.2 Tau Pathology
Tau is a microtubule-associated protein that stabilizes neuronal structure. In AD, tau undergoes abnormal hyperphosphorylation, leading to its detachment from microtubules and aggregation into **neurofibrillary tangles (NFTs)**?. This process disrupts axonal transport, causes cytoskeletal collapse, and contributes to synaptic dysfunction?.
Unlike amyloid pathology, tau deposition correlates more strongly with disease severity and cognitive decline?. Recent therapeutic efforts are increasingly focused on targeting tau aggregation and its spread across neural networks.
4.3 Neuroinflammation
Microglial activation plays a dual role in AD. While microglia initially aid in clearing Aβ aggregates, chronic activation leads to excessive release of cytokines, chemokines, and reactive oxygen species?. Genome-wide association studies (GWAS) have identified risk genes such as TREM2, highlighting the contribution of innate immunity to AD¹?.
Astrocytes also contribute to inflammation and blood–brain barrier dysfunction, further exacerbating neurodegeneration¹¹.
4.4 Oxidative Stress and Mitochondrial Dysfunction
Oxidative damage is one of the earliest events in AD pathology. Aβ accumulation leads to excessive production of reactive oxygen species (ROS), lipid peroxidation, and DNA damage¹². Mitochondrial dysfunction, characterized by impaired ATP generation and altered calcium homeostasis, contributes to synaptic failure and neuronal apoptosis¹³.
4.5 Synaptic Dysfunction and Neurotransmitter Deficits
Loss of synapses is the strongest correlate of cognitive impairment in AD¹?. Disruptions in glutamatergic and cholinergic signaling underlie memory deficits and behavioral changes. Reduced levels of acetylcholine form the basis of the cholinergic hypothesis, leading to the development of cholinesterase inhibitors as symptomatic treatments¹?.
4.6 Metabolic Dysfunction and “Type 3 Diabetes”
Recent evidence suggests AD may share mechanisms with metabolic disorders. Insulin resistance in the brain impairs glucose utilization, leading to neuronal energy deficits. Some researchers describe AD as a “Type 3 diabetes” due to overlapping pathways involving insulin signaling and amyloid accumulation¹?.
4.7 Gut–Brain Axis and Microbiome
Emerging studies highlight the role of gut microbiota in AD. Dysbiosis may increase systemic inflammation and alter amyloid deposition¹?. Preclinical data suggest that probiotics and dietary interventions modulate neuroinflammation and cognitive outcomes, though human evidence remains limited¹?.
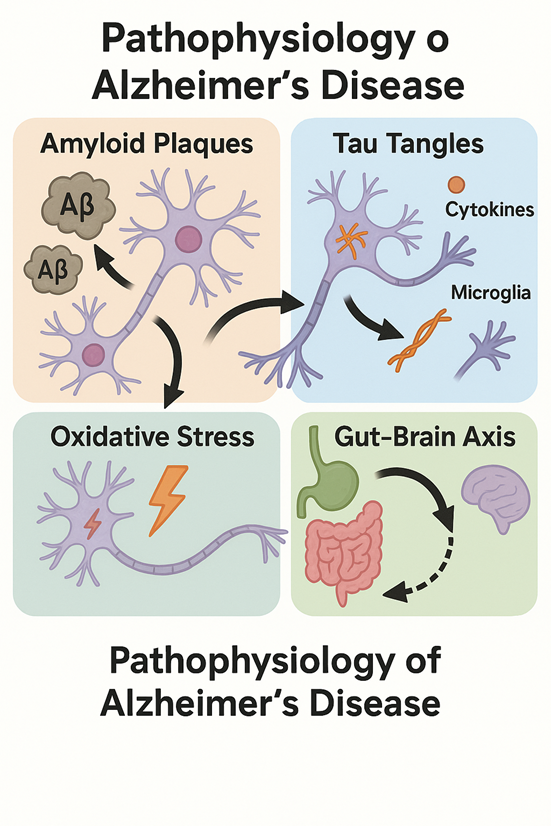
Figure-2
Table 3: Major Pathophysiological Mechanisms in Alzheimer’s Disease
|
Mechanism |
Key Features |
Impact on AD |
|
Amyloid cascade |
Aβ overproduction, impaired clearance |
Plaque formation, synaptic toxicity |
|
Tau pathology |
Hyperphosphorylation, NFTs |
Axonal damage, strong correlation with cognition |
|
Neuroinflammation |
Microglial & astrocytic activation |
Chronic inflammation, cytokine release |
|
Oxidative stress |
ROS production, lipid peroxidation |
DNA damage, neuronal apoptosis |
|
Mitochondrial dysfunction |
Impaired ATP production |
Synaptic failure, cell death |
|
Synaptic dysfunction |
Loss of glutamatergic & cholinergic signaling |
Cognitive decline |
|
Metabolic dysfunction |
Brain insulin resistance |
“Type 3 diabetes,” neuronal energy deficit |
|
Gut–brain axis |
Microbiome dysbiosis |
Systemic inflammation, amyloid changes |
5. Current Pharmacological Therapies in Alzheimer’s Disease
Despite decades of research, the pharmacological options for Alzheimer’s disease (AD) remain limited. Current therapies primarily provide symptomatic relief by enhancing neurotransmission or modulating excitotoxic pathways, but they do not halt disease progression¹.
5.1 Cholinesterase Inhibitors
The cholinergic hypothesis posits that memory impairment in AD is partly due to loss of cholinergic neurons and reduced acetylcholine levels in the basal forebrain². Cholinesterase inhibitors (ChEIs) prolong acetylcholine action by inhibiting its breakdown, thereby improving neurotransmission.
Common side effects include nausea, vomiting, diarrhea, bradycardia, and weight loss. Clinical benefits often diminish after 12–18 months of therapy.
5.2 NMDA Receptor Antagonist
Excitotoxicity via glutamate overstimulation contributes to neuronal injury in AD. Memantine, an NMDA receptor antagonist, is approved for moderate-to-severe AD?. It reduces abnormal glutamatergic activity without disrupting normal synaptic signaling.
Memantine is often combined with donepezil, and clinical studies demonstrate modest improvements in cognition, daily function, and caregiver burden?.
5.3 Combination Therapy
Combining ChEIs with memantine is increasingly common in moderate-to-severe stages. Evidence suggests additive or synergistic effects, though long-term outcomes remain uncertain?.
5.4 Symptomatic Management of Behavioral and Psychological Symptoms
AD patients often develop agitation, psychosis, sleep disturbances, and depression. These symptoms significantly affect quality of life and caregiver stress. Pharmacological options include:
These treatments are symptomatic and must be used with caution, emphasizing the need for safer, more effective drugs.
5.5 Limitations of Current Therapies
Although widely used, current pharmacological treatments offer only modest symptomatic benefit without altering the underlying disease process. Decline in cognition and function continues despite therapy. Side effects, poor tolerability, and diminishing efficacy further limit utility. These shortcomings highlight the urgent need for disease-modifying therapies (DMTs).
Table 4: Currently Approved Pharmacological Therapies in Alzheimer’s Disease
|
Drug/Class |
Mechanism of Action |
Indication |
Clinical Benefits |
Limitations/Side Effects |
|
Donepezil |
Reversible AChE inhibitor |
Mild– severe AD |
Improves cognition, daily function |
GI upset, bradycardia, weight loss |
|
Rivastigmine |
Inhibits AChE&BuChE |
Mild– moderate AD, Parkinson’s dementia |
Cognitive benefit, patch improves compliance |
GI side effects, dizziness |
|
Galantamine |
AChE inhibitor + nicotinic receptor modulator |
Mild– moderate AD |
Dual action, mild functional improvement |
Nausea, vomiting |
|
Memantine |
NMDA receptor antagonist |
Moderate– severe AD |
Reduces excitotoxicity, caregiver relief |
Dizziness, headache, constipation |
|
Combination (Donepezil + Memantine) |
Cholinesterase inhibition + NMDA modulation |
Moderate– severe AD |
Additive effects, modest benefit |
Still symptomatic, cost |
|
Antidepressants (SSRIs/SNRIs) |
Increase serotonin/norepinephrine |
Depression, anxiety in AD |
Mood improvement |
Sedation, GI upset |
|
Antipsychotics |
Dopamine/serotonin antagonists |
Agitation, psychosis |
Short-term control of BPSD |
Stroke risk, mortality |
6. Recent Advances: Disease-Modifying Therapies in Alzheimer’s Disease
The approval of aducanumab in 2021 marked a turning point in Alzheimer’s disease (AD) pharmacology, representing the first agent designed to alter disease progression rather than provide symptomatic relief¹. Since then, multiple disease-modifying therapies (DMTs), particularly monoclonal antibodies targeting amyloid-β (Aβ), have entered late-stage clinical development. Despite optimism, challenges remain regarding efficacy, safety, and accessibility.
6.1 Anti-Amyloid Monoclonal Antibodies
6.1.1. Aducanumab (Aduhelm)
6.1.2. Lecanemab (Leqembi)
6.1.3. Donanemab
6.1.4. Other Antibodies in Development
6.2 Anti-Tau Therapies
Given the strong correlation between tau pathology and cognitive decline, tau-targeting therapies are increasingly prioritized.
6.3 Active and Passive Immunotherapies (Vaccines)
Immunotherapy approaches aim to stimulate the immune system to clear amyloid or tau.
6.4 Small Molecule Disease-Modifying Approaches
Beyond biologics, small molecules offer practical advantages (oral route, lower cost).
6.5 Combination and Multi-Target Therapies
Given the multifactorial nature of AD, researchers are testing combinations of anti-amyloid, anti-tau, and anti-inflammatory agents. Multi-targeted approaches may provide synergistic effects by addressing overlapping pathological pathways¹¹.
Table 5: Recent Clinical Trials of Disease-Modifying Therapies (2020–2024)
|
Drug |
Target |
Trial/Phase |
Outcome |
Status |
|
Aducanumab |
Aβ aggregates |
EMERGE/ENGAGE (Phase III) |
Mixed results, plaque reduction, modest benefit |
FDA approved (2021) |
|
Lecanemab |
Aβ protofibrils |
CLARITY-AD (Phase III) |
27% slowing of decline, ARIA risk lower than aducanumab |
FDA approved (2023/2024) |
|
Donanemab |
Pyroglutamate Aβ |
TRAILBLAZER-ALZ2 (Phase III) |
35% slowing in decline, positive biomarker changes |
Pending approval |
|
Gantenerumab |
Aβ fibrils |
GRADUATE I/II (Phase III) |
Failed to meet endpoints |
Development halted (2022) |
|
Semorinemab |
Tau |
LAURIET (Phase II) |
No cognitive benefit |
Ongoing studies |
|
AADvac1 |
Tau vaccine |
Phase II |
Safe, immunogenic, modest benefit |
Investigational |
7. Adjunctive and Non-Pharmacological Strategies
While pharmacological therapies are essential in managing Alzheimer’s disease (AD), adjunctive and lifestyle-based interventions are equally critical. They address comorbidities, enhance quality of life, and often reduce the rate of functional decline¹.
7.1 Lifestyle Interventions
7.1.1. Dietary Modifications
7.1.2. Physical Activity
7.2 Cognitive and Social Engagement
7.3 Psychological and Behavioral Support
7.4 Assistive Technology and Digital Tools
Table 6: Evidence-Based Non-Pharmacological Interventions in AD
|
Intervention |
Mechanism |
Clinical Evidence |
Impact |
|
Mediterranean/ MIND Diet |
Antioxidants, anti-inflammatory, improved vascular health |
Observational + RCTs |
Slows progression, lowers risk |
|
Aerobic Exercise |
Enhances neurogenesis, synaptic plasticity |
Multiple RCTs |
Improves cognition, mood, daily function |
|
Cognitive Training |
Stimulates neuroplasticity |
Clinical trials |
Improves memory, attention |
|
Social Engagement |
Reduces isolation, depression |
Observational studies |
Better emotional resilience |
|
Music/Art Therapy |
Emotional arousal, preserved non-verbal communication |
Case series, small RCTs |
Improves mood, reduces agitation |
|
Caregiver Training |
Stress reduction, structured routines |
RCTs + meta-analyses |
Improves caregiver well-being |
8. Future Directions and Challenges in Alzheimer’s Disease Pharmacology
Despite major advances, effective and widely accessible treatments for Alzheimer’s disease (AD) remain elusive. Ongoing research is pushing boundaries in molecular medicine, genetics, regenerative therapies, and digital health. At the same time, multiple challenges—scientific, ethical, and socioeconomic—must be addressed before breakthroughs translate into population-wide benefits.
8.1 Precision Medicine and Biomarker-Guided Therapy
8.2 Regenerative Medicine and Stem Cell Therapy
8.3 Gene Therapy and Genome Editing
8.4 Multi-Target Drug Discovery
8.5 Digital Health and Artificial Intelligence
8.6 Global and Societal Challenges
Table 7: Future and Emerging Approaches in AD Therapy
|
Approach |
Rationale |
Current Status |
Challenges |
|
Biomarker-guided precision therapy |
Patient stratification, early detection |
Plasma biomarkers in late validation |
Cost, implementation in primary care |
|
Stem cell therapy |
Neuronal replacement, synaptic repair |
Early-stage trials |
Integration, ethics, tumorigenicity |
|
Gene therapy / CRISPR |
Modify risk genes, enhance protective proteins |
Preclinical & early human studies |
Safety, delivery |
|
Multi-target drugs |
Address multifactorial pathology |
Computational models, preclinical |
Complex pharmacokinetics |
|
AI & Digital Health |
Early diagnosis, remote monitoring |
Pilot programs, start-ups |
Privacy, bias, accessibility |
CONCLUSION
Alzheimer’s disease (AD) remains one of the greatest challenges of modern medicine, with devastating personal, social, and economic consequences. Despite decades of research, truly curative treatments remain elusive. The past two decades have seen remarkable advances in understanding its complex pathophysiology—ranging from amyloid-β and tau pathology to the roles of neuroinflammation, oxidative stress, and vascular contributions. This deeper insight has paved the way for novel therapeutic strategies that go beyond symptomatic relief.
The recent approval of monoclonal antibodies such as aducanumab and lecanemab has been heralded as a milestone, signaling the possibility of disease modification. Yet, controversies around cost, safety, and modest efficacy remind us that these breakthroughs are only the beginning. Future research must not only focus on enhancing efficacy but also on improving accessibility and equity, especially in low- and middle-income countries where the burden of dementia is rising fastest.At the same time, non-pharmacological interventions—including diet, exercise, cognitive training, and psychosocial support—remain indispensable in patient-centered care. Their integration with pharmacological therapy exemplifies the growing shift toward multimodal treatment strategies. Moreover, the incorporation of digital health technologies, artificial intelligence, and biomarker-guided precision medicine represents a paradigm shift in both clinical practice and research.Looking forward, stem cell and gene therapies, polypharmacology, and AI-assisted discovery hold the potential to transform the therapeutic landscape. However, these innovations must be pursued with caution, ensuring safety, ethical oversight, and global accessibility.In summary, the pharmacology of Alzheimer’s disease is entering a new era of optimism tempered by realism. While immediate cures remain out of reach, the convergence of advanced pharmacological research, lifestyle interventions, and technological innovation offers hope that future generations may not only live longer but also live free from the devastating impact of Alzheimer’s disease.Alzheimer’s disease; pharmacology; disease-modifying therapies; amyloid; tau; biomarkers; neuroinflammation; precision medicine; stem cells; non-pharmacological interventions; dementia management.Alzheimer’s disease; pharmacology; disease-modifying therapies; amyloid; tau; biomarkers; neuroinflammation; precision medicine; stem cells; non-pharmacological interventions; dementia management.
REFERENCES


R. Pravallika Sai Sri, K. Sunitha, Pharmacological Approaches in Alzheimer’s Disease: From Symptomatic Care to Future Disease Modification, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 3561-3576. https://doi.org/10.5281/zenodo.17227400
 10.5281/zenodo.17227400
10.5281/zenodo.17227400
